
Abstract
Background:
Women with non-ST elevation myocardial infarction (NSTEMI) have similar extent of myocardial ischemia but less obstructive coronary artery disease (CAD) than their male counterparts. We tested the impact of global coronary artery plaque area and artery tortuosity on myocardial perfusion in NSTEMI patients.
Methods:
Coronary artery plaque area was determined by quantitative angiography in 108 patients (32% women) with NSTEMI. Myocardial perfusion was assessed by contrast echocardiography in the 17 individual left ventricular segments. Artery tortuosity was defined as ≥3 curves >45° in a main coronary artery.
Results:
Age, prevalence of hypertension, and diabetes did not differ between sexes (all nonsignificant). Women had lower prevalence of ≥50% coronary artery stenosis (74% vs. 91%, p<0.05), while global coronary plaque area (35±22 vs. 43±21mm2) and the number of segments with hypoperfusion (6.9±3.7 vs. 7.2±3.4) did not differ between sexes (both p>0.07). In multivariate analysis, larger coronary artery plaque area was associated with a 35% higher risk for having severe myocardial hypoperfusion (odds ratio 1.35 [95% confidence interval 1.01–1.80], p<0.05) in the total study population, while no association between artery tortuosity and myocardial ischemia was found. Similar results were obtained in separate analysis among women and men.
Conclusion:
In women and men with NSTEMI, the global coronary artery plaque area was an important determinant of the severity of myocardial hypoperfusion at rest independent of presence of significant coronary stenoses. These findings may expand current understanding of NSTEMI in patients with nonobstructive CAD.
Introduction
S
Previous studies using contrast echocardiography or cardiac magnetic resonance imaging have demonstrated that ischemic burden measured by these techniques is an important prognosticator in particular in women with nonobstructive CAD. 10,11 In a smaller study, we recently demonstrated that the extent of myocardial hypoperfusion in patients with non-ST elevation myocardial infarction (NSTEMI) was comparable in women and men despite less obstructive CAD in women. 7 However, it is not clear whether coronary artery plaque area may influence myocardial perfusion in NSTEMI patients independent of presence of significant coronary artery stenoses. Furthermore, others have suggested that also artery tortuosity may influence coronary perfusion. 9 The aim of this study was therefore to explore if coronary plaque area and arterial tortuosity impacted myocardial perfusion in NSTEMI patients, and thereby could explain the mismatch between extent of myocardial hypoperfusion and presence of significant CAD previous reported in NSTEMI women.
Materials and Methods
Study population
A total of 126 consecutive patients diagnosed with acute NSTEMI, defined as the combination of chest pain and troponin T elevation, hospitalized at the Department of Heart Disease, Haukeland University Hospital, from March through December 2008 and scheduled for acute coronary angiography within 72 hours after admittance were eligible for the study. Excluding patients with hemodynamically unstable disease, mechanical valve prostheses or severe pulmonary disease, a total of 110 patients signed informed consent and all of them underwent myocardial contrast echocardiography prior to scheduled coronary angiography. 12
For the present post-hoc analysis, reanalyzing the angiograms in this previous series with quantitative coronary angiography, two of the 110 patients were excluded because all native coronary arteries were occluded, leaving 108 patients for the present study population. Clinical risk assessment was performed in all patients using the thrombolysis in myocardial infarction (TIMI) risk score model. 13 The study was approved by the regional ethical committee and performed in accordance with the Helsinki declaration.
Quantitative coronary angiography
Quantitative coronary angiography was performed offline by a single reader (IE) blinded to clinical data and myocardial perfusion assessment using a digitalized automatic edge detecting analysis software (QAngio® XA 7.1, MEDIS Medical Imaging Systems, Leiden, The Netherlands) (Fig. 1, panel A).
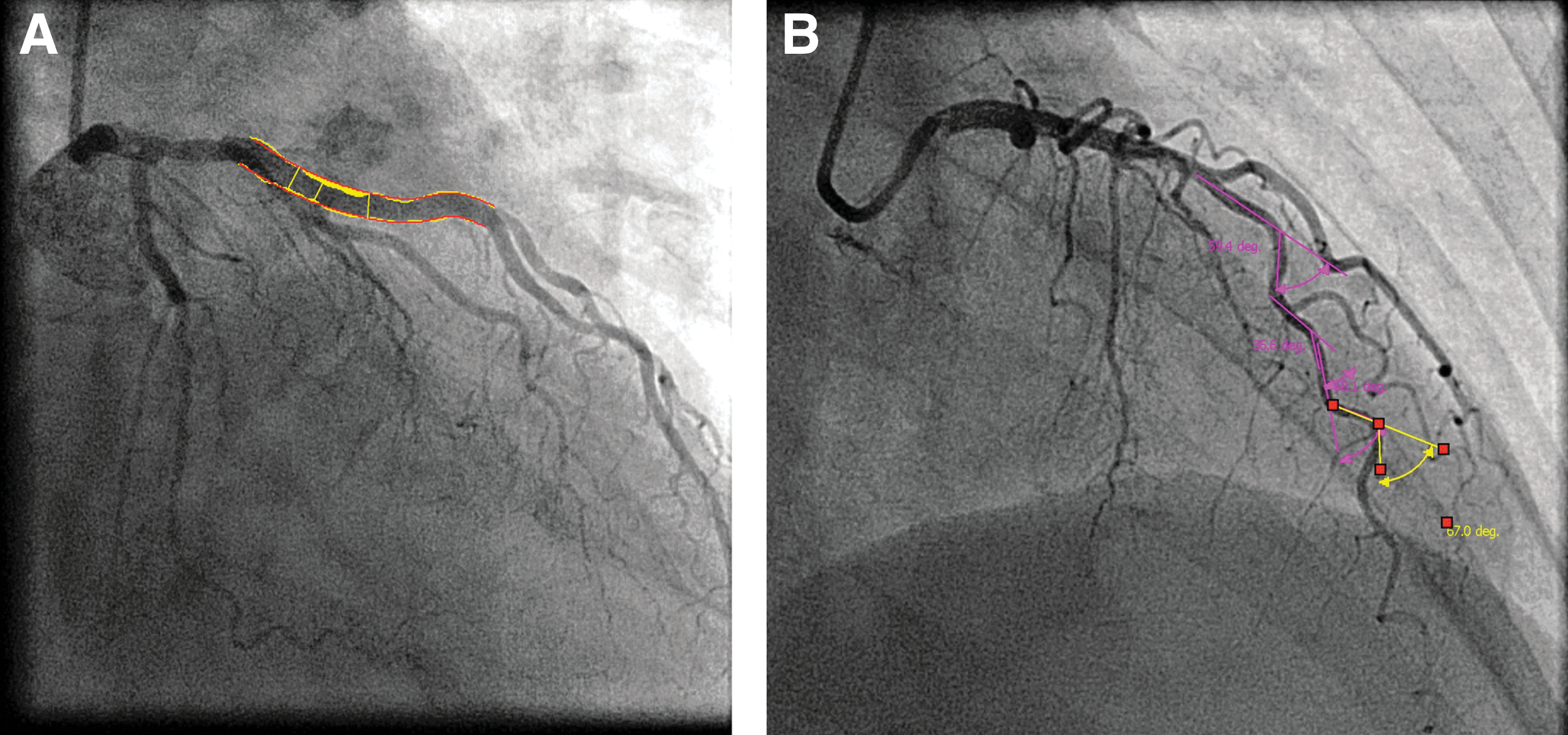
Quantitative coronary angiography. Coronary artery plaque area
The coronary artery tree was divided into 17 segments, following the modified American Heart Association model. 14 The tip of the catheter was used for calibration. Stenosis severity and plaque area assessed as lumen diameter reduction was determined in all vessel segments with a diameter >1.5 mm. Global coronary artery plaque area was calculated as the sum of plaque area in all segments. A coronary artery lumen diameter reduction of ≥50 % on the angiogram was considered a significant stenosis.
Coronary artery tortuosity was measured in the three main coronary arteries in standardized views: The left anterior descending artery in the right anterior oblique view with cranial angulation, the left circumflex artery in the left anterior oblique with caudal angulation and the right coronary artery in the right anterior oblique view. 9 Coronary tortuosity was regarded present if ≥3 curves >45° was found in the same artery (Fig. 1, panel B).
Echocardiography
Quantitative echocardiography was performed following the joint European Association of Echocardiography and American Society of Echocardiography guidelines. 15 Left ventricular (LV) ejection fraction was assessed by the modified biplane Simpson formula and regional LV function by wall motion scoring. 15 Wall motion score was assessed in apical 2-, 3-, and 4-chamber views using a 17-segment LV model as recommended in current quantitation guidelines. 15 The average wall motion score value was taken as wall motion score index in the individual patients. Methods and results from myocardial contrast echocardiography have previously been reported in details. 7,12 In short, myocardial contrast echocardiography was performed at rest by real-time low-mechanical index imaging and destruction–replenishment using Cadance Contrast Pulse Sequencing technology (Acuson Sequoia C512, Siemens, Mountain View, CA, echocardiograph). An intravenous bolus dosage of 0.3 mL Perflutren Lipid Microsphere ultrasound contrast (Luminity®, Lantheus Medical Imaging, North Billerica, MA) was given before perfusion imaging. The bolus dosage was repeated if necessary to ensure a stable contrast concentration and avoid contrast swirling during image acquisition. Regional myocardial perfusion was scored visually as normal (contrast replenishment within five heart beats) or hypoperfusion (delayed contrast replenishment after more than five heart beats) using the guideline-recommended 17 segment LV model (Fig. 2). 15,16 The extent of myocardial perfusion abnormalities was assessed as the number of segments with hypoperfusion. Severe myocardial hypoperfusion was considered present if hypoperfusion was detected in ≥6 LV segments. 12
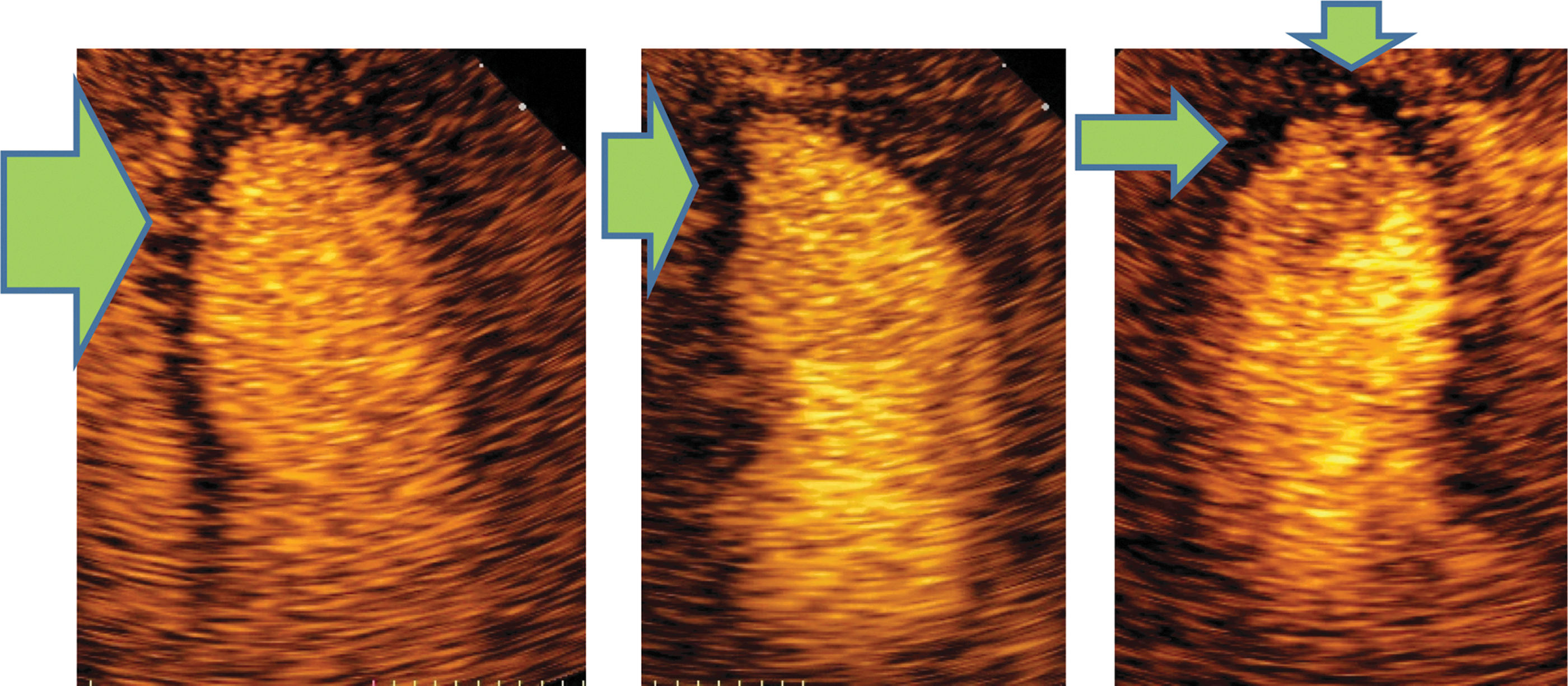
Myocardial contrast echocardiography. Apical 4-chamber, 2-chamber and long axis view images taken five beats post flash demonstrating subendocardial and transmural hypoperfusion in the apical left ventricular segments marked with green arrows.
Statistics
Data management and statistical analysis were performed by the IBM SPSS statistical program version 20.0 (IBM SPSS, Chicago, IL). The study had 80% power to detect a 30% difference in coronary artery stenosis between women and men at a statistical level of 0.05. Continuous variables are reported as mean and standard deviation and categorical variables as numbers and percentages. Comparisons between groups were performed by unpaired t-test or chi-squared statistics as appropriate. Covariates of global coronary artery plaque area and tortuosity were identified by Pearson's correlation coefficient and logistic regression analysis as appropriate. Independent covariates of the extent of myocardial hypoperfusion were identified in multiple linear regression analysis. Covariates of severe hypoperfusion (involving ≥6 LV segments) were identified in multiple logistic regression analysis. The associations of presence of severe myocardial hypoperfusion with global coronary artery plaque area and presence of significant coronary artery stenosis were tested in receiver operator characteristics curve analysis. A p value <0.05 was considered statistical significant. The intraobserver variability of myocardial perfusion assessment and of coronary artery plaque area measurement was calculated separately from echocardiographic and angiographic images, respectively, in 11 patients analyzed twice and reported as intraclass correlation coefficient.
Results
Patient characteristics
The proportion of patients >65 years of age was significantly higher among women, while mean age, troponin T levels and TIMI risk score did not differ between women and men (Table 1). There were no sex differences in anti-ischemic treatment at study entrance. None of the women were on hormone replacement therapy. The extent of wall motion abnormalities and myocardial hypoperfusion did not differ between women and men, reflecting comparable myocardial infarct size (Table 2). The mean time between contrast echocardiography and angiography was 1.87±2.6 days, with a median of 1.0 day. There were no adverse events from contrast infusions, except for three patients who experienced transient lower back pain.
BMI, body mass index; CAD, coronary artery disease; TIMI, thrombolysis in myocardial infarction risk score.
LV, left ventricular.
Coronary artery plaque area
A total of 35 main arteries had proximal total occlusion. From the total of 1422 coronary artery segments visible on the angiograms, 69 segments were excluded from analysis due to poor image quality and vessel overlap, and another 170 segments were excluded due to luminal diameter ≤1.5 mm, which cannot be analyzed with our method, leaving a total of 1252 (88% of visible segments on the angiogram) for assessment of coronary artery plaque area.
Reproducibility of myocardial perfusion score by intraclass correlation coefficient was 0.95 (95% confidence interval [CI] 0.90–0.98) and for coronary artery plaque area 0.86 (95% CI 0.75–0.91).
Global coronary artery plaque area did not differ significantly between women and men despite lower prevalence of significant coronary artery stenoses and multivessel disease in women (Table 2). In receiver operating characteristic curve analysis, global coronary artery plaque area was significantly associated with having severe myocardial hypoperfusion in both women and men, while presence of significant coronary artery stenosis was significantly associated with severe myocardial hypoperfusion only in women, probably reflecting the low prevalence of nonobstructive CAD in men (Fig. 3).
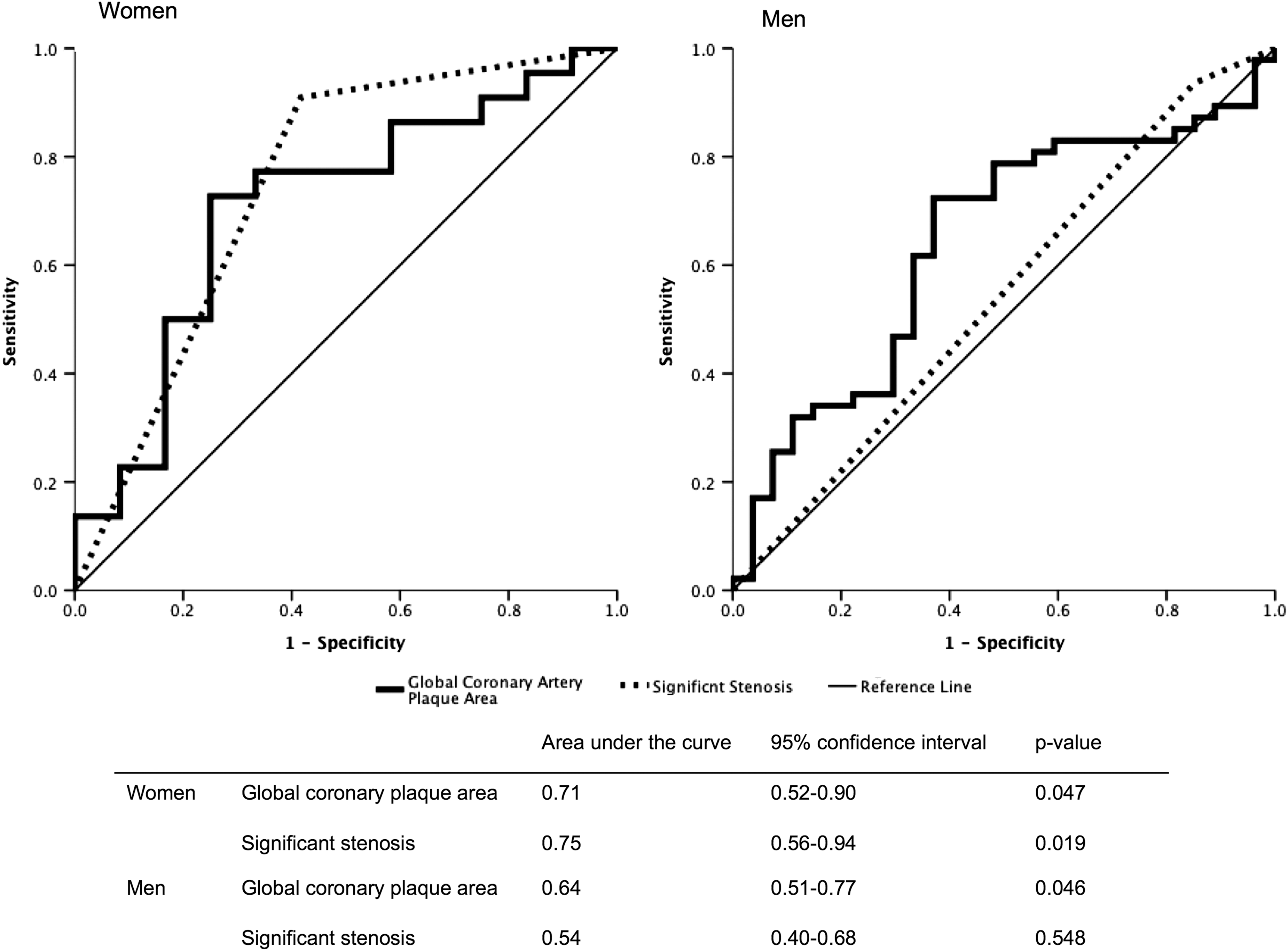
Global coronary artery plaque area and severe myocardial hypoperfusion. Receiver operating curve analysis of the univariate association of presence of severe myocardial hypoperfusion with global coronary plaque area and presence of significant coronary artery stenosis in women and men.
Coronary artery tortuosity
A total of 273 native main coronary arteries were visible on the coronary angiograms. Of these, 34 were excluded due to low image quality, leaving 239 (88%) available for analysis of tortuosity. All three main coronary arteries could be assessed in 65 patients, two in 31 patients, and one in 7 patients. Tortuosity was more prevalent among women than men (Table 3). Global coronary artery plaque area did not differ between patients with tortuous and non-tortuous coronary arteries (42.0±23.5 vs. 38.0±17.4 mm2, p=0.367). Tortuosity was not associated with the extent of myocardial hypoperfusion in the total study population or in men and women analyzed separately.
95% CI, 95% confidence interval; OR, odds ratio.
Determinants of myocardial hypoperfusion
A significant association was found between global coronary plaque area and both severity and extent of myocardial hypoperfusion in univariate analyses (both p<0.05) (Tables 3, 4). In multiple logistic regression analysis, adjusting for known confounders of hypoperfusion, a 10 mm2 higher global plaque area was associated with a 35% higher risk for having severe myocardial hypoperfusion on the echocardiogram (odds ratio 1.35; 95% CI 1.01–1.80, p=0.047), independent of presence of significant coronary artery stenosis (Table 3). However, the association of larger global coronary plaque area with larger extent of myocardial hypoperfusion was attenuated and became borderline statistically significant when adjusted for confounders in multivariate analysis (β=0.18, p=0.057) (Table 4).
VIF, variance inflation factor.
Discussion
The present study demonstrates that global coronary artery plaque area is an important determinant of the severity of myocardial hypoperfusion in NSTEMI patients, independent of presence of significant coronary artery stenoses. Of note, global coronary artery plaque area did not differ between sexes despite lower prevalence of obstructive CAD in women. In fact, nonobstructive CAD was nearly 3-fold more prevalent in women than in men in the present study, in accordance with previous reports from registries and meta-analyses. 5,6 Although computer tomography coronary angiography is recognized as a superior method for assessment of coronary artery plaque area, invasive coronary angiography is the preferred diagnostic technique for diagnosis of CAD in current management guidelines for NSTEMI patients. 17 Therefore, our findings are relevant for clinical practice.
Distinct sex differences in coronary atherosclerosis are well described. 2 Typically, women have more diffuse atherosclerosis, smaller arteries and more microvascular involvement. 2,18 These factors may contribute to the reported sex difference in treatment procedures and outcome among CAD patients. 19,20 Intravascular ultrasound in women with chest pain and nonobstructive CAD has demonstrated a high prevalence of atherosclerosis with positive remodeling and preserved lumen size. 21,22 This emphasizes the limitation of the present study using angiography to estimate the coronary artery plaque area, since only the luminal narrowing is visualized on the angiogram. In addition, it was not possible to measure plaque area in coronary arteries <1.5 mm in diameter with our method. Consequently, global coronary artery plaque area may have been underestimated, in particular in women in our study, due to the combination of more positive remodeling and smaller coronary artery diameter. Furthermore, angiographic normal reference segments often contain mild to moderate diffuse atherosclerosis, possibly leading to an underestimation of the true lumen diameter, and thereby of the plaque area. 23 Still, as demonstrated, reproducibility of global coronary plaque area measurement by our method was good.
The prognostic importance of the ischemic burden assessed by contrast echocardiography at rest has been documented in patients with acute chest pain. 11,24 The use of contrast stress echocardiography in assessment of CAD risk in menopausal women is currently under evaluation. 25 In patients with myocardial infarction, larger extent of myocardial hypoperfusion by contrast echocardiography at rest has been demonstrated to predict unfavorable LV remodeling and impaired prognosis. 24,26 Similarly, previous studies assessing myocardial perfusion by magnetic resonance imaging have reported increased morbidity, in particular hospitalizations for angina pectoris, in women with chest pain and nonobstructive CAD. 10,27 Consequently, extent and severity of the perfusion abnormalities are important prognosticators in patients with different types of acute coronary syndromes.
It was recently demonstrated in a numerical simulation study that coronary artery tortuosity may induce myocardial ischemia through a reduction in coronary artery perfusion pressure. 28 Typically, coronary artery tortuosity is more prevalent in women and in patients with hypertension. 9 In this study, tortuosity was indeed more prevalent in women, but not associated with hypertension. Coronary artery tortuosity was not associated with myocardial hypoperfusion at rest neither in women nor men. Thus, the clinical relevance of coronary tortuosity in NSTEMI remains to be established.
Finally, endothelial dysfunction, vessel inflammation and microvascular disease may all contribute to myocardial hypoperfusion in NSTEMI patients with nonobstructive CAD beyond the global coronary artery plaque area. 2,29,30 However, these factors were not measured in the present study. On the other hand, hypertension and diabetes, comorbidities known to be associated with endothelial dysfunction did not differ between women and men, and also did not predict the extent of myocardial hypoperfusion in the present study. 31
Conclusions
In women and men with NSTEMI, the global coronary artery plaque area was an important determinant of the severity of myocardial hypoperfusion at rest independent of presence of significant coronary stenoses. These findings may expand current understanding of NSTEMI in patients with nonobstructive CAD.
Footnotes
Author Disclosure Statement
No competing financial interests exist.