
Abstract
Background:
Constipation is an uncomfortable symptom experienced by many patients with advanced cancer, and it decreases the quality of life. Several studies have advised pharmacological therapies for constipation management, whereas others have promoted nonpharmacological approaches that promote changes in the patient’s lifestyle. However, constipation management by nurses has not yet been systematically reviewed in patients with cancer. Therefore, this study conducted a scoping review of nursing support focused on nonpharmacological therapies offered to relieve constipation in patients with cancer.
Methods:
The review was guided by Arksey and O’Malley’s five-stage scoping review framework. We searched the databases of PubMed, Cumulative Index to Nursing and Allied Health Literature, CENTRAL in the Cochrane Library, and Ichushi-Web of the Japan Medical Abstract Society from the databases’ inceptions to August 31, 2023, using various search terms such as “cancer,” “constipation,” and “nursing care.”
Results:
A total of 1501 articles that met the eligibility criteria were identified; of these, 5 articles were selected, and 1 additional article was found via handsearching. The final sample included six articles. We categorized the articles into three major nursing support types: acupressure, aroma massage to the abdomen, and self-management education. Five studies used a randomized controlled trial (RCT) design, including one with a randomized, waiting-list controlled trial, and one used a non-RCT design. All included studies showed the effectiveness of nonpharmacological interventions to improve constipation.
Conclusion:
This study also identified three types of nursing support for patients with cancer to relieve constipation. However, because of the small sample size, further evidence is required.
Key Message
Three major types of nonpharmacological nursing care for constipation were highlighted: acupressure, abdominal aroma massage, and self-management education. Such targeted nursing interventions have the potential to improve the quality of life of patients with cancer.
Introduction
Constipation refers to difficult bowel evacuation characterized by straining, lumpy or hard and dry stools, the sensation of incomplete evacuation, anorectal obstruction, or the use of manual maneuvers. 1 Constipation in patients with cancer can be caused by a variety of factors, including disease progression; medications such as opioid analgesics, antiemetics, iron, diuretics, and chemotherapeutic agents; metabolic problems such as dehydration, hypercalcemia, hypokalemia, diabetes mellitus, and hypothyroidism; poor food and fluid intakes; lack of privacy; inactivity; age; depression; and sedation.2,3 Constipation is an uncomfortable symptom experienced by approximately half of the patients with advanced cancer, and it decreases the quality of life.3–6
Several studies have highly recommended and guided pharmacological therapies for constipation management, whereas others have promoted nonpharmacological approaches that lead to changes in the patient’s lifestyle.3,7–9 The European Society for Medical Oncology (ESMO) Clinical Practice Guidelines identify pharmacological therapies for constipation in patients with cancer. It also suggests prevention and self-care strategies as nonpharmacological approaches. 3 As a complement to the ESMO results, the Multinational Association of Supportive Care in Cancer (MASCC) also recommends pharmacological therapy. Notably, nonpharmacological therapies with a higher level of evidence are not mentioned; although it recommends constipation management in patients with advanced cancer, regular assessment for constipation, individualized management, use of appropriate equipment, and adequate privacy, 7 the strength of the evidence for these recommendations is the lowest among the guidelines, as they are based on case reports and clinical examples.
Other recommendations support combinations of pharmacological and nonpharmacological treatments. The Oncology Nursing Society in the United States recommends lifestyle education and osmotic or stimulant laxatives for the treatment of opioid-induced constipation (OIC). 8 Its guidelines also suggest nonpharmacological approaches to manage constipation successfully. Nursing support often includes nonpharmacological therapies, and nurses play an essential role in managing and preventing constipation in patients with cancer.5,10 For example, nurses who support patients with cancer routinely assess constipation-related factors, monitor bowel movements, and educate patients on constipation management 5 and the need to promote changes in the patient’s lifestyle to reduce constipation. 3 Nursing support also includes monitoring symptoms, teaching, and treatments to prevent and decrease symptoms. 11 However, constipation management by nurses has not yet been systematically reviewed in patients with cancer, although there have been reviews in patients not diagnosed with cancer. 12 Nonpharmacological therapy to relieve constipation in patients not diagnosed with cancer indicated dietary modification, educational measures in lifestyle, and abdominal massage. For patients not taking opioid and not experiencing constipation, increasing fiber intake, fluids, and exercise may help prevent constipation; however, these measures may actually be harmful for those with advanced or progressive disease. 13 This study supplements previous guidelines and reviews by examining nonpharmacological therapies that nurses can provide to patients with cancer and will help indicate nursing support for relieving constipation in these patients in the future.
Study purpose
This study aimed to conduct a scoping review of nursing support provided for constipation relief in patients with cancer and to identify nonpharmacological therapies. In this study, nursing support for constipation is defined as any nonpharmacological treatment for constipation relief that a nurse can provide. The results can help clarify evidence-based nursing support for constipation in patients with cancer.
Methods
This study utilized the method developed by Arksey and O’Malley to conduct a scoping review of nursing support provided to alleviate constipation experienced by patients with cancer, 14 following the Preferred Reporting Items for Systematic Reviews and Meta-analysis Statement Extension for Scoping Reviews reporting guidelines and checklist. 15 Scoping reviews comprehensively map the extensive literature and understand the content of the research evidence; it is not necessary to assess the quality of the research.
This study was conducted up to the mapping of the scoping review and included reviews that assessed the effects of oncology nursing, defined as any type of intervention provided by nurses. Many nurse-led intervention studies often do not include details on the interventionists. 11 Therefore, if the care provider was not stated, the researchers, including oncology nurses, discussed whether nurses could provide the kind of care in their daily clinical practice. If the researchers agreed that nurses could provide this type of care, then it was identified as a nursing intervention. The complex interventions were also included if the nurse was mentioned as one of the care providers.
In addition, the protocol paper described five symptoms experienced by patients with cancer (pain, dyspnea, nausea and vomiting, constipation, and delirium) and caregiver burden, and this scoping review focused on constipation among these symptoms. 16 The scoping review applied a five-step process, as follows.
Identifying the research question
First, the scoping review identified the key research question: What types of nursing support are provided to resolve constipation experienced by patients with cancer?
Identifying relevant studies
Second, we searched PubMed, the Cumulative Index to Nursing and Allied Health Literature, the Cochrane Central Register of Controlled Trials in the Cochrane Library, and Ichushi-Web of the Japan Medical Abstract Society databases from the databases’ inceptions to August 31, 2023. Search formulas were first created in PubMed as an initial search. Subsequently, search formulas were created to match other databases Two authors (K.N. and Y.K.) completed this initial search in consultation with the librarian. The eligibility criteria were (1) patients with cancer over 18 years old; (2) intervention or observational studies that focused on relieving constipation; (3) nursing support (if the intervention provider was a nurse, the intervention was determined to be feasible by the nurse; if the intervention provider was not specified or the investigator, the study team discussed and decided whether the intervention could be routinely performed by the nurse); and (4) studies that quantitatively assessed constipation using a scale. The exclusion criteria were (1) at least 20% of patients in the sample did not have cancer, (2) secondary analyses, and (3) not written in Japanese or English. Acupuncture and electroacupuncture, which cannot be performed by Japanese nurses, were intentionally excluded.
Study selection process
Third, the web-based application Rayyan—a software for systematic reviews that facilitates initial screening through titles and abstracts—was used to analyze the identified articles. K.N. and Y.K. independently assessed the titles and abstracts of all studies, followed by full-text screening against the eligibility criteria. Any discrepancies in study selection were resolved by discussion. The study selection process is summarized in Figure 1.
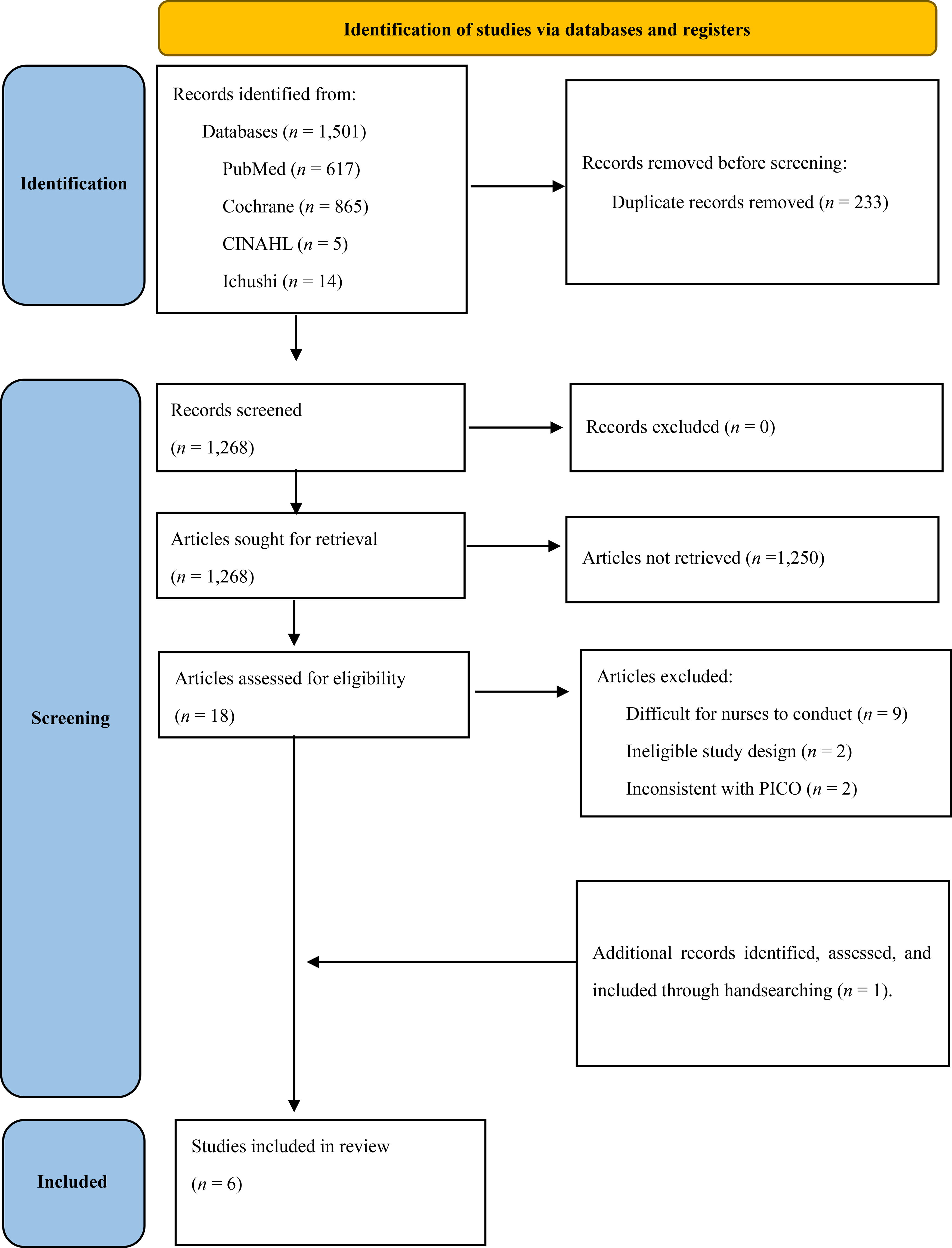
Flow diagram of the scoping review process.
Charting the data
Fourth, a Microsoft Excel spreadsheet was used to organize the data from the collected articles. Two authors (K.N. and Y.K.) independently entered data into the spreadsheet. A form was created to extract the study characteristics, including the first author’s name, publication year, country, title, study design, sample size, age, type of cancer, type of nursing support, outcome measurement tools, and results of the interventions for constipation. 16 Data were extracted independently by the same two authors. Studies were excluded at this phase if they did not meet the eligibility criteria.
Collating, summarizing, and reporting the results
Fifth, the nursing support provided in the studies extracted from the literature review was categorized by care components through qualitative thematic analysis. The nursing support data considered in the selected studies were extracted as raw data in Microsoft Excel; consequently, the nursing support elements were categorized. Initially, one author (K.N.) classified the data, which were validated by another author (Y.K.). Subsequently, the categorized data were further reviewed and validated by the study group, comprising the remaining coauthors. This multistep validation process ensured the accuracy and reliability of the data analysis.
Results
A total of 1501 articles that met the eligibility criteria were identified; 233 were excluded owing to duplication, and 1268 articles were selected. These were screened for title and abstract, with 1250 articles being excluded. The remaining 18 full-text articles were evaluated for eligibility, and 13 articles were excluded owing to tasks difficult for nurses to conduct (n = 9), ineligible study designs (n = 2), and inconsistency with the Population, Intervention, Comparison, and Outcome framework (n = 2). Finally, one additional paper was found via handsearching, for a final sample size of six articles (Fig. 1). We categorized care components into three major types of nursing support: acupressure (n = 4),17–20 abdominal aroma massage (n = 1), 21 and self-management education (n = 1). 22 Regarding the study design, five studies were randomized controlled trials (RCTs), including one randomized, wait-list controlled trial, and the other used a non-RCT design. All the extracted articles showed intervention effectiveness. Quantitative measures of constipation included the Constipation Assessment Scale (CAS) and the Bristol Stool Form Scale. Table 1 provides details on the included articles.
Summary of Elements of Included Articles
BSFS, Bristol Stool Form Scale; CAS, Constipation Assessment Scale.
Discussion
This study found that three types of nursing support were typically provided to patients with cancer to relieve constipation: acupressure, abdominal aromatherapy massage, and self-management education. Most studies included in this review were RCTs and demonstrated effective interventions. Some studies examined patients with breast cancer in the treatment phase, and acupressure on the abdomen was frequently used for participants in the end-of-life stages. However, there remains little nursing support available to relieve constipation in patients with cancer.
Acupressure
The number of studies examining acupressure has increased, and most reporting countries are in Asia. Reviews of acupressure have reported that acupressure relieves cancer-related nausea, vomiting, and fatigue23–25 and that auricular acupressure may be recommended in addition to standard treatment to prevent constipation in patients with leukemia. 26 Acupressure improves symptoms by stimulating specific acupuncture points on the body and improving the flow of qi in Traditional Chinese Medicine. Qi means the vital fluids and the energy that flow through our bodies. In contrast to acupuncture, acupressure is noninvasive, cost-effective, and easy to incorporate into clinical practice; therefore, it is increasingly being reported as a nonpharmacological intervention for constipation. 27 Studies of auricular acupressure in terminally ill patients with cancer published after September 2023 show short-run benefits, suggesting that auricular acupressure may be helpful in the terminal stages. 28 As acupressure is less invasive, we consider it useful as nursing support for alleviating constipation in patients with cancer. However, to conduct acupressure treatment, nurses must acquire acupressure knowledge and skills to identify effective acupressure points for constipation and apply appropriate pressure.
Abdominal massage
Both massage with essential oils and plain massage were found to improve constipation in patients with advanced cancer compared to the control group. The essential oil massage group had a higher CAS before the intervention than the plain massage group; however, by Day 5 post-intervention, both had decreased by a similar degree, and the symptoms of constipation had improved. 21 Aromatherapy has a relaxing effect, alleviating tension and anxiety. 29 However, in general, patients’ preferences for smells and ingredients and their perceptions tend to differ. When massaging the abdomen, both aromatic oil massage and plain massage options can be offered, depending on the patient’s preference. In the study, it was conducted by a nurse who is a certified aromatherapist; the other nurses have received training in massage techniques from a nurse who is a certified aromatherapist, whose assessment enabled them to provide care. Furthermore, abdominal massage stimulates the intestinal tract to induce and promote peristalsis and defecation. Reviews, including those on other diseases, suggest that abdominal massage can be effective in relieving constipation. 30 Abdominal massage improves constipation in OIC, and it is commonly implemented in nursing care. 31 Few studies on abdominal massage in patients with cancer have been reported, but the benefits of abdominal massage are promising.
Self-management education
Self-management education involves providing a self-management program to educate patients about abdominal massage, abdominal exercises, and information on proper defecation and position to alleviate antiemetic-induced constipation during chemotherapy. It should be noted that information on proper defecation and position is essential in this intervention. MASCC guidelines recommend providing adequate privacy and appropriate equipment, such as a commode and footstool, to promote defecation. 7 Educating patients about self-care to prevent constipation, including providing information on bowel positioning and tools for comfortable bowel movements, is likely to be beneficial regardless of the patient’s stage of disease.3,7
Limitations
This scoping review has some limitations. First, we excluded papers reported in languages other than English and Japanese because our research group lacked language proficiency beyond these two languages. Second, we did not evaluate the quality of the studies. Third, not all the nursing care interventions extracted in this study are routinely provided by nurses worldwide, as the scope of care provided by nurses varies from country to country. Fourth, the role of the oncology nurse is broadly defined, as there is no worldwide collective term for oncology nursing. 32 Therefore, the results of this study do not define the role of the oncology nurse.
Conclusions
This study identified three types of nursing support provided to patients with cancer to relieve constipation: acupressure, aromatherapy massage to the abdomen, and self-management education. Most of the studies considered were designed as RCTs, and the interventions were found to be effective. Future research should examine the feasibility of implementing these types of nursing support interventions to help treat and prevent constipation in patients with cancer.
Footnotes
Acknowledgments
The authors thank the National Center Consortium in Implementation Science for Health Equity (N-EQUITY) for their guidance and Editage (www.editage.jp) for English-language editing.
Authors’ Contributions
All the authors contributed to the preparation, drafting, and editing of this scoping review. K.N. and Y.K. conceived the idea for this research, followed by discussions with the other authors (K.K., M.K., M.M., Y.M., Y.S., T.S., and J.K.), contributing to the finalizing of the research idea. K.N. and Y.K. developed the data extraction tool and the systematic database search strategy in consultation with the specialist librarian at Yokohama National University. All the authors contributed to the preparation and editing of the article and read and approved the final version of this article.
Data Availability Statement
All relevant data have been included in this article.
Funding Information
This study was funded by the Japan Health Research Promotion Bureau (JH) Research Fund (2019-[1]−4) and JH Project fund (JHP2022-J-02). This work was supported by the Japan Society for the Promotion of Science KAKENHI (grant number 21H03236).
Author Disclosure Statement
The authors declare that they have no conflicts of interest.