
Abstract
Introduction:
Identifying the evolving needs of patients with advanced heart failure (AdHF) and triaging those at high risk of death can facilitate timely referrals to palliative care and advance patient-centered individualized care. There are limited models specific for patients with end-stage HF. We aim to identify risk factors associated with up to three-year all-cause mortality (ACM) and describe prognostic models developed or validated in AdHF populations.
Methods:
Frameworks proposed by Arksey, O’Malley, and Levac were adopted for this scoping review. We searched the Medline, EMBASE, PubMed, CINAHL, Cochrane library, Web of Science and gray literature databases for articles published between January 2010 and September 2020. Primary studies that included adults aged ≥ 18 years, diagnosed with AdHF defined as New York Heart Association class III/IV, American Heart Association/American College of Cardiology Stage D, end-stage HF, and assessed for risk factors associated with up to three-year ACM using multivariate analysis were included. Studies were appraised using the Quality of Prognostic Studies tool. Data were analyzed using a narrative synthesis approach.
Results:
We reviewed 167 risk factors that were associated with up to three-year ACM and prognostic models specific to AdHF patients across 65 articles with low-to-moderate bias. Studies were mostly based in Western and/or European cohorts (n = 60), in the acute care setting (n = 56), and derived from clinical trials (n = 40). Risk factors were grouped into six domains. Variables related to cardiovascular and overall health were frequently assessed. Ten prognostic models developed/validated on AdHF patients displayed acceptable model performance [area under the curve (AUC) range: 0.71–0.81]. Among the ten models, the model for end-stage-liver disease (MELD-XI) and acute decompensated HF with N-terminal pro b-type natriuretic peptide (ADHF/proBNP) model attained the highest discriminatory performance against short-term ACM (AUC: 0.81).
Conclusions:
To enable timely referrals to palliative care interventions, further research is required to develop or validate prognostic models that consider the evolving landscape of AdHF management.
Introduction
Heart failure (HF) is a progressive and incurable disease affecting more than 60 million individuals globally. 1 Despite the rapidly evolving advancements in medical therapy, HF remains characterized as a disease with high morbidity, economic burden, and all-cause mortality (ACM), with many patients progressing to advanced stages.1,2 In the United States, the prevalence of HF is projected to increase by 33%, from 9.7 million individuals in 2025 to 12.9 million individuals by 2060. 3
Patients with advanced HF (AdHF) experience severe and persistent symptoms resulting in functional constraints defined as New York Heart Association Class (NYHA) class III (i.e., marked limitation of physical activity) or class IV (i.e., have HF symptoms even at rest), severe cardiac dysfunction, unplanned hospitalizations from cardiac-related exacerbations, and severe impairment of exercise capacity despite optimal guideline-directed treatment.4,5 They suffer a multitude of physical and psychological symptoms. 6 Prior studies have highlighted that the end-of-life stage can begin three years before death and can vary by disease and individual.7,8 Early integration of palliative care has been recommended by the American Heart Association (AHA) 4 and the European Society of Cardiology 5 as it provides an opportunity to address the unmet needs of patients and their caregivers by providing timely and optimal symptom management, including exercise-based rehabilitation, and psychological and spiritual support. In optimizing scarce palliative care resources for those with the greatest palliative needs, some studies have focused solely on AdHF when deriving its referral criteria. 9
While there is consensus to integrate palliative care earlier, there is no systematic way to identify patients who are in the advanced stages of HF. 10 Despite experiencing symptoms comparable with patients with advanced cancer,11,12 patients with AdHF have suboptimal referral rates to palliative care, which occurs <2 weeks in the disease trajectory.13,14 In the United States, among 2,647 hospitalized patients with AdHF, only 6% were referred for palliative care services. 15 In Singapore, AdHF patients had the highest mean number of emergency department visits, inpatient hospitalizations, and substantial length of stay in the last one-year of life compared with patients with advanced cancer and other noncancer diagnoses. 16
Establishing the advanced stage for HF patients has been a challenging pursuit for clinicians and health care systems due to prognostic uncertainty. Complicating matters further are the patients’ poor understanding of their prognosis and the terminal nature of this disease. Varying attitudes and beliefs toward palliative care by health care providers eventually lead to low referral rates to palliative care.17,18 Consequently, the current management of HF patients has been biased toward life-prolonging therapies even at the end of life. Instead, the focus should be shifted toward improvement in quality of life through the reduction of cardinal symptoms such as dyspnea and fatigue, which can be managed with strategies, including palliative care and rehabilitation.16,19–21
International guidelines recommend assessing a patient’s risk of mortality to guide discussions on prognosis.4Accurately prognosticating AdHF patients can redirect health care resources to high-risk patients who may benefit from early palliative interventions. HF patients are at higher risk of death for multiple reasons beyond cardiac deaths alone. Predicting the risk of ACM captures the overall risk of death and provides a more holistic view of the patient’s prognosis. Prior systematic reviews have evaluated risk prediction models for HF patients of varying disease severity in ambulatory and out-of-hospital care settings.22–24 However, there is limited uptake of these models to augment clinical decision making and no one model can be endorsed. Several limitations have been highlighted that have hindered its adoption into clinical practice.22–25 These include the heterogeneity of the study population, inclusion of patients from clinical trials that lack representation of the wider population, methodological issues, and lack of data to assess for generalizability. Studies evaluating HF prognostic models, including the Seattle Heart Failure Model (SHFM) and Meta-Analysis of Global Group in Chronic Heart Failure (MAGGIC), found an underestimation of one-year mortality risks among ambulatory HF patients 26 and those with AdHF. 27
It is challenging for prognostic models to keep pace with the constantly evolving care management, device therapies, and pharmacological treatments for HF, and hence important to reassess the predictive utility of variables included in these models in contemporary cohorts of patients. It is unlikely that one model will be able to predict all types of HF and severity. Focusing on a narrower group of AdHF patients may yield models with better performance. While several models are available for HF, there are far fewer validated models specific to the AdHF population.
Given the importance of risk prediction in the AdHF population, we aim to perform a scoping review to identify risk factors associated with up to three-year ACM, and describe prognostic models developed or validated in AdHF populations. Insights from this review can provide a more nuanced understanding of risk factors and models to predict ACM in AdHF. Stratifying AdHF patients based on prognosis can facilitate referrals to appropriate care settings, closer monitoring of high-risk AdHF patients by specialist palliative care teams, meaningful conversations about serious illness, and patient-centered future care plans.
Methodology
We adopted the five-stage scoping review framework proposed by Arksey and O’Malley 28 and Levac et al. 29 The formulation of the research question was guided by the Population, Index prognostic factors, Comparator prognostic factors, Timing, and Setting framework. 30 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline was used to summarize the identification of studies.
Study eligibility
Primary studies published worldwide that included adults who were aged ≥18 years old, diagnosed with AdHF, assessed for risk factors that were associated with up to three-year ACM using multivariable analysis and written in English were considered for this review. AdHF was defined as HF patients with NYHA Class III or IV, or AHA/American College of Cardiology (ACC) Stage D, or patients identified to be in the advanced stages of the disease (Table 1).
Inclusion and Exclusion Criteria for Assessing Studies’ Eligibility
Bibliographic databases and search strategy
We searched in PubMed, OVID, Excerpta Medical database, Cumulative Index to Nursing and Allied Health Literature, Web of Science, and the Cochrane library databases for articles published between January 2010 and September 2020 to ensure that contemporaneous studies were included. We included gray literature and hand-searched articles (Supplementary Appendix S1). All searches were conducted with the assistance of a medical librarian, with input from clinicians.
The search strategy applied medical subject headings’ terms and keywords that were tailored to each database. To identify our study population, we included keywords such as “end-stage heart failure,” “advanced heart failure,” “New York Heart Association III and/or IV,” “American College of Cardiology Stage C and/or D”; keywords for study design included “randomized controlled trial,” “observational,” “longitudinal,” “cross-sectional,” “case-control,” “cohort”; keywords for type of analysis included “prognostic model,” “prognosis,” “multivariable model,” “multivariable analysis,” and keywords to identify our outcome included “all-cause mortality,” and “death rate.” Additional details are presented in Supplementary Appendix S1.
Appraisal of included studies
All included articles were appraised for risk of bias using the Quality of Prognostic Studies (QUIPS) tool where six domains were assessed—namely, study participant, study attrition, prognostic factor measurement, adjustment for other prognostic factors, and statistical analysis and reporting. 31
Screening and data extraction
Title and abstract screening, full-text screening, data extraction, and risk-of-bias assessment were performed using the COVIDENCE Systematic Review Software (Veritas Health Innovation, Melbourne, Australia). Title and abstract screening were performed by P.K., P.P.G., S.N.H.X., Y.W.F., E.C.S.S., R.Y.T., J.T., J.C., L.Z.H., L.T.H., V.H., T.C.K., A.C.H., T.W.S., and A.H., where each article was assessed by two reviewers. We tested the eligibility criteria to ensure interscreener agreement. Full text of articles that met the inclusion criteria were retrieved and screened to ensure relevance. Bibliographic information, study population, study design, statistical methods, risk factors examined, and mortality risk periods were extracted from each study. Full-text screening and data extraction were performed by P.K., P.P.G., S.H.N.X., R.T., and J.T. Disagreements were discussed and resolved through consensus within the team.
Analysis
We summarized key characteristics of the included studies and provided an overview of the risk factors investigated across the literature. These risk factors were described and categorized into broader domains, which may influence mortality. The emergent domains and subdomains were discussed with the research team before reaching consensus. For each risk factor, we counted the number of (1) unique articles it was assessed in, (2) models that reported the effect size of risk factors, (3) models that reported the risk factor to be significant, (4) models that found the risk factor to be associated with a reduced risk of up to three-year ACM, and (5) models that found the risk factor to be associated with an increased risk of up to three-year ACM.
Results
After removing duplicates and selecting the relevant articles that met our inclusion criteria, 65 articles were included in this scoping review, contributing to a total of 119 multivariable models (Fig. 1).
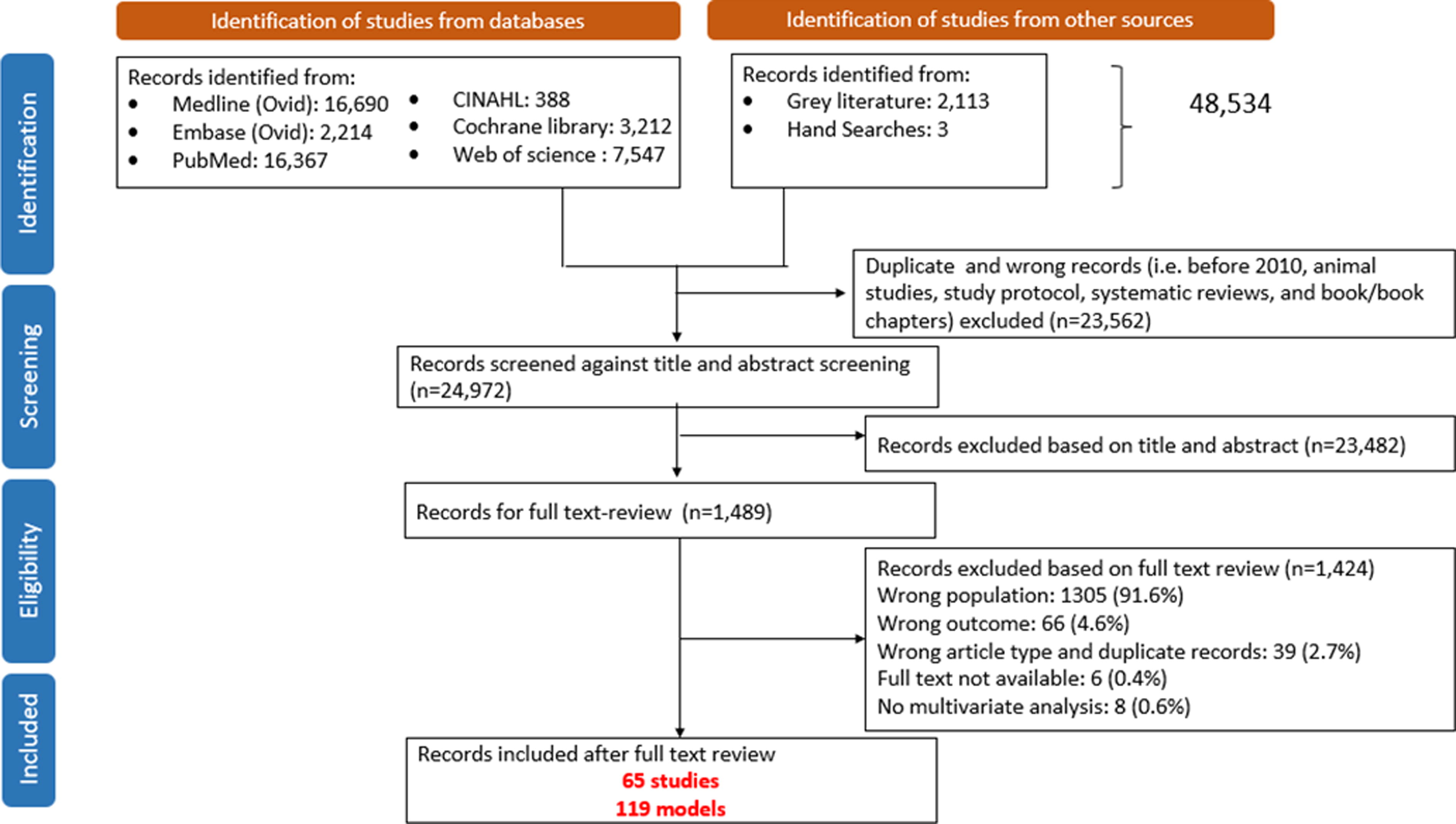
PRISMA flowchart of articles that were assessed.
Baseline characteristics of included studies
Most of the included studies were based in Western and/or European cohorts (n = 60 articles), in acute care settings (n = 56), with a median age of 65 years across study cohorts (Table 2).
Characteristics of the 65 Included Studies
Asia (China, India, Japan); Europe (Austria, Germany, Greece, Italy, Poland, Spain, Sweden); Middle East (Iran, Turkey); Multinational (multiple trial sites in North and South America and Europe); South America (Brazil).
Based on individual study’s inclusion criteria.
Median is derived from the study’s reported mean or median estimate.
IQR, interquartile range; LVEF, left ventricular ejection fraction; NYHA, New York Heart Association; AdHF, advanced heart failure.
Forty studies were secondary analyses derived from HF clinical trials, primarily from the Efficacy of Vasopressin Antagonism in Heart Failure Outcomes with Tolvaptan (EVEREST) (n = 19 articles, 43 models) and the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness (ESCAPE) (n = 14 studies, 22 models) trials. The Cox proportional hazard model was primarily used (n = 104 models), followed by logistic regression (n = 15 models).
Across the 119 models, 7 models (4 studies) assessed for in-hospital mortality (proportion died range: 4%−10.5%). A total of 81 models assessed for <1 year mortality (42 studies) (proportion died range: 3%−45%, median: 25%) and 31 models assessed for 1–3 years of mortality (31 studies) (proportion died range: 4%−72%, median: 31%).
Risk-of-bias assessment
Most articles were rated as having low-to-moderate bias based on QUIPS (Fig. 2). The domain “study attrition” was not appropriate for 12 articles as they were retrospective database studies and therefore assessed as ineligible. The domain “statistical methods and reporting” addresses appropriateness of the study’s statistical methods and completeness of reporting. Four studies were assessed as high bias as approximately 50% of the patients were excluded due to missing data.
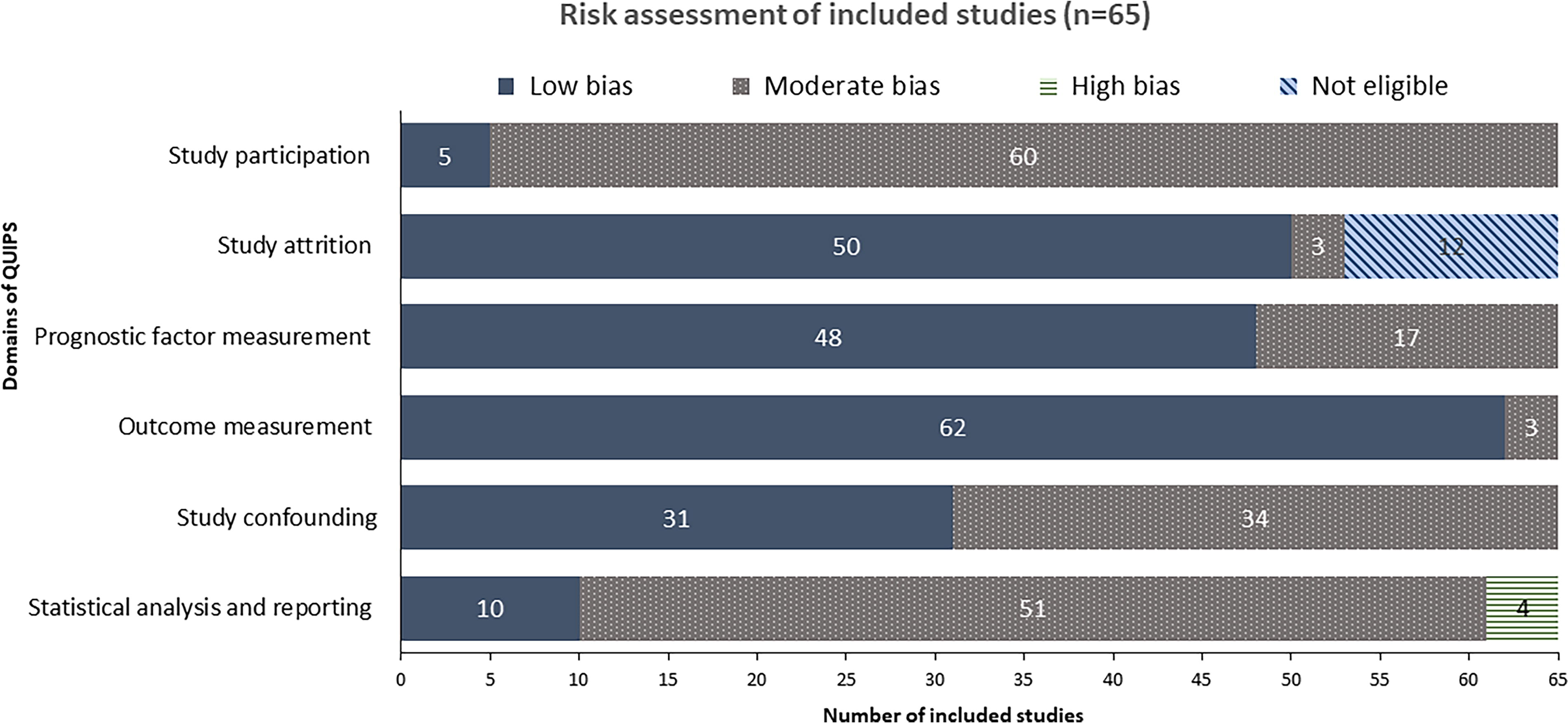
Risk of bias using the Quality of Prognostic Studies tool.
Domains and subdomains identified
We identified 167 risk factors that were identified and categorized into the following six domains, that is, individual factors, acute conditions, cardiovascular status, overall health status, interventions, and external factors (Table 3). Due to the heterogeneity of risk factors within each domain, we further categorized these variables into 29 subdomains (Table 3). A detailed list of all 167 variables can be found in Supplementary Appendix S2.
Overview of Risk Factors Associated with Mortality Among Advanced Heart Failure Patients
For most of the articles included, the tendency was to focus and report the effects of one or two key risk factors of interest while adjusting for other variables. We have reported variables that were commonly studied across the articles (Table 4). Overall, variables related to the domains of cardiovascular health and overall health status were frequently included in the models.
Subset of Risk Factors Commonly Assessed
ACEI: Angiotensin-Converting Enzyme Inhibitors (ACEI); ARB: Angiotensin II Receptor Blockers; BUN: Blood urea nitrogen; RF: Risk Factor.
Individual factors
Individual factors, such as demographics and advanced directives, were included in models across 48 articles (Table 4).32–78 Older age (6 models) and male gender (4 models) were significantly associated with high risk of ACM. Different ethnic groups, specifically AdHF patients of Caucasian, African American, and Hispanic ethnicity, had a differential risk for ACM. Only one article assessed the impact of advance directives. Patients with advance directives were noted to confound the risk of ACM.
Acute conditions
Short-term exacerbations were included across three studies45,48,60 (3 models) (Table 4). The presence of pneumonia (1 model) and having a late onset of acute kidney injury (1 model) were significantly associated with increased risk of ACM.
Cardiovascular status
A total of 57 articles32–49,51–86,89,91,92 included cardiovascular-related variables in the models (Table 4). Risk factors from cardiac-related medical parameters (36 articles), cardiac biomarkers (32 articles), cardiac imaging (31 articles), AdHF etiology (25 articles), and electrocardiograms (21 articles) were commonly assessed as prognostic factors.
Among the cardiac-related medical parameters, a lower systolic blood pressure (9 models) and more rapid heart rates (3 models) were associated with increased risk of death.
Of 10 models that reported the effect sizes of the cardiac biomarker, brain natriuretic peptide (BNP)/N-terminal pro b-type natriuretic peptide (NT-proBNP), six models found an association between increasing values of BNP/NT-proBNP levels with ACM risk.
Within the cardiac imaging subdomain, higher levels of ejection fraction were negatively associated with risk of ACM (5 models).
Ischemic and nonischemic AdHF etiology was observed to be commonly included (25 articles, 70 models). Although effect sizes were not reported in most of these models, ischemic AdHF etiology overall presented a higher risk of ACM (2 models).
In the electrocardiogram subdomain, the presence of atrial fibrillation or flutter conferred an increased risk of ACM (4 models).
Overall health status
A total of 57 articles33–37,39–45,47–81,83–92 included variables related to overall health status in the multivariable analysis. The most common subdomains studied were renal function (48 articles), full blood count (19 articles), comorbidity (30 articles), functional status (22 articles), and lifestyle risk factors (10 articles) (Table 4).
Renal function reflected by low estimated glomerular filtration rate (eGFR), low levels of serum sodium, and high levels of serum blood urea nitrogen was associated with increased risk of ACM. Five out of six models reported lower risk of death among those with higher hemoglobin levels. In contrast, one of the six models reported higher hemoglobin levels at admission being associated with higher risk of death.
While comorbidity burden was frequently included in the models, only 19 models reported effect sizes, of which comorbidity burden was not found to have a significant impact on mortality in 15 models.
With regard to function using the NYHA status, a higher NYHA status (IV vs. III) was associated with higher risk of death (18 articles; 3 models).
Interventions
A total of 37 studies32,33,35,39–42,44,45,47,51–55,57,58,61–65,69,73–78,81,82,85,86,88,93,94 assessed interventions such as medications, hemodynamic support, and cardiac-related interventions (Table 4). The use of angiotensin-converting enzyme inhibitors and/or angiotensin receptor blockers, and beta-blockers conferred a lower risk of ACM. Hemodynamic support and history of cardiac interventions such as coronary artery bypass grafts and implantable cardioverter defibrillators had no statistically significant influence on ACM (Supplementary Appendix S2).
External factors
A total of 17 studies accounted for nonpatient factors such as geographical region and health care payment sources (Table 4).32,34,35,39–42,47,50–54,57,63–65 Only one study found a differential effect of different payment sources (i.e., Medicare vs. Medicaid) on mortality.
Prognostic models developed or were validated in the AdHF population
One model predicted 6-month ACM based on the ESCAPE population, which had reasonable model performance (area under the curve; AUC: 0.78). 83 There were no data on external validation.
Szczurek et al. (2018) validated three models among the AdHF population in 2018. 95 The discriminatory performance of the model for end-stage liver disease (MELD-XI) was the highest (AUC: 0.812; 95% confidence interval [CI]: 0.769–0.856), followed by the HF survival score (AUC: 0.781; 95% CI: 0.732–0.829) and MAGGIC (AUC: 0.771; 95% CI: 0.720–0.823).
Scrutinio et al. (2015) validated six models among advanced acute decompensated HF patients for 90-day mortality (AUC range: 0.714–0.810) and in-hospital mortality (AUC range: 0.749–0.915). 96 The acute decompensated HF updated with the NT-proBNP (ADHF-NT-proBNP) model had the highest discriminatory performance in 90-day mortality (AUC: 0.810; 95% CI: 0.769–0.852) and in-hospital mortality (AUC: 0.815; 95% CI: 0.761–0.868). Prognostic models developed or validated on the AdHF population are summarized in Supplementary Appendix S3.
Discussion
Key findings of this scoping review
We reviewed 167 risk factors that were associated with up to three-year ACM and prognostic models specific to AdHF patients, across 65 articles that were rated with low-to-moderate bias. Risk factors were categorized into 6 domains and 29 subdomains, mostly reflecting cardiovascular health and overall health status. Several risk factors have emerged consistently across the articles. Lower levels of systolic blood pressure, ejection fraction, serum sodium, eGFR, hemoglobin levels, and higher levels of BNP/NT-proBNP and serum blood urea nitrogen were associated with increased risks of death. Generally, prognostic models identified in this review exhibited moderate model performance in the AdHF population, except for the MELD-XI and ADHF-NT-proBNP models that had the highest discriminatory performance against short-term ACM.
Variables identified in this review echo findings from previous systematic reviews,22–25 which included HF patients in either inpatient or outpatient settings. However, most of these HF prognostic models that utilized these variables, including those reviewed for AdHF in this study, have demonstrated poor-to-moderate discrimination (AUC range: 0.66–0.81). This average model performance can be attributed to population, variables, and methodological issues in model development.
Prognostic models for patients diagnosed with HF
Prognostic models for chronic HF such as SHFM (1992–1994), 97 HFSS (1986–1991), 98 and MAGGIC (1995–2008), 99 as well as for acute decompensated HF such as the ADHF-NT-ProBNP (2005–2011), 100 were developed on cohorts from past decades. As medical therapy and care management have evolved, the significance of predictors in these models may evolve over time. These risk models were developed before the introduction of angiotensin receptor/neprilysin inhibitor and sodium/glucose cotransporter 2 inhibitors to the AHA guidelines, which significantly reduces mortality risks among HF patients. 4 Prognostic models should be reassessed as new therapies are introduced to this population.
Current models may have included diverse HF populations, which lack variables to accurately discriminate survival probabilities or were derived from clinical trials that included less complex HF patients, limiting the generalizability to AdHF patients. It is unlikely that one prognostic model will be suited for all HF patients as underlying disease mechanisms and potential predictive variables differ by ejection fraction, etiology, or severity of HF. Risk stratification based on these factors may improve model accuracy.101,102
The ESCAPE and HFSS model were developed in AdHF populations. For the ESCAPE model, having had cardiopulmonary resuscitation/mechanical ventilation and BNP > 1300 pg/mmol had the greatest influence on risk of ACM. The presence of interventricular conduction defect and presence of ischemic cardiomyopathy had the highest weights in the HFSS model. Creatinine, sodium, hemoglobin, systolic blood pressure, left ventricular ejection fraction, and blood urea nitrogen had the highest weights across these models, indicating greater influence on short-term ACM.
To provide a multidimensional understanding of a patient’s risk, functional parameters such as 6-minute walking distance, frailty, or other patient-reported outcomes such as dyspnea, fatigue, and the use of repeated measurements to capture dynamic changes of risk factors instead of static measurements can be considered to improve model performance. 103
There should be concerted efforts to report prognostic models in accordance with the transparent reporting of a multivariable prediction model for individual prognosis or diagnosis framework. Methodological issues such as handling of missing data or appropriate reporting of model performance measures should be addressed to avoid biased estimates.97,98 Discrimination and calibration measures provide a comprehensive understanding of how the model can reliably predict a patient’s probability of death. Discrimination, for example, AUC, is frequently reported in the isolation of other metrics. Calibration is the agreement between predicted risk probabilities produced by the model and observed mortality risk. It provides valuable insights on how well the model performs across the different levels of risk probabilities, indicating whether it tends to over- or underestimate a patient’s risk. 104 Nutter et al. evaluated six prognostic models and found that despite attaining moderate discrimination, mortality risks were underestimated in an elderly cohort of AdHF patients. 27 The generalizability of most models is unknown. Model performance derived from the development cohort tends to be optimistic, but external validation can provide a better understanding of how the model performs in a new population of HF patients. 105
Implementation to clinical practice
Referrals to palliative care should be based on needs. However, given that resources are limited, it may be challenging for health care providers to recognize all needs and disease-based criteria listed in Chang et al. (2020).9,14 Therein lies the advantage of using risk scores. To improve the uptake of prognostic models, they can be embedded into electronic health records so that risk scores can be generated automatically to alert clinicians of the risk of deterioration. In addition, interventions can be implemented if patients are identified as high risk. This includes developing individualized patient-centered care models that integrate early palliative care and cardiac rehabilitation that offer exercise-based training and other psychosocial interventions, which significantly improves patients’ quality of life and reduces hospitalizations. 21 Before deployment of the model, the probability threshold used to classify a patient as high risk must be considered in parallel with other factors such as acceptable rate of error, implications on treatment, care plans, local health care practice, health care resources, and funding mechanisms. 106 If models such as MEDL-XI and HFSS with higher sensitivity or a lower threshold are preferred, more patients will be identified as high-risk patients and would be referred to palliative care.
Accurate prognostication remains essential for directing goals of care and deciding the need for specialist or hospice care. The latter is often guided by prognosis due to resources and funding considerations. These risk models highlight to the health care community that certain patients are at a higher risk of deterioration despite the use of curative treatments. Palliative care should be initiated alongside these treatments by cardiologists, with early advanced care planning discussions for goal setting. Specialist palliative care can be initiated when symptoms become more complex, with a shift in resource utilization to community support. Therefore, these risk models are essential in initiating a process of collaborative care involving cardiologists, palliative care physicians, and the wider health care community.
Strength and limitations
This review enhances our current understanding of risk factors that can influence ACM, aiding the development or the updating of AdHF prognostic models. However, findings should be interpreted with caution. We were unable to account for the magnitude, significance, and direction of all risk factors across the 119 models as some studies only reported the effect size of the key risk factor. An incomplete model presentation hinders the ability of other researchers to reproduce the study findings or validate the model in external populations. The final model should be provided in the form of the original regression equation, including intercept or baseline hazard, to ensure adequate transparency in reporting and accurate interpretation of the results. Most of the studies included used data derived from clinical trials, which may limit the generalizability of these findings to the wider AdHF population. In addition, there were multiple studies stemming from the same HF trials. As each of these studies investigated different risk factors, the concern for publication may be reduced. Most of the studies included in this review were based in acute care settings. It is essential to recognize potential variability in prognostic factors in different care settings. 107 AdHF patients are not exclusively confined to the acute care setting. They are also encountered in ambulatory care settings and there exists a gap in the comprehension of risk factors and models for patients seen in such settings. Therefore, as an area for future research, understanding differences in prognostic factors for AdHF seen across different care settings may offer some pertinent insights in improving palliative care in AdHF. As the models account for ACM, the competing risk of dying from a noncardiac cause cannot be addressed.
Due to the substantial number of articles identified, and with the evolving landscape of care management in this population, we limited the search strategy to 2010–2020. We acknowledge that the search strategy could have been extended till 2023. We posit that the nature of risk factors may not have undergone substantial changes. We performed a rapid search of the literature in PubMed for relevant articles published between October 2020 and December 2023 and two relevant articles were identified.10,108 The variables identified in these articles have already been accounted for in the scoping review (Table 4 and Supplementary Appendix S3).
Conclusion
To enable the early identification of high-risk patients who would benefit from timely palliative care interventions, further research is required to develop new models or validate the existing ones that consider the evolving landscape of AdHF management.
Footnotes
Acknowledgment
The authors thank Yasmeen Munro, medical librarian from the Lee Kong Chian School of Medicine, for her support in generating the research strategy.
Authors’ Contributions
A.H. and T.W.S. obtained funding for the study. The study was conceptualized and the research question was refined by P.K., T.W.S., and A.H. P.K., P.P.G., S.N.H.X., Y.W.F., J.C., L.Z.H., L.T.H., V.H., T.C.K., L.T., A.C.H., T.W.S., and A.H. provided inputs for the search strategy. P.K., P.P.G., S.N.H.X., Y.W.F., J.C., L.Z.H., L.T.H., V.H., T.C.K., A.C.H., T.W.S., and A.H. performed title and abstract screenings. Full-text screening and data extraction were performed by P.K., P.P.G., S.H.N.X., R.T., and J.T. Evidence was synthesized, and the article was written by P.K. All the authors provided inputs to the article.
Availability of Data and Materials
Data extracted from the included articles can be found in the supplementary information.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study is funded by the National Medical Research Council Health Services Research Grant—NMRC HSG (HSRGEoL18may-0003). Grant: National Medical Research Council Health Services Research Grant (HSRGEoL18may-0003). Funding period: December 15, 2019, to January 14, 2024.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.