
Abstract
Introduction:
Home hospice medication management ideally addresses symptoms, reduces unnecessary medication use, and optimizes quality of life. Grounding decisions in goals of care is critical. How to ascertain and align patients’, families’, and clinicians’ goals for medication management remains challenging.
Objectives:
To describe the iterative development and acceptability testing of a structured, interdisciplinary approach to goal concordant prescribing (GCP).
Methods/Approach:
We started with a previously developed deprescribing curriculum that followed a three-step process: review, align, and simplify. We utilized human-centered design and adult learning experts to translate the existing curriculum into tools and training that addressed gaps identified in an environmental scan (see Supplementary Data for a review of existing tools). Weekly multidisciplinary design team meetings revealed the need for tools to facilitate medication-focused and goal-oriented communication. The revised GCP program includes three clinician-facing tools: (1) GCP Person-Centered Medication Reconciliation worksheet, (2) Goal Assessment and Priorities (GAP) Tool, and (3) GCP Conversation Guide. Acceptability was tested with nursing and social work staff at a not-for-profit hospice who completed two 2-hour GCP training sessions. We used a content analytic approach to evaluate written and verbal feedback that was collected after each session.
Results:
Participants felt that framing deprescribing in positivist language that connected medication changes to goals was innovative and a useful conversation skill. Participants also felt that GCP training was acceptable, the GAP tool and skill practice were useful, the GCP Program added value to clinical practice, and medication review in relation to prioritized goals was innovative and useful without adding to clinician workload.
Conclusion:
GCP supports alignment of patient and family priorities with medication management. This nurse-delivered intervention involves the interdisciplinary team and employs novel tools. Pilot testing indicates GCP tool and training acceptability to facilitate medication management conversations.
Key Message
This article describes the iterative development of a clinician-facing toolkit for goal concordant prescribing (GCP) in hospice. Acceptability testing indicates that clinicians are positive about tools to facilitate goal assessment and prioritization around medications in hospice, as well as training to guide deprescribing within the framework of GCP.
Introduction
Ensuring that medication prescribing addresses symptom management, minimizes unnecessary medication use, and optimizes quality of life is a critical function of hospice care. “Deprescribing,” the practice of reducing unnecessary medication burden under clinical supervision, is described as “the systematic process of identifying and discontinuing drugs in instances in which existing or potential harms outweigh existing or potential benefits within the context of an individual patient’s care goals, current level of functioning, life expectancy, values, and preferences.” 1 How to optimize deprescribing based on patients’ values and preferences while accounting for prognosis is challenging. 2
We previously proposed that an important first step is to reframe deprescribing as “goal concordant prescribing (GCP).” 3 This opens the deprescribing aperture to better reflect the reality of clinician–patient–family caregiver (FCG) interactions, where each party brings their own understanding, goals, and priorities to the shared decision-making process. 4 Grounding prescribing decisions in goals of care, rather than in lists of appropriate drugs5,6 or high-risk drugs, 7 is important in hospice where successful outcomes often depend on patient/family preference.8,9
Clarity on how to operationalize GCP is lacking. 8 Further, it is challenging for clinicians to accurately ascertain prioritized patient goals, and existing deprescribing approaches tend to overlook the role of frontline nurses and other nonprescribers on the interdisciplinary team (IDT) in the process of medication-related decision-making. 10 To address these gaps, this article describes the iterative development, refinement, and acceptability testing of a clinician-facing toolkit for a GCP program that supports medication-focused, shared decision-making in hospice.
Methods
Building on an existing training program to create the goal concordant prescribing program
The GCP Program was developed from an existing deprescribing training called SIMPLIfy (Shared Medication PLanning In [SIMPLIfy] Home Hospice: An Educational Program to Enable Goal-Concordant Prescribing In Home Hospice). 3 The training consisted of a three-part, 1.5-hour total clinician-facing didactic sessions that included communication demonstration and role-plays. The goal was to teach hospice clinicians a standardized deprescribing approach that aligns medication prescribing with patients’ and caregivers’ goals. To help them retain and practice the communication skills presented in the curriculum, clinicians received a “cheat sheet” of useful phrases. They also received medication management notebooks that could be given to patients and FCGs that addressed management of common symptoms, medications in hospice, and deprescribing. The training was used in a cluster-randomized feasibility trial that included clinician feedback at the trial’s end (ClinicalTrials.gov NCT03972163).
While clinicians and patient-FCGs responded positively to user-testing in the feasibility trial at two hospice programs, 11 exit interviews from participating clinicians identified several challenges and opportunities for improvement. This feedback was used to develop the GCP Program.
Developing the GCP program
With the SIMPLIfy training 3 as a starting place, we developed GCP using a human-centered design process. This included a four-step design-thinking model: (1) Clarify, (2) Ideate, (3) Develop, and (4) Implement. 12 Human-centered design “is a problem-solving technique that puts real people at the center of the development process, enabling you to create products and services that resonate and are tailored to the audience’s needs. The goal is to keep users’ wants, pain points, and preferences front of mind during every phase of the process.” 13 It is an iterative, collaborative, and person-centered approach for designing products and systems to solve complex challenges. 14 Human-centered design approaches share several principles: end-user involvement, iterative design, and multidisciplinary teamwork.15–17
To execute this process, we convened a multidisciplinary team of experts in nursing practice and communication (S.D.M.; M.C.), serious illness communication and palliative medicine (E.F.), geriatric medicine and pharmacoepidemiology (J.T.), human-centered design (L.O.), and adult learning theory (J.R.).
Step 1. Clarify
The team reviewed the exit interview feedback from SIMPLIfy to distill the opportunities for improvement: (1) clinician users (hereafter “users”) wanted more specific guidance about how to have the conversation; (2) users wanted to be shown how the deprescribing process could be integrated into their workflow with very clear steps; (3) users suggested a medication recommendations worksheet to support longitudinal medication management; and (4) users requested an approach to deprescribing conversations that allowed the staff to demonstrate that they have the “best interests of the patient in mind,” including detailed and clear guidance on how to determine patients’ goals of care.
Step 2. Ideate
The purpose of this step is to overcome “cognitive fixedness - a mindset in which one consciously or unconsciously assumes there’s only one way to interpret or approach a situation.” 13 Our multidisciplinary team met weekly to brainstorm solutions; this comprised the first iteration of development after the SIMPLIfy trial. 11 Discussions revealed the need for three new tools to facilitate medication-focused, goal-oriented communication: (1) a medication list that integrated patient and FCG goals into longitudinal medication management; (2) a tool to ascertain patient and FCG goals specific to hospice medication management; and (3) a workflow-integrated conversation guide to focus medication-related decision-making. We conducted an environmental scan for existing tools and found none specific to these needs (Supplementary Table S1). Thus, our multidisciplinary term agreed by consensus to develop the tools.
Step 3. Develop
We developed three prototype tools as specified in Step 2-Ideate. We sought external review of these prototypes from five active hospice clinicians (including a nurse practitioner, two RNs, and two RN clinical educators). While feedback was positive, they highlighted the need for the clinical case to illustrate tool use; this resulted in the case described in Figure 1. This comprised the second “post-SIMPLIfy” iteration of development. Else, they felt the prototype GCP tools were “Comprehensive and concise—a user-friendly tool for both admission nurses and case managers.” They noted that the “Color coded sections [were] easy to navigate. Prioritizes patient’s goals of care.” They commented on the usefulness of having “A talking point specifically regarding potential medication side effects.” One reviewer noted that the tools positively augmented workflow: “Medication review and reconciliation are an essential part of every visit. The guide could enhance the conversation to ensure that focus remains on the patient’s goals of care.” Each tool is described below.
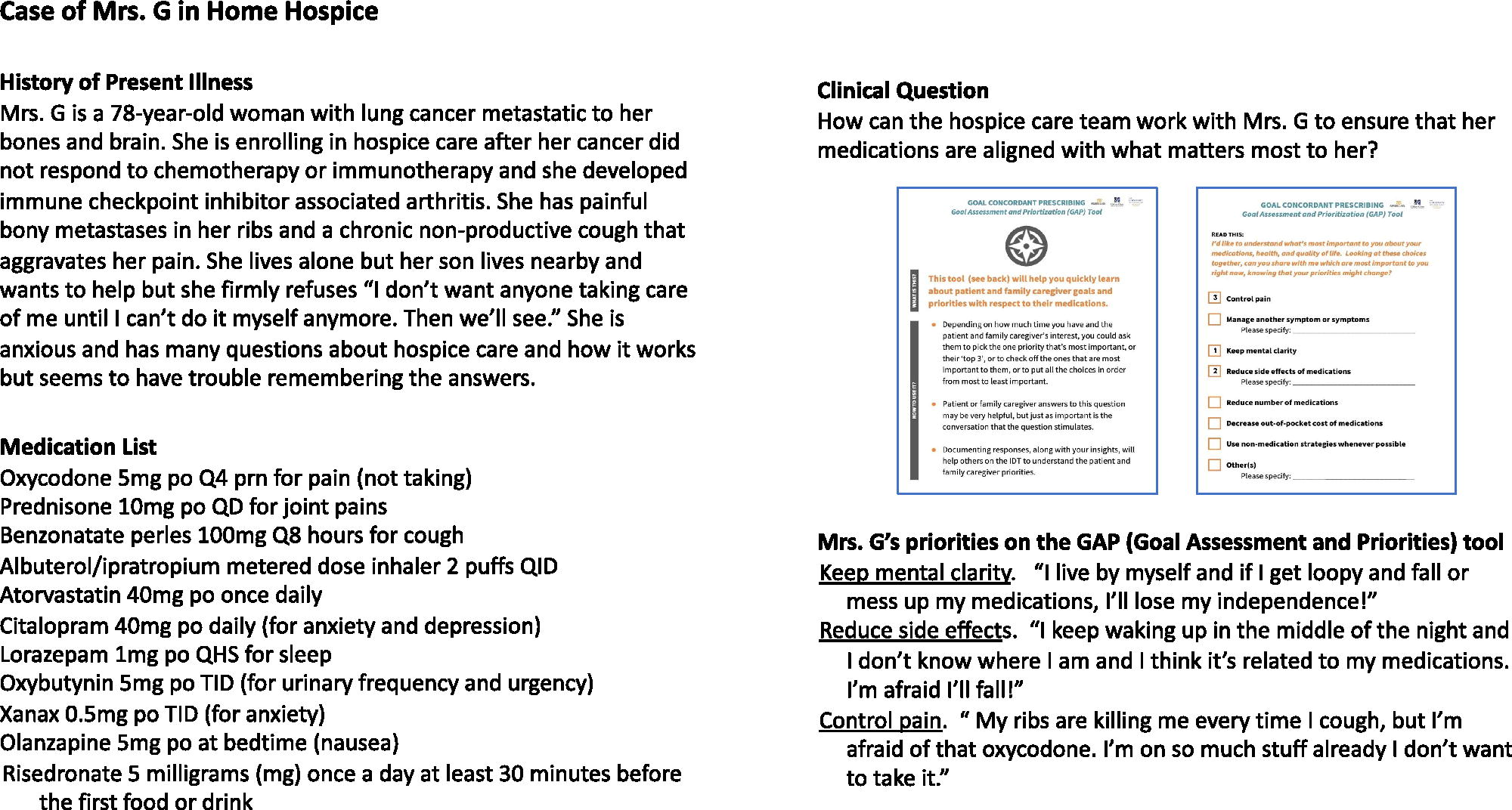
Clinical case to illustrate use of the GCP process. GCP, goal concordant prescribing.
Patient-Centered Medication Reconciliation tool
We felt that medication reconciliation could be expanded to elicit patients’ understanding of their medications, and that this can begin on hospice admission. To facilitate gathering this information during routine medication review, we augmented the medication list to solicit key aspects of medication use: Whether the medication is being taken, and if so, how? Whether the patient or FCG feels the medication is helping? How does the patient feels on the medicine (e.g., better or worse?)? Whether the patient and/or FCG is open to changing the medication? (Fig. 2). Ascertaining this information during the reconciliation process can improve efficiency in both short- and long-term medication management. For example, a GCP conversation for deprescribing would be approached very differently if a patient believed a medication was helpful and they were not open to changing it versus a medication that the patient is not taking because of adverse effects. The Patient-Centered Medication Reconciliation tool is designed to facilitate longitudinal involvement of multiple clinicians in the patient’s care and help the patient and FCG develop a shared understanding of the medications.
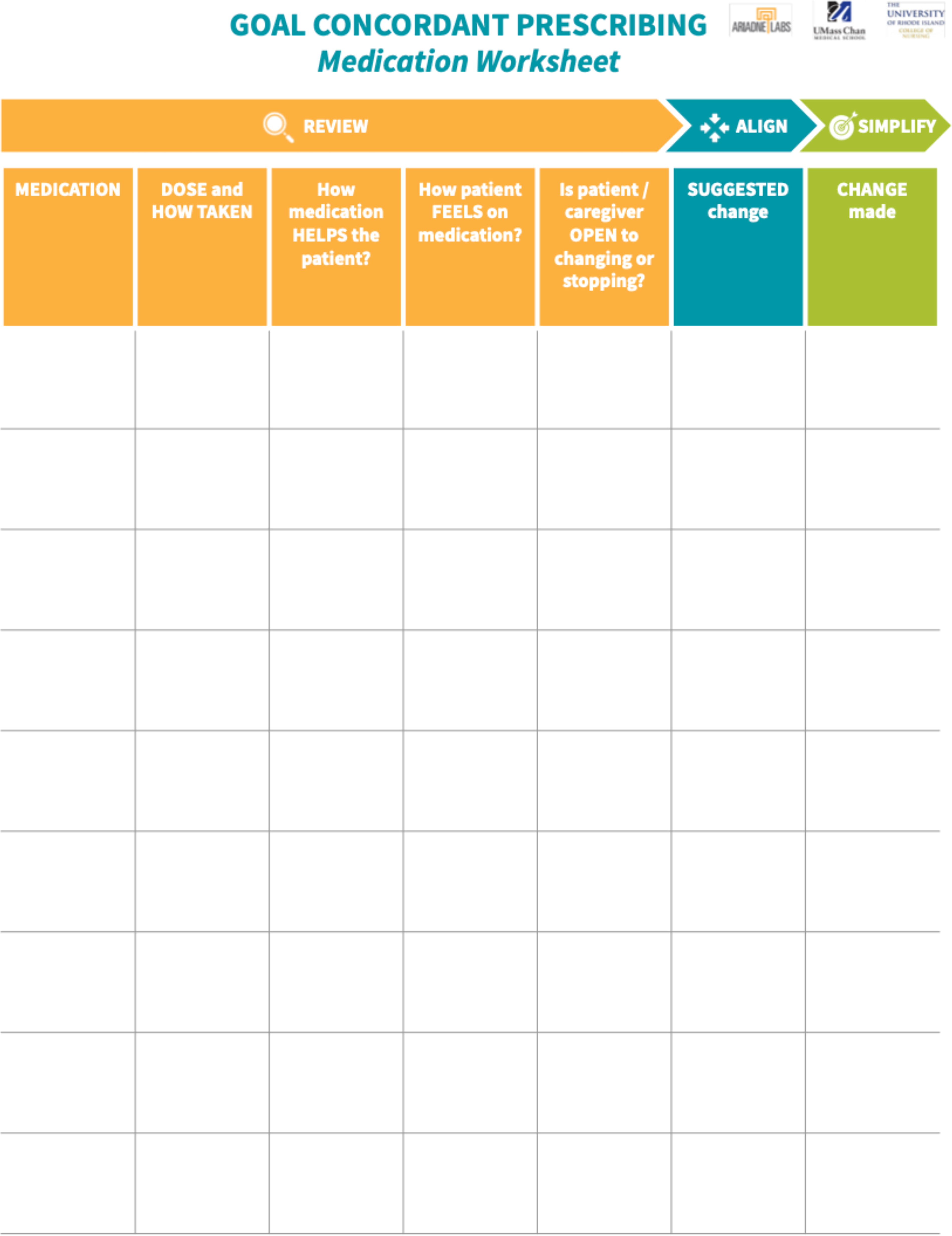
Patient-centered medication reconciliation tool.
Goal Ascertainment and Prioritization tool
GCP begins by talking about patient’s priorities in relation to medications. Rather than relying on a general exploration of goals and values, we developed the Goal Ascertainment and Prioritization (GAP) tool (Fig. 3). The tool presents options for the patient to compare, allowing them to identify options that are most important at that time, or to add options that are not included. The tool was designed to be printed so that the patient, FCG, and hospice clinician can look at it simultaneously and not need to hold all the options in their memory. The suggested goal options are drawn from palliative care and pharmacology literature but are not definitive; they may be modified to fit clinician practice, patient population, and cultural context.
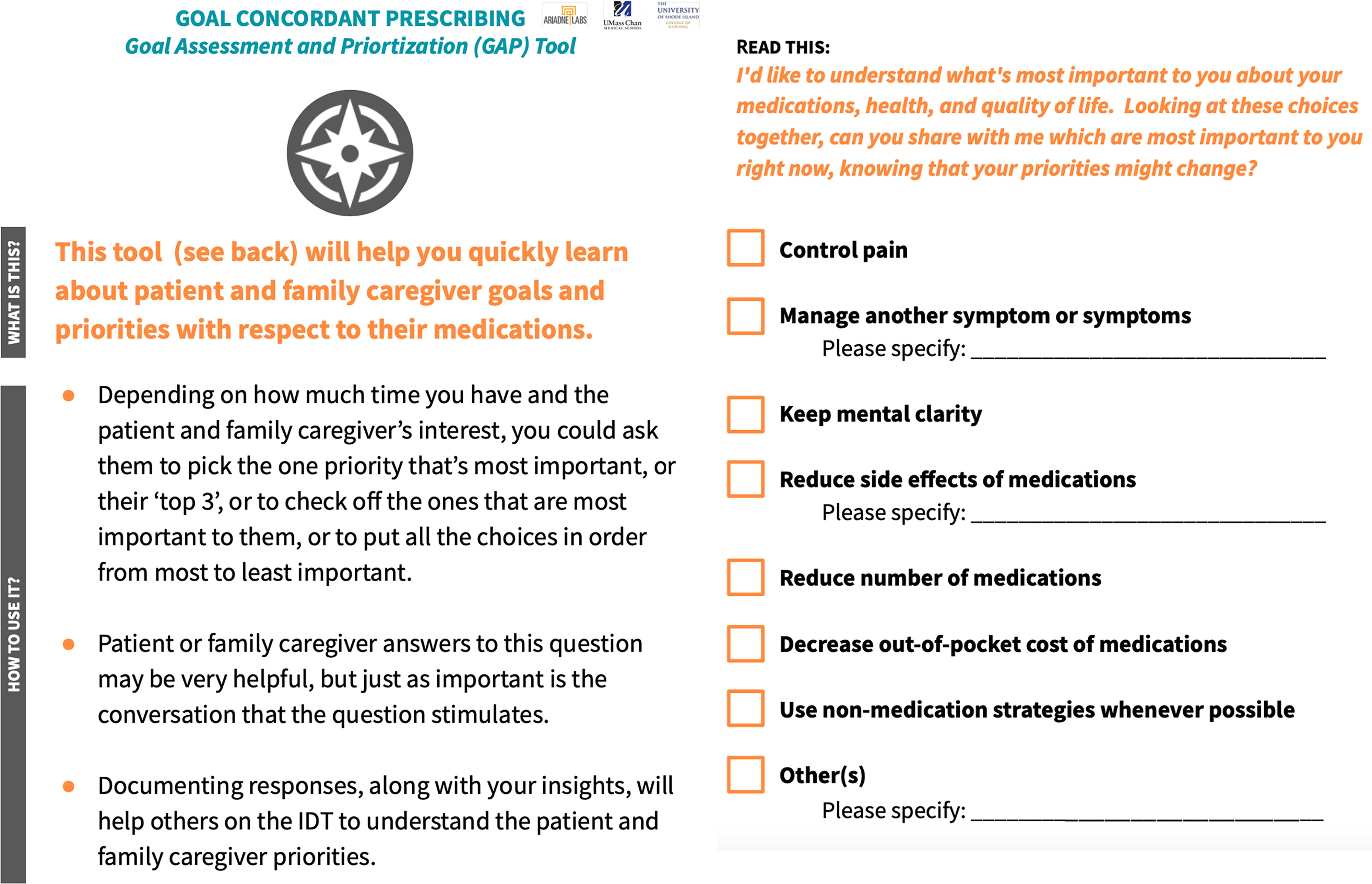
GAP tool. GAP, goal assessment and prioritization.
The reverse side of the GAP tool includes suggestions for use. Some patients may only be able to identify a few priorities or even only one that is most important, others may only be able to comment on how they feel about each option. Any response constitutes information that clinicians can use in better understanding patients’ priorities.
Once identified, as much as possible, the clinician and the IDT can use patients’ priorities to inform care and deprescribing decisions. Knowing patients’ and FCGs’ priorities, sharing them with the IDT, and using them to make and explain treatment decisions will support provision of the best care possible.
GCP conversation guide
This guide is intended to bring together the two proceeding tools into a suggested workflow for interdisciplinary GCP organized into three phases: review, align, and simplify (Fig. 4). Some or all these steps can be repeated as patients’ health status changes, necessitating a reassessment of priorities.
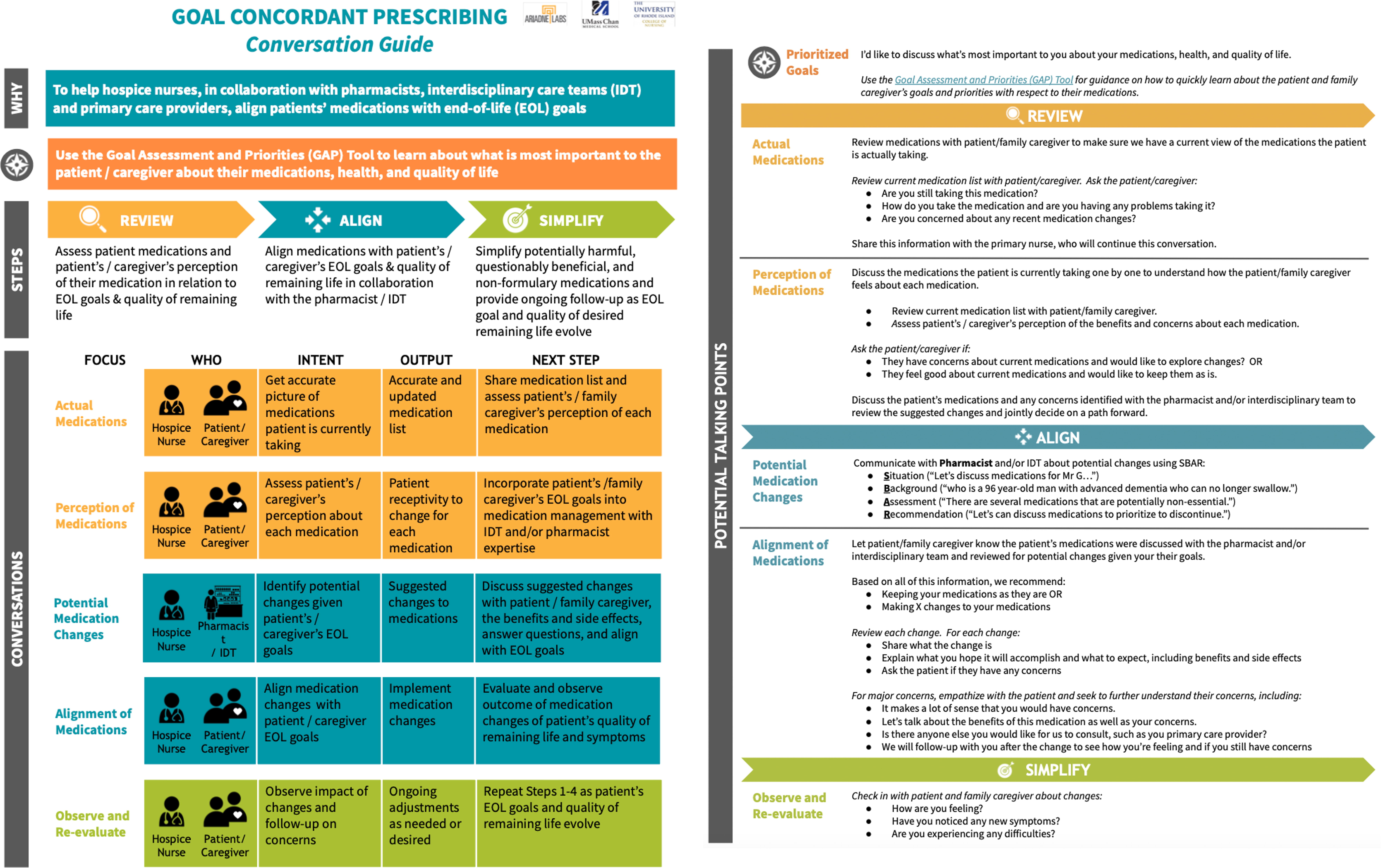
GCP conversation guide.
The “Review” phase ideally begins with the hospice Admitting Nurse using the Patient-Centered Medication Reconciliation List. The information gained may be particularly important for medications unrelated to the hospice admitting diagnosis and those that will not be covered by hospice. This information is intended to be passed to the Primary Nurse (i.e., nurse case manager), who can continue to explore patients’ medication-related perceptions. The Primary Nurse is best positioned to use the GAP tool to answer the key question: what is most important to the patient and FCG about their medications and quality of life.
In the “Align” phase, the Primary Nurse consults with the IDT and, if available, the pharmacist to identify potential changes based on the patient’s and FCG’s priorities. The Primary Nurse can then return to the patient and FCG with proposed changes and the rationale for each change. They show how recommended changes align with the patient’s and FCG’s priorities, or with the hospice team’s priorities. 4 This emphasizes why the changes are being made, not just the change itself. It may also reassure the patient to know that recommendations were formulated by a hospice team who were aware of their prioritized goals.
The “Simplify” phase occurs as medication changes are made, ideally in the direction of simplification although this may not always be the case. In this phase, it is critical to follow up to see whether changes are having the desired effect. If the changes are not working, it gives the hospice team the opportunity to revise the care plan and try again. If the patient and FCG see that the hospice team is committed to making sure the patient’s medications match their prioritized goals, not just saving money, future deprescribing efforts could be easier.
The front of the conversation guide emphasizes workflow, while the reverse side provides suggested phrases framed in positive language. We suggest language that frames medication changes in positive terms of “aligning the medications with the goals of care” instead of negating terms of “stopping,” “deprescribing,” or “taking away unnecessary medication,” so as not to perpetuate fears and negative perceptions of hospice.2,18
Step 4. Implement
At this stage, we assessed the acceptability of the tools with end users.
Setting and participants
Licensed hospice clinicians were recruited through a convenience sample at a single not-for-profit hospice in Massachusetts in late 2022. While the GCP program was always designed to train and include diverse interdisciplinary hospice providers (i.e., physicians, advance practice providers, social workers, chaplains and pharmacists) in the GCP process, 3 participant recruitment for this pilot test was tailored to accommodate the request of the hospice’s leadership to initially include nurse practitioners, all nursing staff, and executive staff (i.e., Executive Director, Director of Social Work, Clinical Director). Interestingly, positive response to Session 1 led the leadership to request the inclusion of all front-line social workers for Session 2.
Training overview
The program includes two, 2-hour sessions. Session 1 reviewed clinical risks of polypharmacy, standards for prescribing and deprescribing in hospice, and introduced the GCP tools. Session 2 detailed how to use the tools and used three role-plays to practice use of each component. The training sessions were held in an educational conference room with audiovisual support and space for interactive role play. We used powerpoints with embedded videos illustrating use of the tools with simulated patient, family member and interprofessional team members who illustrated use of the tool with the case summarized in Figure 1.
Data collection
We collected written and verbal reflections (unstructured open-ended questions) after each session about the overall training and tools, and evaluations of specific training components. In each session, we invited participants to verbally share what they wrote in their evaluations and to expand upon their thoughts and recommendations; this allowed the participants to generate an interactive discussion. Reflection questions included: What is new to you about this approach? What surprised you? What are you still curious about? What will you take forward? We kept field notes and a video recording from each training session. The team and research assistants reviewed the video recording of each session to verify field note content about spontaneous participant reactions.
Data analysis
Content analysis organized written and verbal feedback. All feedback was reviewed by three investigators (E.F.; J.T.; S.D.M.) and categorized into content areas of usefulness, acceptability, and perceived value by one investigator (S.D.M.).
Results: Testing GCP Training and Tool Acceptability
Training participants
The two-day, in-person, training had a total of 17 participants. Day one had 14 attendees (9 hospice nurses, 2 APRNs, and 3 Directors [executive, social work, and clinical]) who completed 8 reflections and 11 evaluations. Day two additionally included 3 social workers; these 17 participants provided 11 reflections and 13 evaluations. No pharmacists were included because this hospice did not employ one onsite.
Content analysis of evaluations and feedback
Usefulness of the GAP tool and training
Participants found the GCP toolkit and training useful. They reflected that discussing and prioritizing medications in relation to the patients’ and caregivers’ overall goals was new and differed from usual practice. One participant explained, “The setup of reviewing important aspects of their medications in relation to prioritizing [patients’] goals is a different way to approach these conversations.” Participants specifically appreciated the structured, team approach to the medication review, patients’ identification of the top priorities for their goals of care, and the alignment of medications with the patients’ values. All participants valued the “positive rather than negative” framing and language.
Acceptability
Participants noted that the structured and simplified approach of “review, align, simplify” would help facilitate and frame deprescribing conversations without adding to or changing their workflow. Acknowledging that medication management is “not just a once and done conversation”, many thought this would lead to a more focused and streamlined process. An unanticipated development was the request that social workers be trained since they could play a key role in difficult conversations.
Added value in practice
The GAP tool received the most enthusiastic reception. Participants agreed that the GAP tool would add value to their current practice. Participants thought that attending physicians might be more likely to approve medication change recommendations if framed in the context of patient’s priorities. They also appreciated the simplified and focused GCP conversation guide to frame medication management conversations.
Discussion
This article describes the iterative creation of a hospice clinician-facing toolkit and training that started with feedback from a clinical trial, then feedback about tool prototypes, and finally by feedback from an acceptability pilot test of the GCP training. Early testing of the approach to “review, align, and simplify” centered on patient goals, as well as response from representative hospice staff at each stage, was positive and suggests promise for improving care delivery.
The resulting program includes a standardized approach to GCP, supporting tools and a clinician training about how to operationalize GCP in home hospice. The toolkit was designed to give structure and support to clinicians, patients, and FCGs with specific grounding to facilitate interactions in home hospice. The Patient-Centered Medication Reconciliation Tool allows an initial assessment of readiness to change and a quick assessment of early medication discontinuation candidates. That is, if the initial review reveals medications that are NOT being taken or are causing undesirable side effects, initial deprescribing can focus on these drugs. This tool can also set up a roadmap for future deprescribing conversations as the patient’s clinical state evolves.
The GAP tool helps to simplify decision-making by providing a limited selection of patient goals that are mechanistically addressable with medication changes. This approach is analogous to the economic concept of presenting a “constrained choice,” which occurs when an individual must determine the optimal combination of options in the face of a constraint which limits the set of feasible combinations possible. 19
We were surprised by participants’ particular excitement about the GAP tool, because these hospice clinicians were very experienced at having goals of care and medication-related conversations with patients and FCGs. This enthusiastic response likely highlights the innovation of this tool to help frontline clinicians streamline their workflow and move toward goal concordance as highlighted in our qualitative results.
Our tools clarify and bolster the role of nonprescribing clinicians, including frontline nurses, in medication management by clearly delineating their importance in clarifying and communicating to the IDT the patient and FCG medication-related goals for care. For example, being able to clearly articulate goals such as “I want to be awake and alert during the day” can quickly get clinical stakeholders onto the same page, as well as help prioritize medication issues with the pharmacist.
As with all innovations, the GCP Program needs further testing to assess replicability of training acceptability as well as implementation feasibility in other hospice settings. We note that did not have full social work staff participation in the testing phase, which may have provided more information about their reaction to the entire training. We also acknowledge that use of the GAP tool may identify priorities that hospice may not be able to fully support or may identify potential conflicts between patient, FCG and hospice goals. Regardless, surfacing these issues is important and the GAP tool can also broaden the discussion to include other priorities where there may be common ground. Ultimately, we need to evaluate its impact on outcomes of importance to patients, families, and hospice organizations.
Our program is important because home hospice is one of the most challenging settings for prescribing. Changes in Medicare reimbursement have put pressure on hospice programs to control pharmacy costs.20–22 Hospice clinicians, especially nurses, are frequently in the position of explaining to patients and FCGs that some long-standing medications will not be covered by hospice. This conversation is even more difficult because it occurs early in the relationship when patients and FCGs have not had enough time to develop trust with hospice staff. 23 Recommendations to stop a long-term medication may be viewed with suspicion.24,25 The GCP toolkit is a promising way to streamline and structure such conversations. Early experience shows that frontline staff are receptive to such support.
Footnotes
Acknowledgments
The authors would like to acknowledge and express gratitude to the hospice program who participated in the evaluation of this program, as well as to Jennifer Rodine and Laura Onelio for their contributions to the development of the GCP tools.
Ethical Approval
Ethical approval for this study was obtained through the UMass Chan Medical School IRB (Project # H15417).
Funding Information
This work was supported by the National Institutes of Health [grant numbers R21 AG060017, K24AG068300]; and an Ariadne Labs Spark Grant.
Author Disclosure Statement
J.T. is a consultant to CVS Health and CVS Omnicare. The remaining authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.