
Abstract
Health care professionals can enhance conversations about serious illness and medical decision-making by adopting a transparent, standardized approach. This article critiques established communication strategies, which often emphasize patient values and goals without providing the necessary medical information to align these goals with a shared understanding of prognosis. We propose an alternate strategy that (1) provides detailed explanations of medical conditions at the beginning of the conversation, (2) includes support persons in discussions, (3) considers capacity, and (4) offers tailored advice by clinicians. The proposed framework aims to provide patients (or their delegates) with the information they need to integrate their values in pursuit of well-informed medical decisions. This strategy builds trust by providing honest information about medical conditions and their trajectories. It empowers decision makers to consider realistic outcomes, allowing them to accept or reject treatments in accordance with their preferences. This article presents a thorough step-by-step guide on how to conduct a serious illness conversation and facilitate medical decision-making, including a supplement that provides example phrases for use in clinical practice.
Introduction
Discussing serious illness and facilitating medical decision-making requires specific expertise. Central to this skill is a focus on communication that prioritizes the open and honest exchange of information contextualized to prognosis. This article advocates for a structured approach to clinician–patient discussions that first informs patients and then helps them make medical decisions that incorporate their values and goals.
Serious illness is a health condition that carries a high risk of mortality, negatively affects daily function, significantly impairs quality of life, or excessively strains caregivers. 1 Several guidelines offer valuable advice on how to discuss serious illness.2,3 Despite some differences, a prevailing theme is prioritizing individual goals and values throughout the discussion. The process typically unfolds sequentially: (1) initiate the conversation and prompt the patient to articulate their understanding of their medical conditions, (2) determine the preferred level of information the patient wants to receive, (3) gradually share the prognosis to match the patient’s readiness, (4) elicit goals and priorities, (5) explore fears, and (6) collaboratively develop treatment preferences based on stated values. In this way, conventional serious illness conversations aim to support patient goals by reinforcing the patient’s role as an expert in their own care.
Although broadly accepted, this process may cause patients to prematurely commit to values and goals without fully understanding their health history, prognosis, or treatment effectiveness—a relevant issue since well-informed patients often revise their decisions.4–7 In this context, guidelines that restrict the disclosure of prognostic information according to patient preference 3 can create a problematic knowledge gap and hinder the clinician’s ability to adequately inform, frame decisions, and provide the critical guidance traditionally expected from health care professionals.
The Palliative and Therapeutic Harmonization (PATH) model of care,5,6 developed by physicians at a Canadian center, represents a shift in the approach to serious illness conversations. The process is designed to ensure that patients (or their delegates) receive comprehensive details about their medical conditions, which in turn empowers them to apply their preferences. It prioritizes information sharing, decision-making with extensive clinician guidance, and incorporating frameworks8,9 that describe the complexities of frailty, dementia, and multimorbidity. The strategy also highlights the importance of considering the patient’s decision-making capacity and strongly advocates for including a support person during serious illness conversations. The process should be completed by an experienced health care professional with extensive knowledge of the patient’s medical history and treatment options, as well as the ability to prescribe medications, to ensure a holistic and comprehensive approach to care planning.
PATH communication is particularly beneficial for individuals with serious health conditions, especially when immediate or near-future medical decisions are necessary. To date, the communication strategy has been practiced in specialty clinics, 5 primary care, 10 acute care, 5 and long-term care. 7 In each of these settings, the approach significantly influences patient decisions. For example, in the original PATH cohort, 5 71 frail patients were scheduled to undergo 77 interventions such as surgery, nonoperative procedures, invasive tests, or hemodialysis. After completing the PATH process, patients (or their delegate) declined 75% of these procedures. A specialized care planning program, MED-LTC 7 used the same process to provide guidance to nursing home residents during the COVID-19 pandemic and significantly influenced decisions. Postconsultation, 83% of long-term care residents (or their delegate) de-escalated care plans. Of these, 62% decided against hospitalization compared with 7% preconsultation. Notably, these patients had previously undergone a conventional care–planning process, reinforcing the principle that sharing detailed information about an individual’s health status changes decisions.
In contrast to other models, the PATH methodology prompts clinicians to offer specific, well-supported recommendations when appropriate. It relies heavily on the application of evidence-informed decision-making and encourages clinicians to examine relevant literature to provide prognostic and treatment data contextualized to the individual. Although this guidance may at first appear paternalistic, the method is fundamentally patient-centered, using honest and open dialogue. These measures build trust and culminate in informed decisions that align with patient preferences.
Table 1 compares traditional guidance, exemplified by the Serious Illness Communication Guide, 2 and the PATH approach. 5
Contrasting the Serious Illness Conversation Guide with the Palliative and Therapeutic Harmonization Communication for Goals of Care Discussions
PATH, Palliative and Therapeutic Harmonization.
The steps and principles for PATH communication are outlined below.
Throughout the rest of this article, “patient” refers to the decision maker, whether it is the individual undergoing medical treatment or their delegate.
Steps and Associated Tasks
STEP 1: Get yourself ready: prioritize preparation
Task 1.1: Assemble the story
Before starting the conversation, clinicians need to be well-versed in essential information, such as knowing the patient’s complete medical history, understanding the prognosis of each medical condition, and being informed about the risks and benefits of potential treatments. The preparation demands not only an understanding of the primary issue, such as a cancer diagnosis, but also familiarity with other potentially life-limiting conditions, such as heart failure, dementia, or any diagnosis that might affect prognosis. To accomplish this, clinicians may need to consult specialists and/or the medical literature. By collecting this information and achieving this depth of knowledge, clinicians are well-equipped to provide clear and accurate information.
Task 1.2: Consider the patient’s decision-making capacity
Given the high prevalence of dementia and delirium among older adults, it is important to consider their ability to make medical decisions. A systematic review found that approximately 34% of patients in medical settings lacked the capacity to make informed treatment decisions, 11 usually due to dementia or delirium. The capacity to make medical decisions requires individuals to understand and appreciate their current state of health and available treatment options. Patients who are unable to make medical decisions will require a substitute decision maker, also known as a delegate. In these cases, it may be necessary to engage with the delegate independently, without the patient present.
Task 1.3: Involve family members or support persons
When discussing serious illness and medical decision-making, it is important for the patient to have a support person present during the conversation to promote understanding and provide emotional support during a difficult moment.
STEP 2: Start the conversation: state intentions
Task 2.1: Introduce yourself and your role
The initial exchange sets the tone for the entire discussion.
Task 2.2: Clearly state the purpose of the conversation
Initiate the conversation about serious illness with a straightforward explanation of its intent and objectives.
Task 2.3: Consider asking the patient to describe their health condition(s)
Guidelines often suggest beginning a serious illness conversation by asking the patient to describe their understanding of their medical conditions. While this approach may be reasonable in some cases, it can be challenging in others, such as when patients are expecting information about test results or are uninformed about their health status, which is often the case for frail individuals. 12
Based on the circumstance, the conversation can proceed in one of three ways: (1) ask the patient to describe their medical conditions and potential treatments, (2) have the clinician review information, or (3) let the patient choose between options 1 and 2.
STEP 3: Share information: build a common understanding
Task 3.1: Clarify the patient’s comfort level for receiving information
For patients to plan effectively, they need to be aware of illness severity and prognosis. Insufficient information leads to uninformed decisions,13,14 which can result in adverse outcomes and prolonged suffering.15–17 The current literature on serious illness conversation provides inadequate guidance on how to proceed when patients do not want full disclosure of their health status. In this situation, we recommend identifying a delegate—an individual selected by the patient who is willing to be informed and assist in decision-making.
Task 3.2: If appropriate, begin with a warning statement
A warning statement helps prepare the patient for the gravity of the discussion.
Task 3.3: Provide detailed information about medical condition(s)
PATH communication emphasizes the early dissemination of detailed information before discussing values and goals. By prioritizing this sequence, the clinician establishes a solid base from which patients can align their values with pragmatic treatment preferences.
Why is it important to prioritize early disclosure of clinical information? First, patients value accurate and realistic information about their health conditions, 18 a need often unmet by physicians.19,20 Next, clinical information changes decisions. Studies show that understanding the likelihood of surviving cardiopulmonary resuscitation (CPR) or learning about the prognosis of medical conditions reduces the preference for resuscitation and interventions.4–7 Finally, a comprehensive review of the patient’s medical conditions demonstrates the clinician’s grasp of the health narrative, which builds trust and fosters a shared understanding that empowers both parties.
Task 3.4: Give information in chunks and assess understanding
When giving information, break it into manageable chunks and regularly assess the patient’s understanding. Pause frequently to allow responses and inquire about comprehension. Identify any disparities between the information provided and the patient’s understanding. Avoid sympathy statements and instead acknowledge feelings to show empathy and support.
Task 3.5: Consider frailty
The prevalence of frailty increases with age, 21 affecting 15% of those aged 65 to 74 and at least half of those aged 85 or older. 22 Frailty can be understood by considering cognition, function, and mobility 23 and reflects a person’s state of health and vulnerability. It is typically associated with progressive decline. In addition, frail individuals commonly experience stepwise deterioration following an acute illness or intervention, after which there may be incomplete recovery and, thus, further frailty. 24 This pattern of decremental decline in health following an acute illness can be conceptualized as the frailty cycle (Fig. 1). 7
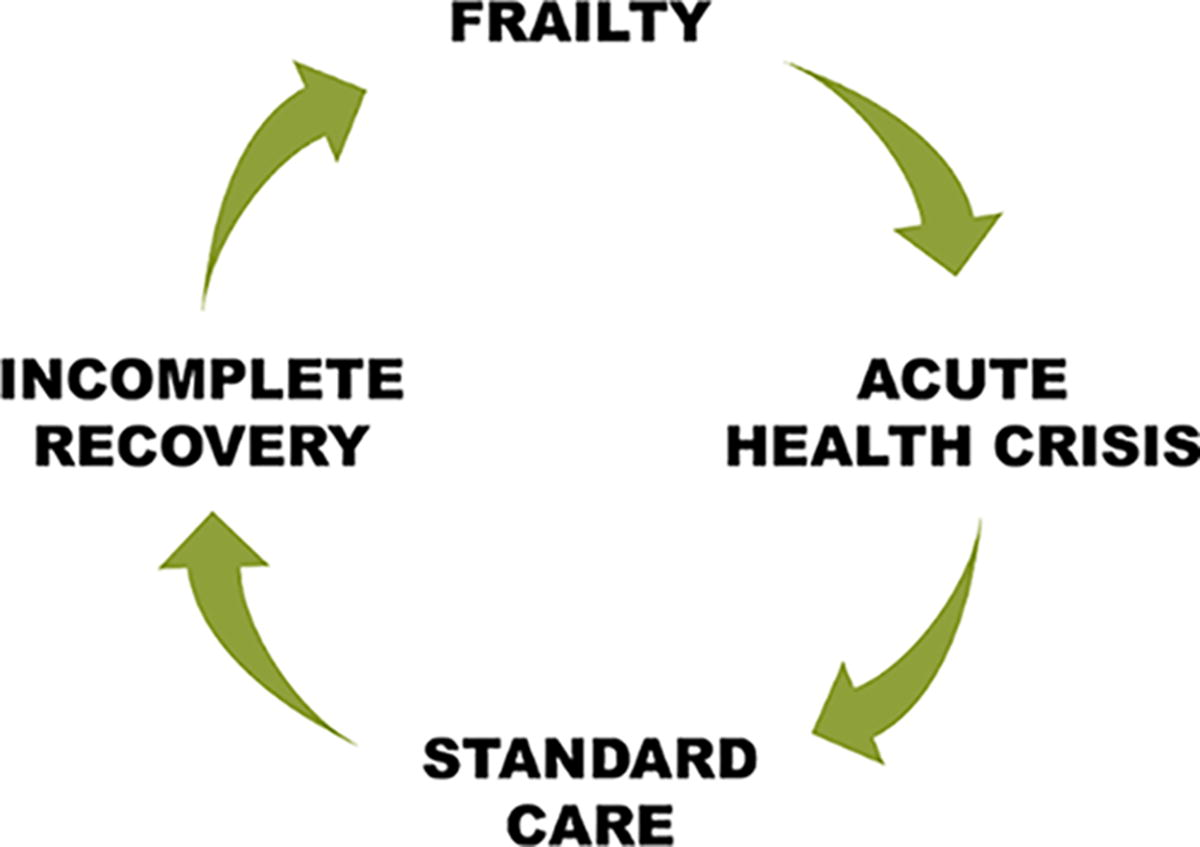
The frailty cycle.
When developing care plans, clinicians need to recognize frailty, honestly discuss its implications, 25 and explain the pattern of the frailty cycle. 7 Even so, frailty assessment should guide rather than dictate clinical decisions, tailoring discussions to individual health contexts and avoiding broad assumptions about quality of life based solely on functional status. While valuable for many older adults, frailty measures are not validated for those with lifelong disabilities 26 or reversible conditions like symptomatic osteoarthritis of the hip that can improve with surgery. As such, understanding frailty requires careful consideration of each patient’s present health and expected health trajectory.
STEP 4. Navigate decision-making: collaborate for informed decisions
Task 4.1: Guide decisions by considering realistic expectations and trade-offs
To emphasize realistic expectations, clearly communicate both potential benefits and risks of the proposed treatments, along with the expected progression of underlying conditions. This information helps patients and families understand likely outcomes and make informed decisions.
When relevant, patients can use predefined “PATH framing questions” during medical interactions. This inquiry helps patients clarify the full picture of their health and establish relevant goals. The questions include:
Which health conditions can be easily treated? Which cannot? How might frailty impact the risks associated with treatment? Will the proposed treatment improve or worsen function and memory? Will the proposed treatment require time in the hospital? If so, for how long? Will the treatment increase the number of good quality years, especially at home? What can be done to promote comfort and dignity in the time left? How will treatment impact living arrangements, supports required, and costs?
27
Task 4.2: When appropriate, make recommendations
Guidance about serious illness conversations and medical decision-making often suggests that physician recommendations should “flow only from patient goals.” 3 However, individuals facing serious illness highly value physician input.7,18,28 Accordingly, the PATH model advocates for clinicians to provide patients with evidence-informed recommendations, especially when a proposed treatment offers limited benefit. In this step, clinicians are urged to discourage treatments, even those considered standard of care, if they are likely to cause harm, such as performing CPR on individuals with advanced frailty. 25 Conversely, they should encourage treatments that are likely to be beneficial. This advice helps patients understand the risks and benefits of interventions and make decisions that align with achievable goals within the context of their health conditions.
STEP 5: Enable decisions: identify key choices
Task 5.1: Discuss treatment options and help the patient make decisions that align with their values and goals
After providing patients with a thorough understanding of their medical conditions, prognosis, potential treatment outcomes, and clinician perspective, it is now the right moment for them to make specific decisions. Equipped with knowledge and guidance, patients can approach their decision-making with clarity and confidence based on their preferences. This consensus building process might require a substantial amount of time, or in certain situations, occur over days.
The PATH decision-making form provides a structured outline that details possible treatments, ensuring all options are thoroughly discussed to guarantee comprehensive care planning (Supplementary Data S1).
Compared with the broader categories covered by the Physician Orders for Life-Sustaining Treatment (POLST), 29 the PATH form provides a more detailed framework for discussing specific care decisions, such as whether to pursue antibiotics, blood transfusions, and other common treatments. In addition, while the POLST is an official physician order form, the PATH form is included in the medical record as part of the consultation process and to document decisions. However, to make these decisions actionable, they must be transferred to an official order form.
STEP 6: Close the conversation: ensure understanding and documentation
Task 6.1: End the conversation with clarity and collaboration
At the end of the conversation, summarize key points, assess the patient’s understanding, and encourage final questions. If the patient lacks capacity to make medical decisions, ask the delegate what information should be disclosed to the patient.
Conclude with a clear action statement outlining next steps, document the care plan in the medical record, and provide the patient with a copy. Ready access to documented decisions is essential for guiding future clinical interactions, particularly during health emergencies.
The principles outlined in this article are presented, step-by-step, in the document titled “Strategic Communication to Empower Informed Decision-Making: The PATH Guide” (Supplementary Data S2).
Conclusion
Navigating the complexities of patient communication requires practical strategies and a commitment to transparent and honest dialogue. PATH communication introduces a new approach to serious illness conversations that focuses on thorough information sharing and personalized recommendations that consider overall health, frailty, and multimorbidity.
This article contends that exploring patient values early in the conversation is premature, as it is challenging to establish feasible goals when health issues are not fully understood. Instead, with the help of an experienced clinician, patients should apply their values and goals only after fully appreciating the significance of their medical conditions and expected outcomes. Far from being paternalistic, this strategy honors patient autonomy by providing a detailed understanding of health, thereby empowering patients to make decisions that align with personal preferences and realistic expectations.
By adhering to these principles and following the step-by-step guide (Supplementary Data S2), clinicians can master the nuances of communication, enhance their confidence, and transform a potentially daunting task into a compassionate and supportive exchange.
A follow-up article is planned to describe a specific conversation with a patient.
Author Disclosure Statement
L.M. and P.M. are the co-founders of the PATH program, which provides structured clinical models to care for the frail elderly. All other authors have no interests to disclose.
Laurie Mallery co-conceptualized and developed the communication framework, wrote the initial draft, and oversaw the revision process. She was part of a clinical team focused on improving communication strategies, which informed the manuscript.
Paige Moorhouse co-conceptualized and developed the communication framework, provided review and feedback, and was also part of a clinical team focused on improving communication strategies, which informed the manuscript.
Nabha Shetty helped with manuscript development and provided review and feedback. She is overseeing goals of care education and programming at Nova Scotia Health. She was also a member of a clinical team focused on communication strategies, which informed the manuscript.
Anne-Marie Krueger-Naug, Ashley Paige Miller, Maia von Maltzahn, and Amanda Tinning, provided review and feedback. They were members of a clinical team focused on communication strategies, which informed the manuscript.
All authors participated in the revision process, approved the final manuscript, and agree to be accountable for all aspects of the work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.