
Abstract
Background:
Co-administration of multiple intravenous drugs via the Y-site is common in palliative care. Information on the compatibility of opioid analgesics with intravenous drugs commonly used in palliative care is lacking.
Objective:
We aimed to determine the physical compatibility of 4 opioid analgesics with 64 drugs during simulated Y-site administration.
Design:
Four opioid analgesics and intravenous drugs were prepared using 0.9% sodium chloride solution or water for injection, without dilution, according to the manufacturer’s recommendations (morphine hydrochloride, oxycodone hydrochloride, fentanyl citrate, and hydromorphone hydrochloride concentrations: 10, 10, 0.05, and 1 mg/mL, respectively).
Measurements:
In the compatibility tests, the opioid analgesics and target drugs were mixed in an equal volume ratio; the appearance, turbidity, and pH were evaluated immediately, one and four hours after mixing. Incompatibility was defined as change in appearance (turbidity increase ≥0.5 nephelometric turbidity units, Tyndall effect, visual judgment) and pH change ≥10%. Incompatible combinations were retested using dilutions of either opioid analgesics or the target drug.
Results:
Of the 255 combinations, 26 (10%) were defined as incompatible, including 12 morphine hydrochloride, 11 oxycodone, and 3 hydromorphone combinations involving 15 target drugs. Of the 28 retests conducted by diluting drugs in the combinations determined to be incompatible, the combinations of omeprazole (0.2 mg/mL) and lansoprazole (0.3 mg/mL) with morphine hydrochloride (1 mg/mL) remained incompatible.
Conclusions:
Utilization of these compatibility data for morphine hydrochloride, oxycodone, fentanyl, and hydromorphone in clinical practice should help guide safer drug administration and influence the selection of IV combinations in palliative care settings.
Key Message
Utilization of compatibility data for morphine, oxycodone, fentanyl, and hydromorphone in clinical practice should help guide safer drug administration and influence the selection of IV combinations in palliative care settings.
Introduction
Opioids such as morphine, oxycodone, fentanyl, and hydromorphone are used to treat moderate-to-severe pain, which affects 70%–80% patients with advanced cancer. 1 Furthermore, the prevalence of pain in patients with end-stage cardiovascular disease is reportedly 77%, with opioids being the treatment of choice for persistent pain. 2 For patients in palliative care who cannot take opioids orally or transdermally, intravenous administration is selected when subcutaneous administration is not possible because of peripheral edema, coagulation disorders, poor peripheral circulation, or a requirement for high volume or doses, or when rapid pain control is required. 1 Hospitalized patients are often prescribed various medications in addition to opioids for symptom relief and treatment of infections.3,4 Therefore, intravenous opioid injections may be combined with other drugs through the Y-site.
A clinical pharmacist has an important responsibility of providing information regarding incompatible drugs. Consequently, tools for preventing drug incompatibility, such as compatibility charts or the pH color code system, have been developed.5–8 However, in a questionnaire survey targeting Board Certified Pharmacists in Palliative Pharmacy certified by the Japanese Society for Pharmaceutical Palliative Care and Sciences (JPPS), 96% of respondents said that they received consultations for drug combinations administered through the Y-site that had not undergone compatibility testing, with 88% experiencing anxiety when answering these questions. 9 Notably, drug compatibility testing for opioid injections, which is necessary for clinical practice, is still lacking.
The limited drug compatibility data for opioid injections means that multiple separate venous access sites for the simultaneous administration of drugs with unknown compatibility may be required. However, establishing new venous access sites for geriatric patients and patients in palliative care may be difficult. Therefore, this study aimed to determine the physical compatibility of morphine, oxycodone, fentanyl, and hydromorphone with 64 intravenous drugs used in palliative care during simulated Y-site administration, using visual inspection, turbidity evaluation, and pH measurements. We conducted a questionnaire survey of 3640 pharmacists from the JPPS who were affiliated with a hospital or pharmacy to determine the target drugs. On the basis of the results, we selected the 64 target drugs. 10
Methods
Test materials
The opioid analgesics used in this study included morphine hydrochloride hydrate (morphine HCl) (Shionogi Pharma Co. Ltd., Osaka, Japan; Lots W5471, W5529, W5672, W5699, W5745, W5799, W5866, and W6051), oxycodone hydrochloride hydrate (oxycodone) (Daiichi Sankyo Co. Ltd., Tokyo, Japan; Lots SQA0015. SQA0018, SQA0025, SQA0026, SQA0027, SQA0029, SQA0033, and SQA0040), fentanyl citrate (fentanyl) (Terumo, Tokyo, Japan; Lots A0032, B0058, E2035, F2009, F2019, F2025, H1005, and H1006), and hydromorphone hydrochloride (hydromorphone) (Daiichi Sankyo Co. Ltd.; Lots UTA0021, UTA0022, UTA0029, UTA0039, and UTA0043). The 64 target drugs were selected among those typically administered at the Y-site for palliative care, including drugs requested by pharmacists affiliated with JPPS. 10 Concentrations of the drugs used in this study were prepared with reference to the upper limits of manufacturer recommendations or existing reports based on clinical concentrations.11,12 In principle, 0.9% sodium chloride (Otsuka Pharmaceutical Factory Inc., Tokushima, Japan; Lots 1A79P, 1J80P, 2E83P, 2E95P, 2H89P, 2K91P, 3B92P, 3H00P, and 4G79P) was used for dissolution or dilution. Water for injection (Otsuka Pharmaceutical Factory Inc.; Lot 11104C) was used for dilution as needed per instructions in the package insert. Ganciclovir and voriconazole were dissolved in 10 and 19 mL of water for injection, respectively, and diluted with 0.9% sodium chloride, while carperitide was prepared with water for injection only. Hydromorphone was diluted in 0.9% sodium chloride to prepare a 1 mg/mL solution. Fentanyl, morphine HCl, and oxycodone solutions were prepared at concentrations of 0.05, 10, and 10 mg/mL, respectively, without dilution.
The combinations for the compatibility tests were investigated prior to testing using the ASHP Injectable Drug Information 2023 Edition (ASHP database), a compatibility test database. 13 Combinations determined to be chemically incompatible or physically incompatible only by microscopic confirmation, which could not be performed in this study, were excluded.
Combinations judged to be physically incompatible were diluted with test materials and retested up to two times. The first retest was performed with the opioid concentration diluted to the lower limit of normal dosing concentrations and the concentration of the target drug unchanged. Thus, the concentrations of opioids diluted in 0.9% sodium chloride were as follows: hydromorphone (0.2 mg/mL), fentanyl (0.01 mg/mL), morphine HCl (1 mg/mL), and oxycodone (1 mg/mL).14–16 The second retest was conducted only if the drug combination of the first retest was judged as physically incompatible. In the second retest, the concentrations of opioids were the same as those used in the first retest, whereas the compatibility test concentration of target drugs was further diluted five times with 0.9% sodium chloride to the lower limit of the clinical concentration.
Test and control solutions
Test solutions comprised combinations of opioid analgesics and target drugs in a turbidity-measuring vial at an equal volume ratio (1:1) to a total volume of 12 mL. Control solutions prepared for all drugs were used as the reference for the evaluation of turbidity, visual appearance, and the Tyndall effect. Control solutions were diluted to the concentration of test solutions. Each control solution (12 mL) was prepared by mixing 6 mL of the test material and 6 mL of 0.9% sodium chloride in a vial for measuring turbidity. Similarly, pH control solutions were prepared with 0.9% sodium chloride in polypropylene containers to have the same concentrations after the test. Before being mixed as test or control solutions, each of the prepared test materials was passed through a 0.22-μm filter (Millex-GV PVDF filter unit, Merck Millipore Ltd., Cork, Ireland; Lots R0DB42488, R0SB84770, R1JB14225, and 0000221569). Human albumin was passed through a 0.44-μm filter (Millex-HV PVDF filter unit, Merck Millipore Ltd.; Lot R1SB00608).
Physical compatibility tests
Compatibility tests were conducted using three test solutions. The test duration was set to four hours, which is the maximum duration for the evaluation of physical compatibility alone as per stability and compatibility study guidelines. 17 Similar to the protocol for the existing Y-site compatibility test, the pH, turbidity, appearance, and Tyndall effect were evaluated immediately after mixing and at one and four hours after mixing. 18 The pH and turbidity were measured by inverting the test solutions 10 times immediately before measurement.
The pH was measured using a pH meter (LAQUA act D72, Horiba Ltd., Tokyo, Japan) and electrode (9618S-10D, Horiba Ltd., Tokyo, Japan), which was calibrated using pH 4, pH 7, and pH 9 standards before each experiment. Turbidity was measured using a turbidimeter (TurbiDirect TB300IR, Tintometer GmbH, Dortmund, Germany) according to the scattered-light measurement method; in addition, the change in the Tyndall effect was evaluated. Three consecutive turbidity measurements were conducted for each test solution during each period. Calibration was performed at four points using turbidity standards of <0.1, 20, 200, and 800 nephelometric turbidity units (NTU), according to the manufacturer’s recommendations. The measurable range was 0.01–1100 NTU. The Tyndall effect was observed in the dark using a red laser pointer (PR500-RC, Canon Marketing Japan Co. Ltd., Tokyo, Japan) (635 nm; maximum output, ≤1 mW). The laser was applied from the bottom of the turbidity-measuring vial, and visual confirmation of the laser was defined as the presence of the Tyndall effect (Fig. 1).
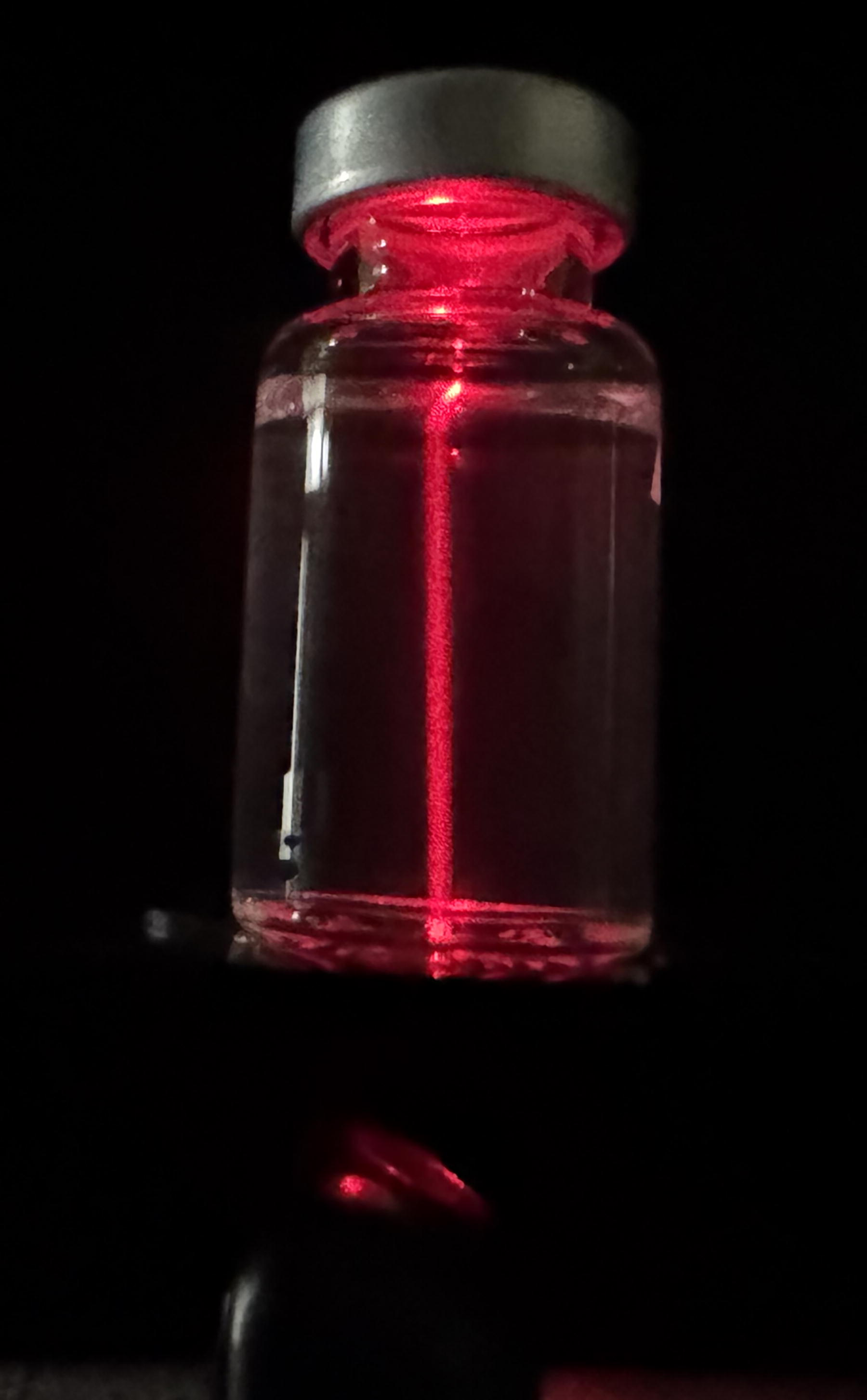
Verification of the Tyndall effect. The red laser pointer (635 nm; maximum output, ≤1 mW) is applied from the bottom of the vial that measures turbidity, and visual confirmation of the laser light is defined as the presence of the Tyndall effect. The figure shows the Tyndall effect using the vial with a standard turbidity value of 20 NTU (Standard T-Cal 20, Tintometer GmbH, Dortmund, Germany) as a mode. NTU, nephelometric turbidity unit.
Appearance was evaluated by visual inspection against both white and black backgrounds at a light intensity of 2000–3750 lx under a white LED light source (DS-LS24DSM-W, OHM Electric., Inc., Tokyo, Japan) (illumination; 3000 lx at 30 cm below the source) according to the 18th edition of the Japanese Pharmacopeia. 19 The specified illuminance was measured using a luminometer (LX-2500, Custom Co. Ltd., Tokyo, Japan).
Physical incompatibility was determined by visual, turbidity, and pH assessments. Physical incompatibilities associated with visual appearance and turbidity were defined as gross precipitation, cloudiness, change of the Tyndall effect, or a turbidity increase ≥0.5 NTU relative to the highest turbidity in control solutions.18,20,21 A pH indicative of physical incompatibility was defined as a change of ≥10% relative to the pH immediately after mixing.18,22,23
Results and Discussion
All control solutions for each opioid analgesic were colorless and clear, exhibiting a negative Tyndall effect. The turbidity and pH (mean value ± standard deviation) of control solutions were as follows: morphine HCl (5 mg/mL), 0.09 ± 0.02 NTU and pH 3.29 ± 0.01; oxycodone (5 mg/mL), 0.04 ± 0.04 NTU and pH 4.71 ± 0.01; hydromorphone (0.5 mg/mL), 0.04 ± 0.02 NTU and pH 4.16 ± 0.01; and fentanyl (0.025 mg/mL), 0.04 ± 0.03 NTU and pH 4.69 ± 0.01. Among these, morphine HCl, oxycodone, and hydromorphone underwent retesting; the turbidity and pH (mean value ± standard deviation) of control solutions at retest were as follows: morphine HCl (0.5 mg/mL), 0.05 ± 0.02 NTU and pH 4.26 ± 0.03; oxycodone (0.5 mg/mL), 0.04 ± 0.03 NTU and pH 4.85 ± 0.04; and hydromorphone (0.1 mg/mL), 0.08 ± 0.02 NTU and pH 4.48 ± 0.04. Among the 64 target drugs, the control solutions of six were positive for the Tyndall effect. The appearance and turbidity (mean ± standard deviation) of control solutions were as follows: human albumin (125 mg/mL), yellowish-brown, clear, and 8.21 ± 0.09 NTU; cefepime (20 mg/mL), light yellow, clear, and 0.13 ± 0.03 NTU; ciclosporin (0.25 mg/mL), colorless, clear, and 1.08 ± 0.07 NTU; micafungin sodium hydrate (0.75 mg/mL), colorless, clear, and 0.23 ± 0.05 NTU; tacrolimus (20 µg/mL), colorless, clear, and 0.29 ± 0.06 NTU; and teicoplanin (4 mg/mL), colorless, clear, and 0.34 ± 0.04 NTU.
According to the ASHP database, a combination of 10 mg/mL acetaminophen and 0.05 mg/mL fentanyl reportedly produces clear particles under a microscope, as per the United States Pharmacopeia 788, at four hours.13,24 Therefore, the combination of acetaminophen and fentanyl was excluded from this study. A total of 283 combination tests with the four types of opioid analgesics were conducted, including 28 retests (Table 1). Of the 255 combinations, 26 were defined as incompatible. The incompatibility results of each opioid were as follows: morphine HCl was incompatible with 12 drugs, oxycodone with 11 drugs, hydromorphone with 3 drugs, and fentanyl with no drugs (Table 2).
Drugs Tested for Physical Compatibility with Morphine, Oxycodone, Hydromorphone, or Fentanyl
GLYCEOL® (200 mL) contains 20 g of concentrated glycerin and 10 g of fructose. MAGNESOL® (20 mL) contains 2 g of magnesium sulfate hydrate and 2 g of glucose. MANNITOL-S (300 mL) contains 45 g of d-mannitol and 15 g of d-sorbitol.
Prepared in 0.9% sodium chloride injection.
Prepared in water for injection.
Dissolved in water for injection and then diluted with 0.9% sodium chloride.
Morphine HCl was diluted to 1 mg/mL in 0.9% sodium chloride injection.
Oxycodone was diluted to 1 mg/mL in 0.9% sodium chloride injection.
Hydromorphone was diluted to 0.2 mg/mL in 0.9% sodium chloride injection.
C, compatibility; Conc, concentration of the test drug; HCl, hydrochloride; I, incompatibility; Mfr, manufacturer of the test drug.
Description of Drug Incompatibility with Morphine, Oxycodone, or Hydromorphone
Control solution was prepared by mixing the target drug with 0.9% sodium chloride in a 1:1 ratio.
Prepared in 0.9% sodium chloride.
Dissolved in water for injection and then diluted with 0.9% sodium chloride.
NTU, nephelometric turbidity unit.
Lansoprazole, omeprazole, and potassium canrenoate were found to be incompatible with morphine HCl, oxycodone, and hydromorphone. The combination of potassium canrenoate and opioid analgesics resulted in immediate precipitation after mixing. In contrast, combinations of lansoprazole or omeprazole with opioid analgesics resulted in color changes or precipitation over time (Fig. 2). The combination of morphine HCl and lansoprazole or omeprazole was defined as incompatible immediately after mixing because of the occurrence of the Tyndall effect. The combination of oxycodone and lansoprazole appeared slightly cloudy immediately after mixing; however, this quickly resolved following the gently shaking of the test vial, with the solution becoming colorless and clear. Because these combinations were cloudy even for a short period of time, they were deemed incompatible.

Compatibility of drug combinations that showed color changes over time.
Ganciclovir, acyclovir, furosemide, aminophylline, and letemovir were considered incompatible with morphine HCl and oxycodone. Ampicillin/sulbactam, fosphenytoin, meropenem, and micafungin were considered incompatible with morphine HCl alone. Teicoplanin, methylprednisolone, and posaconazole were considered incompatible with oxycodone alone. All but six of these combinations were judged to be incompatible because of precipitation. The combination of morphine HCl with meropenem resulted in color changes over time (Fig. 2). The combination of morphine HCl and letermovir was defined as incompatible immediately after mixing because of the occurrence of the Tyndall effect. The combination of oxycodone and teicoplanin was judged to be incompatible immediately after mixing due to an increase in the turbidity by ≥0.5 NTU. The combination of morphine HCl and micafungin appeared cloudy white immediately after mixing; however, it quickly resolved, becoming colorless and clear. Because these combinations were cloudy for a short period of time, they were deemed incompatible. Furthermore, the combination of morphine and furosemide and the combination of oxycodone and posaconazole were considered incompatible immediately after mixing due to the occurrence of turbidity.
Twenty-six combinations that were defined as incompatible were retested using diluted opioids; among these combinations, “1 mg/mL omeprazole with 1 mg/mL morphine” and “1.5 mg/mL lansoprazole with 1 mg/mL morphine” were determined to be incompatible. These combinations were retested a second time (retest 2), in which omeprazole (0.2 mg/mL) and lansoprazole (0.3 mg/mL) were also diluted in addition to morphine HCl (1 mg/mL). Following the second retest, both combinations were determined to be incompatible.
The most important factor responsible for incompatibility is a change in the acid–base environment of the drug. Of the 15 drugs that were determined to be incompatible, the standard solutions of nine drugs had a pH value >8; these drugs were as follows: ganciclovir (pH 10.60), acyclovir (pH 10.41), lansoprazole (pH 10.31), omeprazole (pH 9.66), potassium canrenoate (pH 9.42), ampicillin/sulbactam (pH 9.24), furosemide (pH 9.17), aminophylline (pH 9.07), and fosphenytoin (pH 8.44). As opioids are acidic drugs (morphine, pH 3.29; oxycodone, pH 4.71; hydromorphone, pH 4.16), these incompatibilities may be attributed to pH shifts. The finding that basic drugs can be combined with diluted opioid analgesics (excluding the combination of morphine HCl with omeprazole or lansoprazole) provides useful information that can help avoid drug incompatibility.
In contrast, the acidic drugs posaconazole (pH 3.52) and micafungin (pH 5.51) were incompatible in the following combinations: “posaconazole and oxycodone” and “micafungin and morphine HCl.” In a previous study on the compatibility of posaconazole with other drugs, of 91 drugs examined, all drugs that precipitated immediately when mixed with 1.2 mg/mL posaconazole had a basic pH (≥9.0, except for cefepime). 25 Therefore, this was one of the few cases in which the compatibility of posaconazole and oxycodone was considered to be independent of pH. In a previous study on the compatibility of 1.5 mg/mL micafungin and 15 mg/mL morphine sulfate, a white precipitate was reported to be formed immediately after mixing. 26 In this study, morphine HCl was used, and incompatibility was also observed immediately after mixing. Additionally, this study revealed that the combination of 1 mg/mL morphine and 1.5 mg/mL micafungin was compatible, which is a novel finding.
The combination of 40 mg/mL meropenem (pH 7.72) and 10 mg/mL morphine HCl was determined incompatible at one hour after mixing because of a color change. However, in a previous study using morphine sulfate, the combination of 50 mg/mL morphine sulfate and 50 mg/mL meropenem in a 1:1 ratio showed no incompatibility up to four hours after mixing. 27 Possible reasons for these different results include the difference between morphine sulfate and sulfate or differences in the additives in each drug, although this study was unable to elucidate these differences.
Of the 255 combinations evaluated in this study, 48 (19%) were present in the ASHP database as follows: 20 fentanyl combinations, 28 hydromorphone combinations, and 0 morphine HCl or oxycodone combinations. 13 In this study, among the combinations considered compatible, those of hydromorphone with cefazolin, diazepam, phenobarbital sodium, and heparin showed different results, which indicated that they were compatible or incompatible depending on the dilution. 13 Cefazolin, diazepam, and phenobarbital sodium are reportedly compatible with hydromorphone when they are diluted, whereas heparin is reportedly compatible with hydromorphone at a concentration of <12.5 mg/mL.28–30 In combinations involving diazepam, the dilution warrants special attention. Reportedly, when diazepam was diluted with water for injection, 0.9% sodium chloride, 5% dextrose, or Ringer’s injection in a ratio of <1:20 (mixing 1 mL of 5 mg/mL diazepam with 20 mL of each diluent), immediately visible precipitates formed in all four solutions. 31 In the present study, the concentration of these target drugs was lower than the concentration determined to cause incompatibility; therefore, the drugs were considered compatible, and we believe that there is no difference from the data in the ASHP database.
This study has some limitations. Chemical compatibility tests, such as stability tests, were not performed. Moreover, only morphine HCl was used, and the diluents used for the test drugs were limited; consequently, the results may be different if morphine sulfate is used or the drugs are diluted with 5% dextrose. Additionally, even if commercial drugs contain the same active ingredients, additives may differ depending on the pharmaceutical company producing them.32,33 As this study was not able to examine drugs from all pharmaceutical companies, the compatibilities of drug combinations may differ from those reported in this study due to the effects of additives.33,34 In particular, sodium bisulfate, an additive that may cause instability, was included in six drugs tested in this study: adrenaline, dobutamine, dopamine, hydrocortisone sodium phosphate, levodopa, and noradrenaline. 32 The present study was conducted under controlled laboratory conditions that may not fully replicate the complexities and variations encountered in actual clinical settings. Therefore, considering the instability of these drugs, it is necessary to monitor the therapeutic effects of each of the four opioid analgesics determined to be compatible when combined with a drug used in this study.
Conclusions
Of the 255 drug combinations, 26 were defined as incompatible, including 12 morphine HCl combinations, 11 oxycodone combinations, and 3 hydromorphone combinations, involving 15 target drugs. The drugs that were determined to be incompatible with morphine HCl (10 mg/mL) were acyclovir, aminophylline, ampicillin/sulbactam, fosphenytoin, furosemide, ganciclovir, lansoprazole, letermovir, meropenem, micafungin, omeprazole, and potassium canrenoate. The drugs that were determined to be incompatible with oxycodone (10 mg/mL) were acyclovir, aminophylline, furosemide, ganciclovir, lansoprazole, letermovir, methylprednisolone, omeprazole posaconazole, potassium canrenoate, and teicoplanin. Furthermore, lansoprazole, omeprazole, and posaconazole potassium were incompatible with hydromorphone (1 mg/mL).
Of the 28 retests conducted by diluting the drugs in the combinations that were determined to be incompatible, the combinations of omeprazole (0.2 mg/mL) and lansoprazole (0.3 mg/mL) with morphine HCl (1 mg/mL) were confirmed to be incompatible. Utilization of these compatibility data of morphine, oxycodone, fentanyl, and hydromorphone in clinical practice should help guide safer drug administration and influence the selection of improved IV combinations in palliative care settings.
This study involved compatibility tests during simulated Y-site administration of drugs commonly used in palliative care. In the future, we plan to conduct long-term evaluations of stability by simulated mixing in a patient-controlled analgesia pump or syringe pump, given the lack of stability tests or physical compatibility tests for these devices.
Footnotes
Authors’ Contributions
M.K., M.G., K.W., M.Y., K.S., H.T., H.K., and D.H.: Conceptualization, methodology, and writing—review and editing. M.K., M.G., K.W., M.Y., and K.S.: Formal analysis, experiment, and investigation. M.K., H.T., H.K., and D.H.: Supervision. M.K.: Writing—original draft preparation and funding acquisition.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This work was supported by JSPS KAKENHI (grant number: 22K09104) awarded to Masayoshi Kondo. The funders had no role in the execution of this study or interpretation of the results.