
Abstract
Background:
More than 50% of patients worldwide die in hospitals and end-of-life care is costly. We aimed to explore whether support from the palliative team can influence end-of-life costs.
Methods:
This was a descriptive retrospective case–control study conducted at a Czech tertiary hospital. We explored the difference in daily hospital costs between patients who died with and without the support of the hospital palliative care team from January 2019 to April 2020. Big data from registries of routine visits were used for case–control matching. As secondary outcomes, we compared the groups over the duration of the terminal hospitalization, intensive care unit (ICU) days, intravenous antibiotics, magnetic resonance imaging/computed tomography scans, oncological treatment in the last month of life, and documentation of the dying phase. Standard descriptive statistics were used to describe the data, and differences between the case and control groups were tested using Fisher's exact test for categorical variables and the Mann–Whitney U test for numerical data.
Results:
In total, 213 dyads were identified. The average daily costs were three times lower in the palliative group (4392.4 CZK per day = 171.3 EUR) than in the nonpalliative group (13992.8 CZK per day = 545.8 EUR), and the difference was probably associated with the shorter time spent in the ICU (16% vs. 33% of hospital days).
Conclusions:
We showed that the integration of the palliative care team in the dying phase can be cost saving. These data could support the implementation of hospital palliative care in developing countries.
Introduction
There are several specialist palliative care services in the Czech Republic. Medical care in inpatient and home hospices was proven cost-effective by pilot projects of the ministry of health 1 and is paid by insurance companies, so they are widely available across the country. Hospital-based consult teams are quite new to the Czech Health System. The first hospital palliative care consultation teams were established in 2016 and play a leading role in implementing palliative care in Czech hospitals. The palliative care team of the Faculty Hospital Kralovske Vinohrady in Prague is one such team.
Although hospital palliative care teams are developing rapidly in the Czech Republic, most of them provide their services with substantial grant support from private donors. Many central and eastern European countries face very similar problems, and data on the economic aspects of hospital-based palliative care are sparse in this region. 2 Differences in funding mechanisms may, in fact, drive differences in the type of services, as well as the number of patients served and their disease trajectory. 3
According to a regular public opinion survey conducted in the Czech Republic, 78% of Czech people want to die at home. The hospital is not a preferred place of death for most patients, but >50% of patients worldwide die in hospitals. Palliative care in hospitals can be provided in a dedicated palliative care unit or more commonly by a specialist palliative care consulting service. Patients are indicated to the palliative care when their symptom burden and needs are too complex to be managed by their primary team. Patients indicated to palliative care suffer mainly from cancer and patients dying from organ failure or frailty receive palliative care at far lower rates. 4 Medical and ethical dilemmas at the end of life arise as opportunities to prolong life increase.5,6
Specific treatments and diagnostic procedures can be inappropriate and not beneficial to dying patients.7,8 Intensified therapeutic and diagnostic procedures are sometimes performed during the dying phase despite their limited clinical value and the substantial health care costs. 8 According to some studies, costs are highest in the dying phase. 9 Integration of palliative care in hospitals is associated with not only clinical but also economic benefits.10–13 According to studies in the United States, cost savings were largely driven by a significant difference in hospital readmission costs, reduction of emergency department visits, and reduced pharmacological costs. 14
A study using national data from New Zealand found that patients in their last month of life used twice as much medication as age-matched survivors, 15 and specialist palliative care involvement was associated with lower medication costs.16,17 For patients who died in hospital, palliative care consultation was associated with even higher cost savings than for those who were discharged. 18 The patients with a palliative care consultation in the intensive care unit (ICU) had reduced length of stay and lower costs when compared with those without the palliative care consultation; mortality between the two groups was not significantly different. 19
In contrast, some high-quality studies failed to prove any significant difference in hospital costs between the groups with and without palliative care intervention.20,21 However, the applicability and generalizability of evidence are uncertain due to the small sample sizes, short duration, and limited modeling of costs and effects of these studies. Economic evaluations with larger sample sizes are needed, inclusive of the diversity and complexity of palliative care populations in different countries.
Our study aimed to determine whether integration of the hospital palliative care team at the end of life can prevent the use of burdensome diagnostic and therapeutic procedures and explore whether integration of hospital palliative care teams at the end of life can prevent transitions to intensive care and lower health care costs in the European context.
Methods
Design
We used a case–control observational retrospective study design. The differences in the end of life between the two groups of patients with (palliative care group) and without (nonpalliative care group) the support of the hospital palliative care team were compared. We retrospectively analyzed and documented data from paper and electronic medical records of terminal hospitalizations and bills to insurance companies. Study design was approved by Institutional Review Board of the Faculty Hospital Kralovske Vinohrady in Prague (number EK-VP/62/0/2019).
Setting
The Faculty Hospital Kralovske Vinohrady is a tertiary university hospital in Prague with 1200 beds, serving a catchment area of ∼300,000 inhabitants.
The hospital's palliative care team is one of the most developed teams in the Czech Republic and plays a leading role in the implementation of specialist hospital palliative care in the country.
Participants
All 1581 inpatients who died between January 2019 and April 2020 were eligible for the study. A total of 213 patients were supported by the hospital palliative care team during the dying phase. They were matched with similar controls from all deceased patients who were not supported by the team. Routine data from the national death registry and national registry of hospital activity were used for the matching. Propensity score matching was used to control for variation in age group (decades), gender, Charlson comorbidity index, and diagnosis recorded on the death certificate.
Data collection
Data were collected from paper and electronic medical records. Three researchers, all physicians (two internists and one oncologist), analyzed the records of the deceased patients. The variables were inserted into a prepared template. When the semiqualitative data (documentation of the dying phase) were analyzed, content analysis of the written data was carried out. Economic data were collected from hospital bills to the insurance companies.
Variables
Calculation of the total daily costs of a terminal hospitalization and determination of their difference between the control and clinical group were the primary outcomes. There are standardized costs for each procedure in the insurance company's price list. The most exact estimate of the daily costs is possible by counting all the costs of diagnostic and therapeutic procedures documented in medical records (monetary value paid for the medical performance by insurance company) and adding all prices of separately charged drugs and materials.
The secondary outcomes were the length of the terminal hospitalization, days in the ICU, the use of intravenous (IV) antibiotics, chemotherapy and radiotherapy in the last month, and the number of costly diagnostic procedures (computerized tomography [CT]/magnetic resonance imaging [MRI] scans).
Another secondary outcome was the difference between the groups in documenting the death of the patient. Content analysis of the words referencing the dying phase was approved before data collection by consensus of all three researchers and the project leader.
Approved words and phrases used for the dying phase documentation were “dying patient,” “terminal phase,” “terminal disease,” “patient with prognosis in hours/days,” “infaust prognosis,” “patient in the end of life,” and “patient ante finem.” If they were found in medical records, YES was inserted into the prepared table in the “Dying phase documented” column.
All data were inserted into an Excel chart made for this purpose.
Data analysis
The geometric mean and logarithmic transformation of hospital costs were used for power analysis and sample size calculation because of the asymmetric distribution of the data. We used the average terminal hospitalization costs of 50000.00 CZK (1960 EUR) for power analysis calculations.
A total of 195 patients in each group were needed to demonstrate a cost difference of 20% (10000.00 CZK = 392 EUR) between the groups with a significance level of 0.05 and a power of 0.8. We used the PS: Power and Sample Size Calculations (version 3.0).
Standard descriptive statistics were used to describe the data. Numerical variables were described using the mean, standard deviation, and 95% confidence interval. Categorical variables were described using absolute and relative frequencies of categories (percentages).
The statistical significance of differences between the clinical and control groups was tested by Fisher's exact test for categorical variables and the Mann–Whitney U test for numerical data.
The results were considered statistically significant at the level of alpha <0.05 in all applied analyses. Analyses were performed using IBM SPSS Statistics 25.0.0 (IBM Corporation, 2017).
Results
Participants
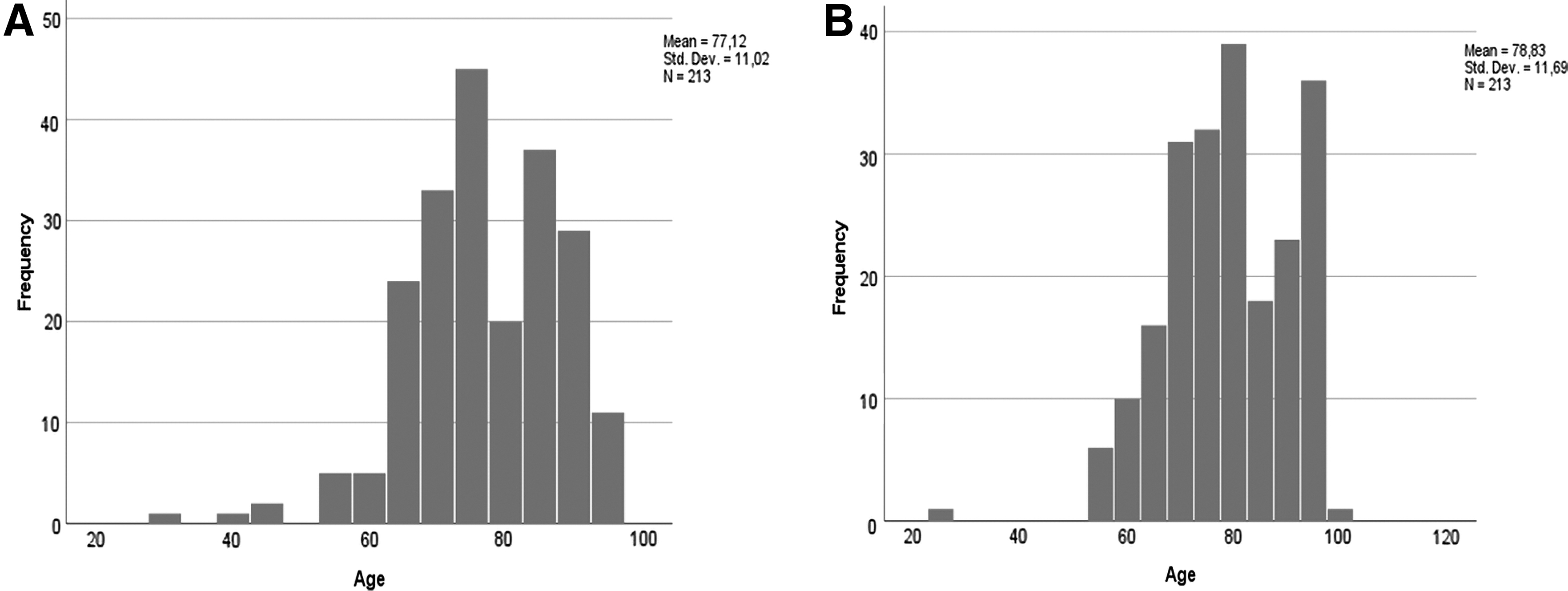
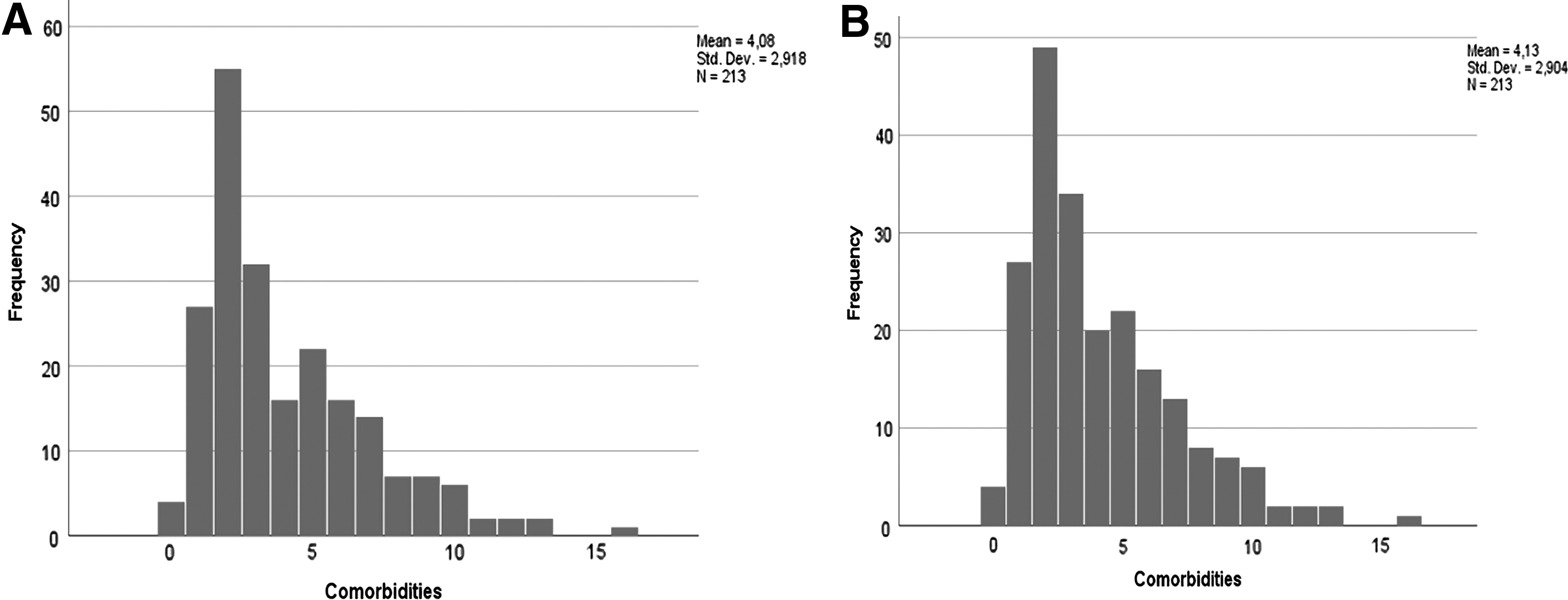
All 213 decedents who received the support of the palliative care team in the measured period and 213 controls out of a total of 1581 decedents were included in the study (their demographics are given in Table 1). Most of them had a main oncological diagnosis reported on their death certificates (Table 1). All participants died during the study period from January 2019 to April 2020. They were mostly elderly, with a higher number of comorbidities (Table 1 and Figs. 1A, B and 2A, B).
Participant Characteristics
Cost and group differences
We calculated all the costs of terminal hospitalization, which was the primary outcome of the study. There was no significant difference between groups in the total costs due to the nonparametric distribution of cost values, with the majority of them around the mean. In contrast, 73 outliers (17%) had hospital costs exceeding double the mean value. More outliers (47 patients, 64%) with extremely expensive hospitalizations were in the nonpalliative group (Fig. 3). The average daily costs were three times lower in the palliative care group (4392.4 CZK = 171.3 EUR per day) than in the nonpalliative care group (13992.8 CZK = 545.8 EUR per day, p ≤ 0.001), and there was a significant difference in the daily hospital costs exceeding 10000.0 CZK (p ≤ 0.001) (Table 3 and Fig. 4).
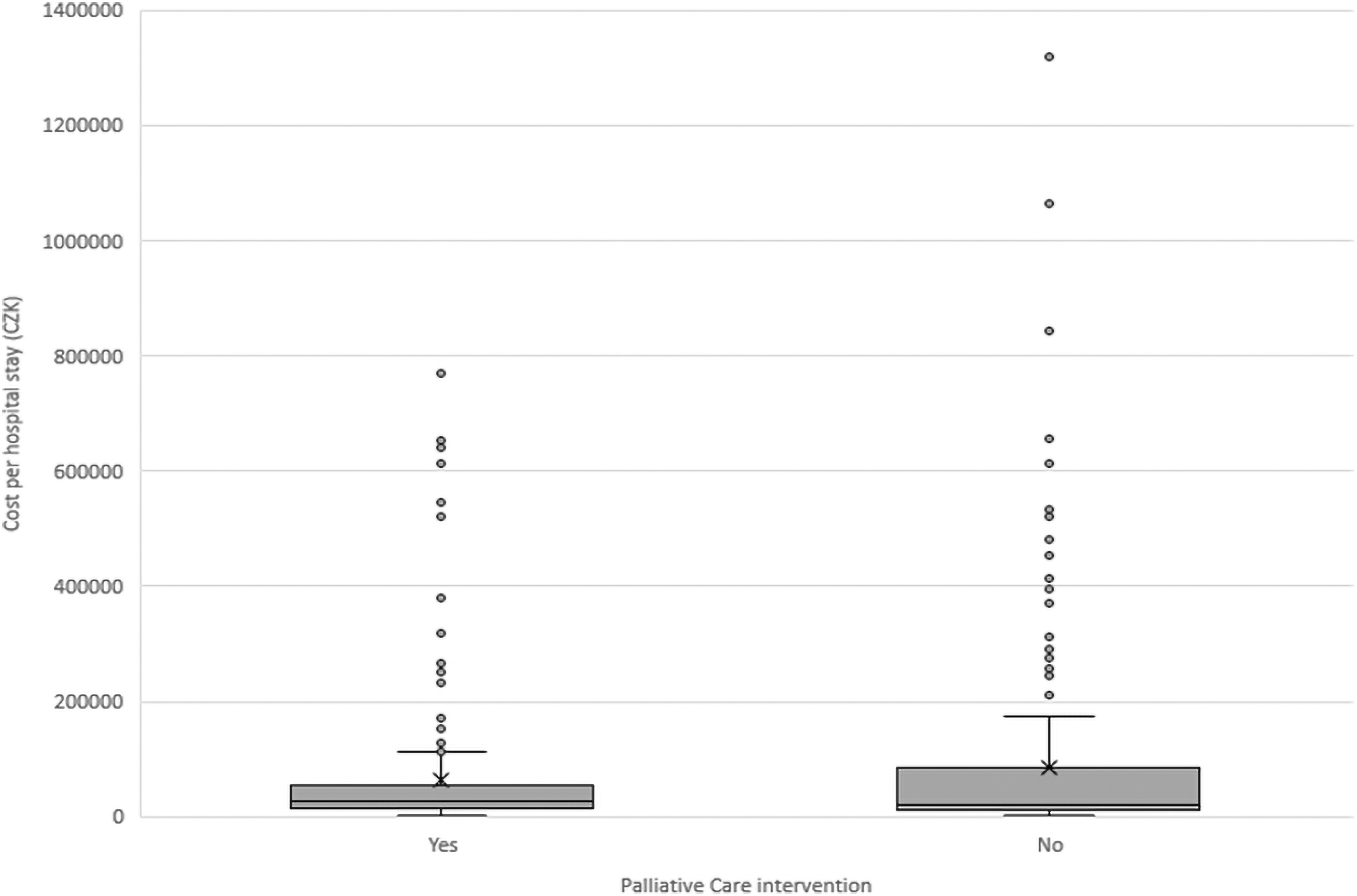
There was no significant difference between groups in the total costs due to the nonparametric distribution of cost values, with the majority of them around the mean. More outliers with extremely expensive hospitalizations were in the nonpalliative care group.
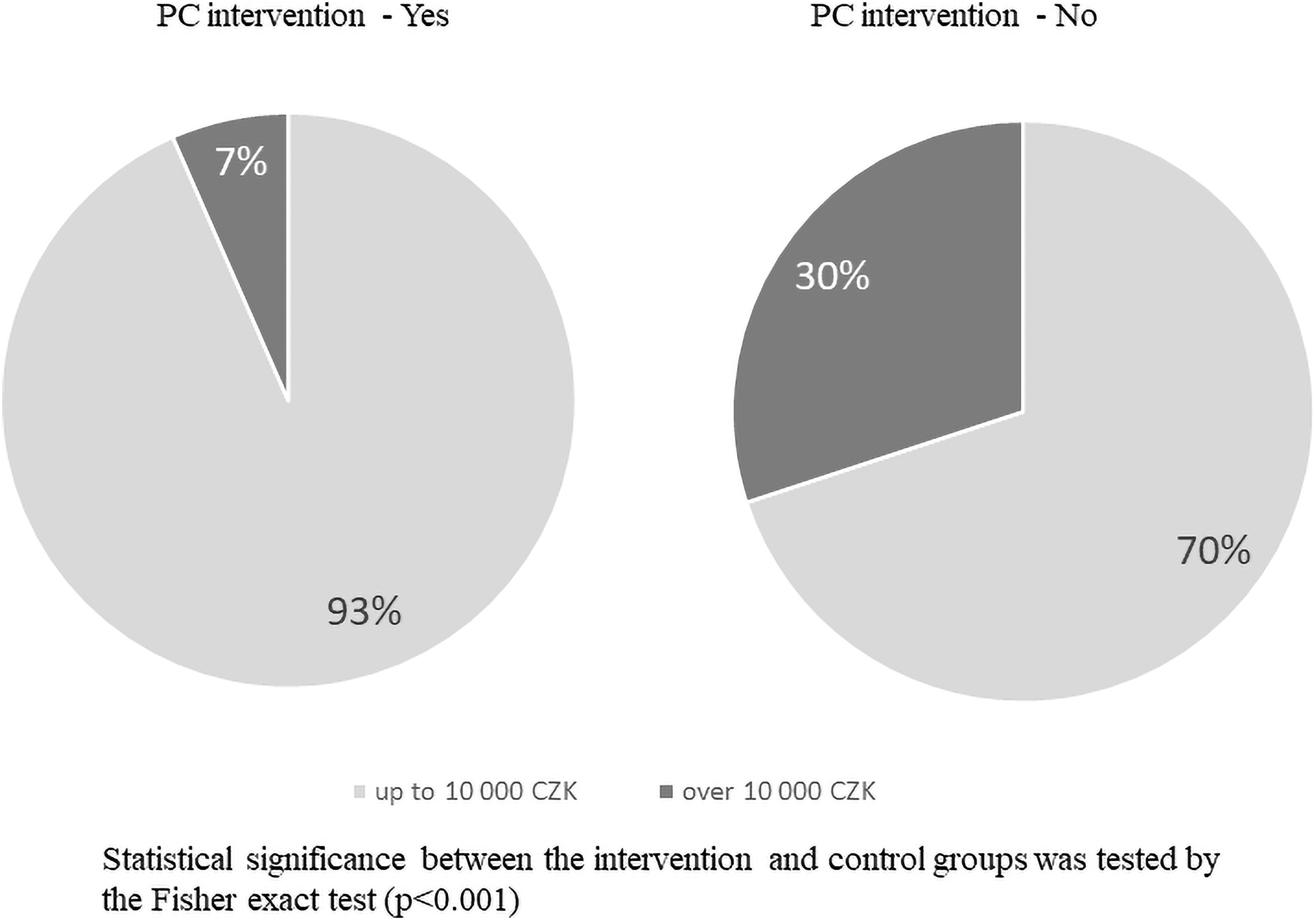
There was a significant difference in the daily hospital costs exceeding 10,000 CZK between palliative care and nonpalliative care groups (7% vs. 30%, respectively).
Chemotherapy and radiotherapy in the last month of life were used similarly, without any significant differences between the cases and controls (Table 4). We also did not observe any significant differences in IV antibiotic use (Table 3). The use of diagnostic MRI and CT scans was also similar, with no significant differences (Table 3).
Hospitalization
We demonstrated a significant difference in the length of terminal hospitalization between the groups. Integration of the palliative care team was associated with significantly shorter terminal hospitalizations (mean = 14.3 days in the palliative care group vs. 18.4 days in the nonpalliative care group, p ≤ 0.001) (Tables 2 and 3).
Length of Hospital Stay
Differences in Costs and Costly Diagnostic and Therapeutic Procedures
CT, computerized tomography; ICU, intensive care unit; IV, intravenous; MRI, magnetic resonance imaging.
Patients who received palliative care interventions spent significantly less time in the ICU (16% of the hospital days in the palliative care group vs. 33% in the nonpalliative care group, p ≤ 0.001) (Table 3).
The context of care was clearer in the palliative care group because 62.4% of patients had been written as dying in their medical records compared with only 30.5% in the nonpalliative care group (p ≤ 0.001) (Table 4).
Differences in Oncological Treatment and the Documentation of the Dying Phase
Discussion
Main findings
This study shows that the integration of the hospital palliative care team during the dying phase has the potential to reduce health care costs. The daily costs were three times lower in patients supported by the palliative care team. The cost savings were associated with a lower number of extremely expensive hospitalizations and fewer days spent in the ICU in the palliative care group compared with their matched controls. Moreover, twice as many patients in the palliative care group had the dying phase documented in their medical records compared with the nonpalliative care group.
Strengths and limitations
To our knowledge, this is the first study to examine cost savings related to hospital palliative care interventions not only in the Czech Republic, but also in the central and eastern European regions. The large sample size (n = 213) increased the strength of the results. Patients of different age groups, cancer types, and noncancer diagnoses were included, and they were properly matched using routine national data from registries and propensity scores; therefore, the biases were reduced to a minimum.
There are also several limitations to this study. The one-center study had limited external validity. In addition, including just dying patients could have been a source of measurement bias. The retrospective study design limits the richness of data; especially in the dying phase documentation, if death was not documented in the records, it does not imply that it was not discussed with the patients and staff. The semiqualitative assessment of the dying phase in medical records and the words used to describe the dying process could have been biased by the researchers. We organized monthly meetings of all three researchers and the project leader to clarify discrepancies and approve a unified method of data collection and content analysis.
Implications for practice
Financial resources can be a significant barrier to the development of palliative care not only in the Czech Republic but also in many other countries. The supporting evidence that hospital palliative care can be cost saving and lower the number of ICU days in the dying phase and number of patients with expensive end-of-life hospitalizations can help when advocating and negotiating with stakeholders. It can promote the integration of palliative care in hospitals in middle- and low-income countries.
Future research
Efforts are ongoing to repeat our study design and include more Czech hospitals to improve the generalizability and strength of the study. Economic evaluation studies in palliative care are available mostly from English-speaking countries and show conflicting results. Cost-effectiveness was proven in palliative home care services in large multicentric studies.22–24 However, some studies did not show significant results mainly in hospital settings.20,21 Most of those with positive impact of palliative care on cost savings in hospitals were conducted in the United States, the United Kingdom, or Ireland.14,22,25
Health systems in non-English-speaking countries can be different and smaller studies in some European countries mentioned in this study failed to prove any benefit on cost savings in hospital palliative care services. 26 More multicenter international and country-specific studies on the cost-effectiveness of hospital palliative care interventions are still needed to increase the evidence in this field.
Conclusion
Our findings suggest that hospital palliative care teams can help provide cheaper end-of-life care. The cost savings are probably associated with the fact that patients with palliative team support have significantly fewer days spent in the ICU and shorter terminal hospitalizations. Moreover, palliative care intervention may help define the context of care as the dying phase is more often documented in medical records when patients are supported by the palliative care team.
Ethical Statement
This research project was performed in accordance with the Declaration of Helsinki and approved by the ethics committee of the Faculty Hospital Kralovske Vinohrady in Prague (number EK-VP/62/0/2019). All methods were performed in accordance with the approved study protocol and ethical guidelines. Informed consent was obtained from the next of kin of the deceased patient.
Data Sharing Statement
All anonymized data generated or analyzed during this study are included in this published article and its supplementary information files.
Footnotes
Authors' Contributions
Conception and design of the study were carried out by Z.K. and J.S. Administrative support was provided by J.S. Provision of study materials or patients was taken care of Z.K. Collection and assembly of data were done by M.K.B., M.M., and K.H. Data analysis and interpretation were done by J.S., P.K., and Z.K. Article writing was done by all authors. Final approval of the article was by all authors.
Acknowledgments
The authors thank the Czech Society of Palliative Medicine, particularly Ondrej Slama and Martin Loucka, for their valuable comments and recommendations on the study design and their guarantee of the implementation of the study results in practice. The authors also like to thank Ivan Rychlik and Martin Havrda, who are the heads of the internal department, for their general support of the research team. We thank Editage (![]() ) for English language editing.
) for English language editing.
Funding Information
This study was supported by the Technology Agency of the Czech Republic program ÉTA3 grant called Dying Matters [Grant No. TL03000709].
Author Disclosure Statement
No competing financial interests exist.