
Abstract
Background:
Tele-assisted home-based palliative care (THPC) usually fulfills the desire of terminal patients to pass away at home. The overall costs of such a service deserve evaluation.
Objectives:
This study aims to determine health care utilization and costs for cancer patients at the end of life, stratified by THPC service.
Design:
Patients who received THPC were matched 1:1 based on age, gender, year of death, and propensity score with those who did not receive THPC.
Setting/Subjects:
A total of 773 cancer patients passed away in a regional hospital in Taiwan during the period of 2012–2020, of which 293 received THPC.
Measurements:
We measured the rates and costs of outpatient clinic visits, emergency department (ED) visits, hospitalizations, and intensive care unit (ICU) admissions during the last week, the last two weeks and the last month before death. In addition, we estimated the driving times and expenses required for transportation from each cancer patient’s home to the hospital using Google Maps. National Health Insurance (NHI) reimbursements and out-of-pocket expenses were also calculated.
Results:
In comparison with patients without THPC, those who received THPC had a 50% lower likelihood of visiting the ED or being hospitalized, a more than 90% reduced chance of ICU admission, but were four times more likely to obtain their medicines from outpatient clinics. THPC patients had similar out-of-pocket expenditures, approximately half of the NHI costs, and lower rates and costs for ambulance transportation to the ED.
Conclusions:
THPC reduced health care costs for terminal cancer patients in the last week, the last two weeks, and the last month before death, while also increasing the likelihood of patients being able to rest and pass away at home.
Key Message
Tele-assisted home-based palliative care (THPC) reduced health care and transportation costs for terminal cancer patients. THPC decreased the odds of dying in the intensive care unit or from out-of-hospital cardiac arrest.
Introduction
Globally, the burden of cancer continues to increase, exerting tremendous physical, emotional, and financial strains on individuals, families, communities, and health care systems. In 2020, approximately 19.3 million new cases of cancer and 10.0 million cancer-related deaths were reported worldwide. Approximately one in five people are diagnosed with cancer in their lifetime, and about one in ten will die from it. 1 In Taiwan, cancer has been the leading cause of death since 1982. Cancer-related deaths accounted for 29.0% of the country’s total mortality in 2020. 2
Near the end stage of cancer, hospitalizations or visits to the emergency department (ED) are typically necessary to manage multiple symptoms.3,4 High levels of depression, anxiety, and burden have been observed among the caregivers of patients with cancer. 5 ED visits are associated with a high caregiver burden. 6 Patients receiving palliative care are less likely to visit the ED in their final month of life. 7 Specialized home-based palliative care (HPC) reduces the utilization of emergency health care resources for the majority of patients. 8
Previous studies have shown that home is the preferred place of death for most cancer patients.9–12 Patients receiving HPC reported greater improvement in satisfaction with care and had a higher likelihood of passing away at home, especially for cancer patients, without increasing caregiver grief. 13
The National Health Insurance (NHI) of Taiwan has provided coverage for the HPC program since 1996 and hospice ward care since 2009. Currently, we have not yet distinguished between the two terms, palliative care and hospice, when delivering care in Taiwan. If a terminal patient is admitted to the hospice ward, they are responsible for covering the cost of food and nursing care. The NHI covers other expenses. Alternatively, if the patient decides to receive HPC, the nurse (or together with a physician during the first visit and when necessary) will primarily travel by taxi or official car to the patient’s home. Patients are responsible for the cost of transportation to and from the hospital. The NHI covers other expenses. Beginning in 2009, the HPC program required care teams to provide 24-hour emergency telephone consultation services. 14 Instant messaging applications (e.g., LINE®) on electronic devices (e.g., smartphones) have gradually become popular since 2011, replacing telephones owing to their convenience in transferring photos, sounds, and videos, as well as facilitating group discussions. 15 Telehealth (also referred to as telemedicine) specifically involves the use of audio and video technologies to deliver synchronous, interactive care to patients at various locations.16,17 Thus, the service is termed THPC.
Puli Christian Hospital is a regional hospital situated in Puli Town, near the center of Taiwan, and serves the residents of Puli Township and the indigenous people living in nearby villages. As most of these places are in rural areas with many mountains, transporting terminally ill patients to the hospital for treatment usually takes considerable time, energy, and resources. 18 Several studies have provided preliminary evidence of generally positive experiences with telehealth for outpatient palliative care among patients and providers.16,19–21 Over the past two decades, the expansion of THPC services in this hospital has shown that terminal patients receiving this care may have lower risks of hospitalization, intensive care unit (ICU) admissions, or ED visits. This could potentially lead to cost savings for patients, families, and society. However, previous research remains largely inconclusive.22–25 Confounding variables originating from the actual spending (e.g., ambulance services owned by different providers) can partially account for these inconsistencies. 26 Thus, we designed this study to determine the financial impact of THPC on health care utilization and costs for cancer patients at the end of their life. We utilized Google Maps to standardize the quantification of time and money spent on transportation expenses, focusing exclusively on terminal cancer cases. We estimated these figures for the last week, the last two weeks, and the last month before patients’ death and compared the differences between those who received and those who did not receive THPC.
Methods
This study commenced after approval from the Institutional Review Board of the Puli Christian Hospital (IRB B-ER-112-188).
Design, setting, and population
Included in the study were patients who received a death certificate from Puli Christian Hospital from 2012 to 2020, as illustrated in Fig. 1. The identification numbers of all individuals in the electronic medical records were encrypted to protect the patients’ privacy. The date of death, date of birth, gender, address of residence, HPC declaration code, first declaration date, chief medical diagnosis at death, and final hospitalization diagnoses (up to five diagnoses) were collected. The diagnoses were coded according to the International Classification of Diseases, Ninth Revision (ICD-9), Clinical Modification. From this group, we selected individuals who had a primary medical diagnosis of cancer at the time of death or had cancer listed as one of the five diagnoses during their last hospitalization before death. Although we initially intended to match more covariates, our hospital’s limited number of cancer patients, as a regional hospital, prevented us from doing so. Thus, we could only collect 293 pairs using the propensity score method matched 1:1 on gender, age, and year of death among all cancer patients.
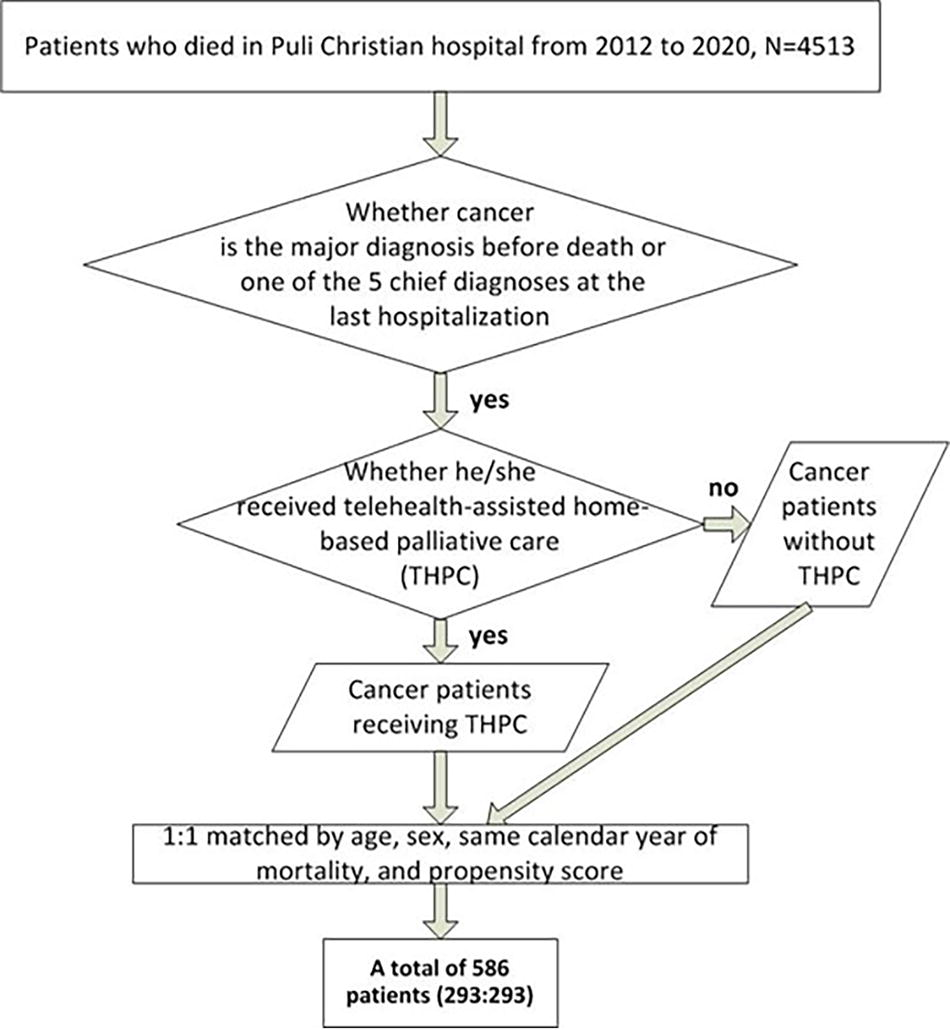
Flow diagram of inclusion of study subjects.
Demographic and clinical factors
The participants’ ages were classified as follows: under 65, 65–79, and 80 years or over. The driving distance and time from each patient’s residence to the hospital were calculated using Google Maps, based on the residential and hospital addresses. Cancer types were classified into seven categories based on the ICD-9 codes as follows: Oropharynx (140–149), Digestive (150–159), Respiratory (160–165), Connective and Breasts (170–176), Urogenital (179–189), Others (190–199), and Lymphatic Blood (200–208). Comorbidities were defined by the ICD-9 codes from the final hospitalization diagnoses (five diagnoses) as follows: Diabetes mellitus (250), Electrolyte imbalance (276), Hypertension (401–405), Congestive heart failure (428), Other heart diseases (393–414 420–429), Dementia (290 331.0), Late effect of cerebrovascular accident (438), Chronic obstructive pulmonary disease (490–496), Cirrhosis (571.2 571.5), Renal failure (585 586), and Pressure injury (707.0).
Health care utilization and expenses
The study accounted for health care utilization and medical-related expenses within the last week, the last two weeks, and the last month before death, which were classified and calculated. Health care utilization encompasses the number of patients and the frequency of uses per 100 patients for outpatient visits, ED visits, hospitalizations, and ICU admissions. The medical-related expenses include those covered by the NHI and out-of-pocket expenses borne by the patients and their families. Expenses were adjusted based on the Consumer Price Index for the year 2021. A rough exchange rate from New Taiwan dollars (NTD) to U.S. dollars (USD) for 2012–2020 was provided in the Supplementary Material (Supplementary Figure S1). 27 The exchange rate fluctuated between 29 and 33 NTD to 1 USD, with an adjustment made in 2021 to 28:1. Google Maps was utilized to determine each patient’s residential address, and the shortest driving distance from their home to Puli Christian Hospital was estimated in kilometers. These distances were then converted into NTD amounts per one-way trip to the outpatient clinic based on taxi fares and ambulance equipped with oxygen and electrocardiogram for ED visits. The final calculation involved summing all transportation and expenses for outpatient visits, ED visits, and hospitalizations. We also calculated the total duration of receiving THPC in days and the number of patients who have received palliative care in the hospice ward.
Statistical analysis
The number of patient health care utilizations was analyzed using McNemar’s test. Owing to skewed distributions, age, driving distance, driving time, number of health care utilizations, and expenses were analyzed using Wilcoxon signed-rank test. All statistical analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC). Since this study involved 43 comparisons, we applied the Bonferroni method to reduce false-positive inferences. That is, we used a p value of less than 0.05/43 = 0.0012 to determine statistical significance.
Results
Demographic and clinical factors
The study involved 773 cancer patients, out of which 293 received THPC. The average duration of THPC was 91 days (with a median of 25 days), and the 95% confidence interval ranged from 64 to 118 days. The distribution is as follows: 63 patients received 1–7 days of care, 43 patients received 8–14 days, 52 patients received 15–30 days, 54 patients received 31–60 days, and 81 patients received ≥61 days. These patients were matched on a 1:1 basis with 293 patients who did not receive THPC for comparison, as summarized in Table 1. There were patients in both groups who received palliative care in the hospice ward. The numbers are 54 (with THPC) and 53 (without THPC). The study found a higher proportion of patients over the age of 80 among those who received THPC. The proportions of different cancer types and comorbidities (except for hypertension) did not appear to be significantly different, even though we did not match based on cancer types and comorbidities. No statistically significant difference was found in distance or driving time between patients with and without THPC (Table 1). About a third of the patients lived in rural areas near Puli Town, with driving distances exceeding 10 km (Fig. 2 and Table 1). Approximately 15% of patients with THPC lived over 20 km from the hospital, and 12% of them had car journeys exceeding 30 minutes to reach the hospital. The longest one-way driving time recorded for a patient to get to the hospital was 109 minutes (Fig. 2). Table 2 summarizes the frequency distribution of places of death, indicating that 78% of patients receiving THPC passed away at home, in contrast to only 9% of those not receiving THPC. Notably, 49 out of 293 patients without THPC died in the ICU or at other hospitals, whereas none of the patients with THPC.
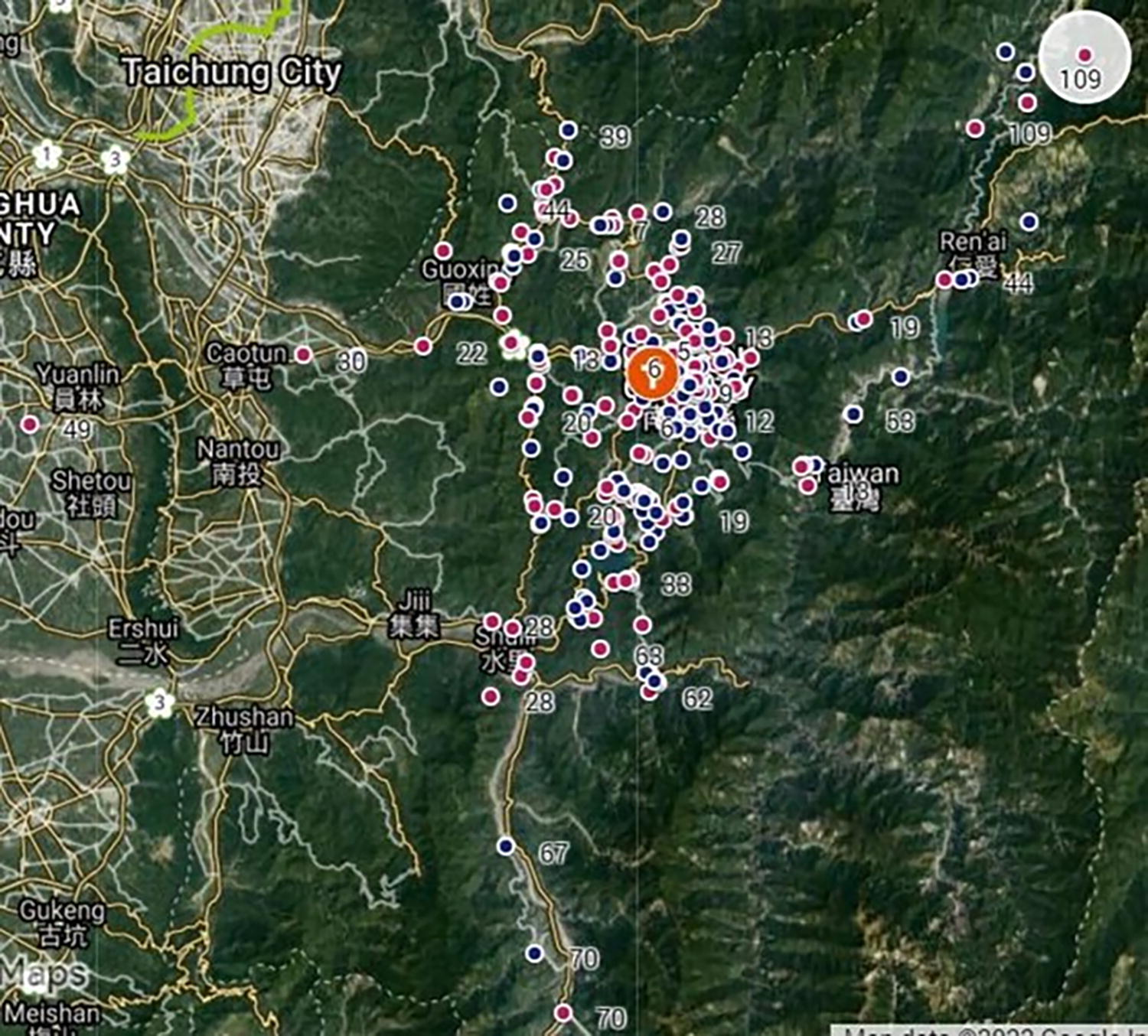
The identified locations (in colored dots; reddish ones for patients receiving THPC, blue ones for non-THPC) and driving times (in minutes) required for ambulance transportation from each cancer patient’s home to Puli Christian Hospital, estimated by Google Maps.
Comparison of Demographic and Clinical Factors Between Patients With and Without Tele-Assisted Home-Based Palliative Care
p value refers to the comparison between patients treated with and without THPC, using
McNemar’s test or
Wilcoxon signed-rank test. The driving times and distances were estimated according to Google Maps.
CI, confidence interval; COPD, chronic obstructive pulmonary disease; CVA, cerebrovascular disease; THPC, tele-assisted home-based palliative care; km, kilometer.
Comparison of the Place of Death of Cancer Patients With and Without Tele-Assisted Home-Based Palliative Care
p value of comparison between patients treated with and without THPC, using Chi-square.
ED, emergency department; ICU, intensive care unit; THPC, tele-assisted home-based palliative care.
Health care utilization and expenses
Within the last week, the last two weeks, and the last month before death, patients under THPC were less likely to visit the ED or be hospitalized, except for the number of hospitalization days during the last month (Table 3). They were also less than one-tenth as likely to be in the ICU, but 4–6 times more likely to obtain their medications from outpatient clinics compared with patients without THPC.
Comparison of Health Care Utilization Within the Last Week/Two Weeks/Month Before Death Between 293 Matched Pairs of Patients With Terminal Cancer, With and Without Tele-Assisted Home-Based Palliative Care
p value refers to the comparison between cancer patients with and without THPC, using Wilcoxon signed-rank test.
Pairs matched with propensity score.
CI, confidence interval; ED, emergency department; ICU, intensive care unit; THPC, Tele-assisted home-based palliative care.
Patients under THPC spent approximately 40% less on health insurance expenses compared with those without THPC, except during the last month (Table 4). However, no significant difference was observed in out-of-pocket medical expenditures. The estimated expenses for ambulance transportation to the ED were significantly lower (Table 5).
Comparison of Medical Expenses in New Taiwan Dollars Within the Last Week/Two Weeks/Month Before Death Between Cancer Patients With and Without Tele-Assisted Home-Based Palliative Care
The exchange rates of NTD can be obtained from the following website: https://www.poundsterlinglive.com/history/USD-TWD. During the study period (2012–2021), 1 USD approximately equaled 30 NTD consistently.
p value refers to the comparison between cancer patients treated with and without THPC, using Wilcoxon signed-rank test.
CI, confidence interval; NTD, New Taiwan dollar; NHI, National Health Insurance; THPC, Tele-assisted home-based palliative care; No. pairs, the number of pairs with the same Match ID as the propensity score.
Comparison of Estimated Transportation and Ambulance Expenses in New Taiwan Dollars Within the Last Week/Two Weeks/Month Before Death Between Cancer Patients With and Without Tele-Assisted Home-Based Palliative Care
The exchange rates of NTD can be obtained from the following website: https://www.poundsterlinglive.com/history/USD-TWD. During the study period (2012–2021), 1 USD approximately equaled 30 NTD.
p value refers to the comparison between cancer patients treated with and without THPC, using Wilcoxon signed-rank test.
Estimating the transportation expenses for outpatient visits based on the patient or family member taking a taxi back and forth (NTD).
Estimating the transportation expenses for emergency treatment based on the patient’s ambulance ride.
CI, confidence interval; ED, emergency department; NTD, New Taiwan dollar; THPC, tele-assisted home-based palliative care.
Discussion
After controlling for confounding variables such as age, gender, year of mortality, types of cancer, and comorbidities, we found that THPC could likely facilitated terminally ill patients to pass away at home, while also reducing ED visits, ICU admissions, and reimbursement costs from the NHI. We have the following arguments to support the above inference. First, no statistically significant differences were found in the proportion of patients receiving palliative care in the hospice ward, the distributions of age (except for those over 80 years old), gender, types of cancer, comorbidities (except for hypertension), distance, or driving time between patients with and without THPC. Higher proportions of individuals over 80 years old and those with hypertension among patients with THPC would typically lead to increased NHI expenses. However, Table 4 shows that the NHI expenses of patients with THPC were still significantly lower than those of patients without THPC. Second, medical care in Taiwan is provided through a single-payer system funded by the NHI, ensuring universal coverage. Beginning in 2009, the coverage rate has been over 99%. 2 Given that a cancer diagnosis is confirmed by two specialists (including one assigned by the NHI) to be registered as a catastrophic illness and exempt from all copayments for both outpatient and inpatient care, the NHI reimbursement comprehensively covers the medical expenses. 28 We further collected expenses paid out-of-pocket and for transportation for comparison (Tables 4 and 5). Third, we selected the statistics from the last week, the last two weeks, and the last month before death because the majority of terminal cancer patients experienced more severe symptoms, such as pain, dyspnea, and fatigue, as they approached the end of life.29,30 At that time, they were generally weak and would require comparable caregiving services. However, providing transportation for them to reach a hospital or clinic was always a challenge for their families and/or caregivers. Without considering the health care utilization of the 18 non-THPC patients who died in other hospitals, we still observed a reduction in the frequencies of ED visits, days spent in the ICU, and hospitalization days as outlined in Table 3. Therefore, we tentatively concluded that THPC led to a decrease in total health care costs.
In the medical records, patients with THPC on average still attended clinic visits several times during the last week, the last two weeks, and the last month before death, which was higher than those without THPC (Table 3). In reality, almost all outpatient visits for patients with THPC were conducted via telehealth assistance (telephone or instant messaging) for diagnosis and prescription to alleviate acute symptoms. Only one family member or caregiver was required to visit the hospital to obtain newly prescribed medications. If the patients already had the correct medicines at home, our THPC staff simply guided them to adjust the dosage for symptom relief through telehealth communication, eliminating the need for their caregivers to come to the hospital. Therefore, THPC could reduce patients’ ED visits or ICU admissions owing to acute symptoms near the end of life, as shown in Table 3. Tables 4 and 5 demonstrate that THPC could decrease NHI reimbursements and estimated ambulance expenses.
Table 2 indicates that THPC increased the likelihood of dying at home and decreased the odds of dying in the ICU or from out-of-hospital cardiac arrest. Given that most THPC patients died at home, THPC could potentially improve the quality of life for these patients and their caregivers or family members. The availability of 24-hour consultation services accompanied with the THPC in Taiwan might also relieve the burden on patients’ families and caregivers.
Puli Christian Hospital served all people of Nantou County, many of whom were aboriginals residing in villages surrounded by high mountains (Fig. 2). One-third of the patients lived more than 10 km away from the hospital (Table 1). If patients were transported by ambulance to the hospital for emergency treatment, the driving speed would typically be slower on mountainous roads compared with urban areas. However, the transportation time and expenses estimated by Google Maps may have taken local irregularities into account. 26 Our 24-hour tele-assisted consultation services provided through THPC could assist patients in managing symptoms promptly at home, potentially avoiding visits to the ED or hospitalization.
Limitations
The following limitations of this study must be acknowledged. First, the THPC and the reference groups each involved only 293 people. Given that many variables could influence the costs of health care services, matching or adjusting every characteristic for the two groups was practically impossible for economic evaluation. The costs considered were based on the viewpoint in the analysis, which further complicated the issue. Nonetheless, we attempted to adopt a societal perspective and matched individuals based on gender, age, and the year of death using propensity score matching. This method resulted in two comparable groups with similar access to medical technology and acceptance of palliative care. Secondly, the longest driving distance in our samples was approximately 65 km, and the longest driving time was about 1 hour and 50 minutes. These distances and times may not be representative of patients residing in urban areas of Taiwan. Therefore, the conclusion drawn from our study may not be directly applicable to other urban hospitals. However, providing THPC services would significantly reduce the transportation inconvenience associated with medical care. Moreover, the utilization of advanced telehealth technology, which enables the transmission of medical data such as photos, sounds, and videos, as well as facilitates group discussions, further enhances this service. Thus, our findings could be applied to other regions with similar conditions, especially to indigenous peoples in Taiwan, in order to reduce health disparities. Third, although 18 patients without THPC died at other hospitals, the median and overall utilization of emergency or inpatient care for patients with THPC were still lower than those of patients without THPC, indicating consistently reduced visits to the ED and hospitalizations under THPC. Fourth, we did not record the mode of transportation used by each patient upon arrival at the hospital. This makes it challenging to determine the appropriate method for comparing transportation costs. In Taiwan, individuals near the end of life are typically transported to emergency services by ambulance. If their conditions are relatively stable, patients in the non-THPC group would usually be escorted to the clinic by either a taxi or a family member’s car. In contrast, THPC patients would first communicate with our service professionals through telephone or instant messaging apps (such as LINE®), followed by sending a family member to ride a motorcycle to the clinic office and back to receive prescription medications. In general, riding a motorcycle is more fuel-efficient, and 71% of travel distances are within 10 km (Table 1). In this study, we conservatively assumed that family members of the THPC group reached Puli Christian Hospital by taxi. This assumption could potentially overestimate transportation costs for this group, but it would not alter the conclusion.
Conclusion/Implications
After standardizing the quantification method for costs, including ambulance transportation, we concluded that THPC reduced the care costs of terminal cancer patients in the last week, the last two weeks, and the last month before death. It also significantly increased the chances of patients resting and passing away at home, which might improve their quality of life. Our empirical evidence could be applied to regional hospitals that serve rural areas and suburban townships. As the current administration of bundled payments for THPC in Taiwan’s NHI system did not fully consider the provision of 24-hour telehealth services, the incentives for providers were not high, especially among privately owned general hospitals. Future collections of the aforementioned data are necessary for reimbursement adjustments and the long-term sustainability of these services.
Footnotes
Acknowledgments
The authors are very grateful to Puli Christian Hospital for providing the dataset used in this study. This study is partially funded by the National Science and Technology Council of Taiwan (NSTC 112-2627-M-006-002).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study is partially funded for Open Access Publication by the National Science and Technology Council of Taiwan (NSTC 112-2627-M-006-002).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.