
Abstract
Background:
Pain is one of the most common symptoms in cancer patients. The Japanese Society for Palliative Medicine (JSPM) first published its clinical guidelines for the management of cancer pain in 2010. Since then, more research on cancer pain management has been reported, and new drugs have become available in Japan. Thus, the JSPM has now revised the clinical guidelines using a validated methodology.
Methods:
This guideline was developed through a systematic review, discussion, and the Delphi method, following a formal guideline development process.
Results:
Thirty-five recommendations were created: 19 for the pharmacological management of cancer pain, 6 for the management of opioid-induced adverse effects, and 10 for pharmacological treatment procedures. Due to the lack of evidence that directly addressed our clinical questions, most of the recommendations had to be based on consensus among committee members and other guidelines.
Discussion:
It is critical to continue to build high-quality evidence in cancer pain management, and revise these guidelines accordingly.
Introduction
Pain is one of the most common symptoms in cancer patients. Unrelieved pain distresses patients and affects their function, their social and psychological well-being, and overall quality of life. Pain is experienced by 55% of patients undergoing anticancer treatment and 66% of patients with advanced, metastatic or terminal disease. Moderate-to-severe pain (numerical rating scale [NRS] score ≥5) was reported by 38% of all cancer patients. 1 A meta-analysis of Japanese cancer patients found pain was reported in 52% of outpatients and 51% of inpatients, with moderate or severe pain reported in 15% of outpatients and 33% of inpatients. 2 Undertreatment for pain remains an issue worldwide and in Japan. A meta-analysis reported that cancer pain was undertreated in 45% of Japanese cancer patients. 2
Several clinical guidelines have been published and revised worldwide to improve the quality of pain management in cancer patients.3–7 The Japanese Society for Palliative Medicine (JSPM) first published its clinical guidelines for the management of cancer pain in 2010. 8 Since then, considerable new research on cancer pain management has been reported, and new drugs have become available in Japan. Thus, the JSPM has revised its clinical guidelines using a validated methodology. This article summarizes the recommendations and rationales for this updated clinical guideline for the pharmacological management of cancer pain and its development.
Objectives and target audience of these guidelines
The objective of the guidelines is to establish standard pharmacological management for cancer pain. The Committee decided that the guidelines would apply only to tumor-related pain, not treatment-related or other pain. The intended audience includes all medical personnel who care for cancer patients, including physicians, oncologists, nurses, and pharmacists.
Short summary of the development process
These guidelines were first published in 2010, 8 and minor revisions were made in 2014. Since then, opioids and constipation treatments have become available, and widely used, in Japan (opioid: hydromorphone, tapentadol, methadone; constipation treatments: naldemedine, lubiprostone, elobixibat, linaclotide). In addition, the methodology for developing guidelines has been refined. This revision has followed the “Minds Manual for Guideline Development 2017,” 9 as done for many guidelines in Japan. The JSPM committee nominated members for the guideline development Working Practitioner Group (WPG members; consisting of four physicians and an epidemiologist) from a pool of specialists with clinical experience that encompasses multidisciplinary areas (Supplementary Appendix SA1). WPG members set 24 clinical questions that were evaluated externally by patient representatives.
Systematic literature review
The systematic review team (SR team) consisted of 9 physicians and 20 pharmacists (Supplementary Appendix SA2). The clinical questions were assigned to each SR team member by lot to minimize any conflicts of interest (COIs). On January 27, 2019, SR team members performed a systematic literature search for each clinical question using the electronic search function in PubMed, Cochrane Central Register of Controlled Trials, and a Japanese medical literature database using literature search terms. Literature for a clinical question was searched by two people using the same search terms, and results were matched (Supplementary Appendix SA3). Additional manual searches for existing systematic reviews associated with each clinical question were conducted within the Pain, Palliative, and Supportive Care (PaPaS) category of the Cochrane database. Search results were filtered by selecting studies in adult cancer patients, published in English or Japanese, and published in peer-reviewed medical journals. The review only included randomized controlled trials (RCTs) evaluating drugs available in Japan or drugs with similar pharmacological action.
In the absence of an RCT in cancer patients, a comparative study in noncancer patients was used. For each clinical question, the outcomes were defined as patient-reported pain, quality of life, and adverse effects. Qualitative systematic reviews were conducted instead of a meta-analysis using the verified method because of the adopted studies' heterogeneity of outcomes and methodologies. In qualitative systematic reviews, we assessed the risk of bias (selection bias, implementation bias, detection bias, case reduction bias, selective outcome reporting, and early study discontinuation bias, and other biases) and nondirectiveness in addition to the outcomes of each RCTs. Furthermore, we assessed the overall RCTs for risk of bias, nondirectiveness, inconsistency between studies, imprecision, and reporting bias and created a table for each clinical question.
Drafting recommendations and Delphi methods
Based on the evidence table and bias risk table compiled by the SR team, WPG members drafted the recommendations and general background descriptions. The WPG members decided to use an original recommendation table for this clinical guideline, following concepts from the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system to articulate the levels of evidence and the strengths of each recommendation (Table 1). 10 The Guideline Development Group (GDG; consisting of 15 physicians, 2 nurses, and 2 pharmacists) was asked to rate the validity of all statements on a nine-point Likert-type scale from one (inappropriate) to nine (appropriate). After two Delphi rounds and a review by eight external reviewers (three palliative care physicians, one oncologist, one pain clinician, two nurses, and one pharmacist), the final version was established (Supplementary Appendix SA4).
Recommendation Strength and Evidence Quality
COI management policy
All members of the WPG, SR team, GDG, as well as external reviewers, have declared all financial and academic COIs. Any WPG, SR team, and GDG member with a meaningful COI were excluded from participating on panel presentations, reviews, discussions, and voting relevant to the area of the COI.
Recommendations
We created 35 recommendations: 19 for the pharmacological management of cancer pain, 6 for the management of opioid-induced adverse effects, and 10 on pharmacological treatment procedure. Table 2 lists all guideline recommendations and conditions for adaptation of the conditional recommendation. Figure 1 shows an overview and the main algorithm for using these recommendations.
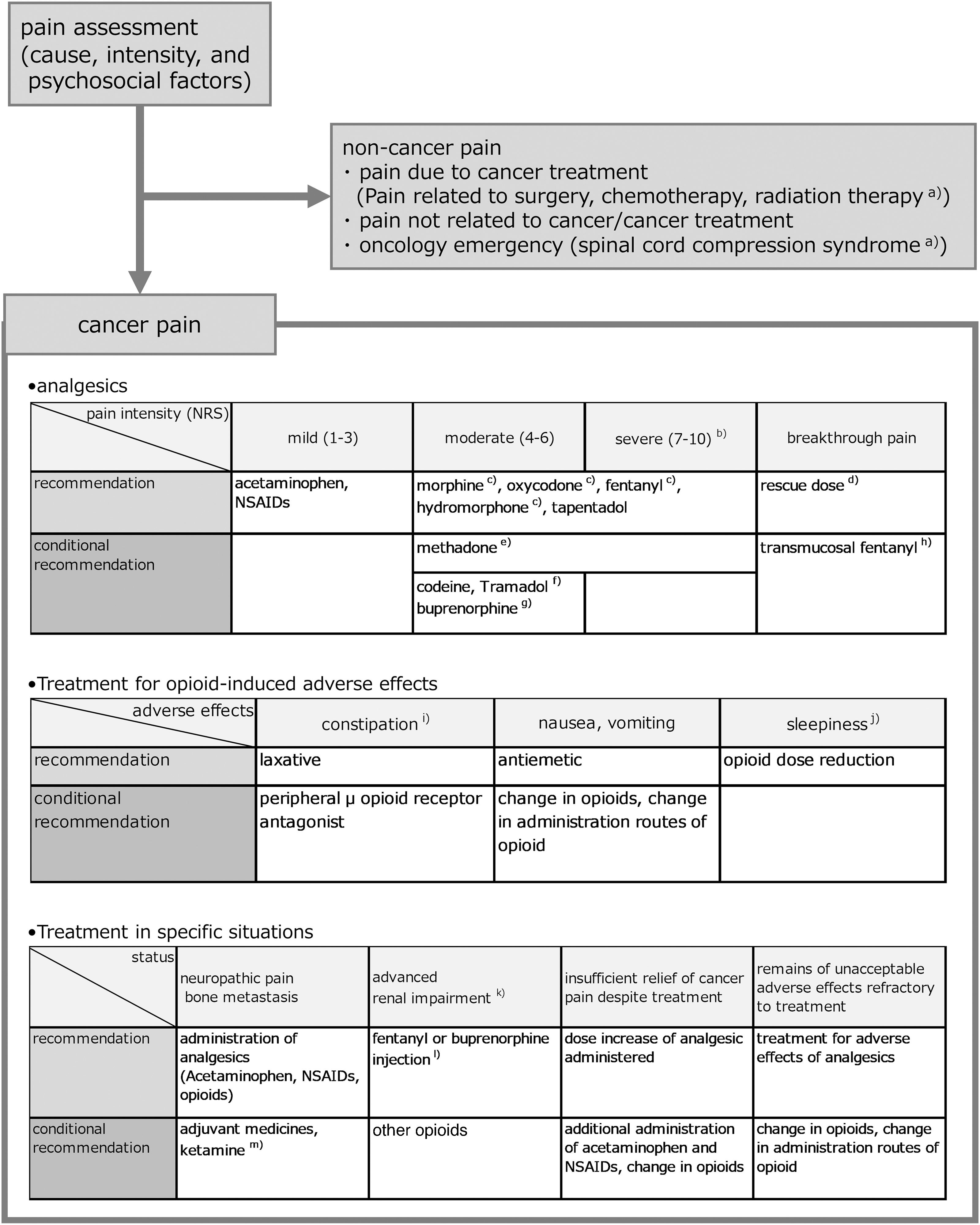
Overview of recommendations for the management of cancer pain. Nerve block and radiation therapy, including subarachnoid analgesia other than pharmacotherapy for analgesia, were excluded from this guideline. Both treatments should be reviewed with a specialist for indications. Bisphosphonates and anti-RANKL antibodies were also excluded from this guideline because they were not administered primarily for analgesia. Laxatives: osmotic laxatives and colonic laxatives. Peripheral mu opioid receptor antagonist: naldemedine. Other constipation medications: lubiprostone, elobixibat, and linaclotide. Antiemetics: metoclopramide, domperidone, antihistamines, haloperidol, prochlorperazine, olanzapine, and the like. Adjuvant medicines: antidepressants, gabapentinoids, anticonvulsants, and antiarrhythmic drugs. Change in opioids: switching or rotating opioid medicines. a)Administer steroids for pain associated with nerve compression, including spinal cord compression syndrome, transient pain exacerbated by radiation therapy, or headache associated with intracranial hypertension due to brain metastasis or cancerous meningitis. b)Opioid administration can start with continuous intravenous or subcutaneous injection for rapid pain relief. c)When administered by continuous intravenous or subcutaneous injection of opioids, PCA can be used. d)Oral morphine/hydromorphone/oxycodone immediate-release formulation, bolus injection of opioid injection, or opioid suppository. e)Despite strong opioid administration other than methadone, consider use in patients with moderate or severe cancer pain remaining. f)Consider use where the administration of strong opioids is not possible due to patient preferences, medical judgment, or medical environment. g)Consider use in the presence of severe renal dysfunction or when it is not possible to administer other strong opioids. h)Fentanyl sublingual or buccal tablets. i)Except for laxatives and peripheral mu opioid receptor antagonists, there is no clear recommendations for other constipation treatments. j)There is no clear recommendation for psychostimulants. k)eGFR <30 mL/min. l)Tramadol, oxycodone, hydromorphone, methadone, codeine, and morphine can be administered carefully. However, codeine and morphine should not be administered if possible. Dosage should be given over a short period and in low doses. m)Consider use in insufficient analgesia despite opioid and adjuvant dose escalation or when it is not possible to escalate the doses of opioid and adjuvants due to adverse effects. eGFR, estimated glomerular filtration rate; NRS, numerical rating scale; NSAIDs, nonsteroidal anti-inflammatory drugs; PCA, patient-controlled analgesia.
Recommendations from the Japanese Society of Palliative Medicine Guidelines
The choice of strong opioids should be based on the physician's experience, preference, and availability at each facility.
Oral morphine/oxycodone/hydromorphone immediate release, bolus of opioid injection, or opioid suppository.
Fentanyl sublingual or buccal tablets.
eGFR, estimated glomerular filtration rate; NSAIDs, nonsteroidal anti-inflammatory drugs; PCA, patient-controlled analgesia.
Pharmacological management of cancer pain
Acetaminophen and nonsteroidal anti-inflammatory drugs
Acetaminophen
There were five RCTs on acetaminophen.11–15 All studies compared high doses of morphine with and without acetaminophen, and the effects of both groups were comparable. There were no trials of acetaminophen and placebo for mild cancer pain. However, due to the widespread use of acetaminophen in Japan and around the world,16,17 the committee concluded that acetaminophen is strongly recommended [Strength of recommendation: 1, Level of evidence: C], and the combination of opioid and acetaminophen is conditionally recommended (Table 2) [2C].
Nonsteroidal anti-inflammatory drugs
There were 40 RCTs on nonsteroidal anti-inflammatory drugs (NSAIDs) for mild cancer pain.18–57 NSAIDs were more analgesic than placebo in one of the three studies comparing NSAIDs with placebo.18–20 In 10 of 14 studies comparing NSAIDs with other NSAIDs, NSAIDs had similar analgesic effects to other NSAIDs.21–25,28–33,55–57 NSAIDs had similar analgesic effects to opioids in seven of nine studies comparing NSAIDs with opioids.26,34–41 In five of eight studies comparing NSAIDs with and without opioids, the combination of NSAIDs and opioids was more effective.42–49 Based on this, the Commission concluded that NSAIDs for mild cancer pain are strongly recommended [1B]. They also conditionally recommended a combination of NSAIDs and opioids [2C]. The recommendation was to evaluate the analgesic effect of NSAIDs after about one week, and if there is no effect, change to opioids instead of other NSAIDs.
Opioids
Morphine
There were 77 RCTs on morphine.35,36,55,58–132 No studies compared morphine with placebo. In 32 of the 40 studies comparing different morphine preparations (oral administration), the analgesic effect was comparable between the different morphine preparations.58–97 In 26 of the 30 studies comparing morphine with other strong opioids, morphine had the same analgesic effect as other strong opioids.103–132 In a systematic review, morphine had a sufficient analgesic effect in most patients (>90%), 133 and adverse effects were constipation, drowsiness, nausea, dry mouth, and vomiting. 134 The committee concluded that morphine for moderate-to-severe pain is strongly recommended [1A].
Hydromorphone
There were eight RCTs on hydromorphone.112–114,135–139 No studies compared hydromorphone with placebo. Hydromorphone and other strong opioids had similar analgesic and adverse effects. Based on this, the committee concluded that hydromorphone for moderate-to-severe pain is strongly recommended [1B].
Oxycodone
There were 26 RCTs on oxycodone.107,118–129,132,137,139–149 No studies compared oxycodone with placebo. In all studies, the analgesic effect of oxycodone was similar to that of other strong opioids. Adverse effects (constipation, drowsiness, nausea/vomiting) were similar to other strong opioids. Based on this, the committee concluded that oxycodone for moderate-to-severe pain is strongly recommended [1B].
Fentanyl
There were 14 RCTs on fentanyl.107–111,121,138,150–156 All RCTs were studies of fentanyl patches, not fentanyl injections. In all 10 studies comparing fentanyl with other strong opioids, fentanyl had similar analgesic effects to other strong opioids.107–111,121,138,150,151,154 In two studies, fentanyl showed lower rates of constipation than morphine.107–111,121 Based on the above, the Committee concluded that fentanyl for moderate-to-severe pain is strongly recommended [1B]. To date, fentanyl patches have been considered high risk in Japan due to their pharmacokinetics, and have not been used as initial opioids. However, due to the simplicity of administrating the fentanyl patch and its milder side effects (constipation) compared with other opioids, the Committee conditionally recommended a minimum dose (6.25 μg/h) of fentanyl patch as the initial opioid [2C].
Tapentadol
There were three RCTs on tapentadol.130,140,157 In all studies comparing tapentadol with other strong opioids, there was no difference in analgesic effect between tapentadol and other strong opioids. Two of the three studies showed no difference in adverse effects between tapentadol and other potent opioids.140,157 Based on this, the Committee concluded that tapentadol for moderate-to-severe pain is strongly recommended [1B].
Codeine
There were 12 RCTs on codeine.37,51,52,119,143,158–164 In seven of the eight studies comparing codeine to placebo, codeine significantly increased analgesia more than placebo.37,52,158–160,162–164 In one study comparing codeine with morphine and oxycodone, codeine was significantly less analgesic. 119 Codeine is inexpensive, and in Japan, it has been widely used in daily practice for cancer pain. Based on this, the Committee concluded that codeine for moderate pain is conditionally recommended [2C].
Tramadol
There were 10 RCTs on tramadol.98–101,161,165–169 In eight of nine studies comparing tramadol with other weak opioids or low-dose strong opioids, there was no difference in analgesic effect between tapentadol and other opioids.98–101,161,165–167,169 Similarly, tramadol had similar adverse effects compared with other weak opioids and low-dose strong opioids.100,101,165,167 Based on the above, the Committee concluded that tramadol is conditionally recommended [2B].
Methadone
There were eight RCTs on methadone.109,115–117,150,170–172 Six of the seven studies comparing methadone with other strong opioids showed no difference in analgesic effects between methadone and other strong opioids.109,115–117,150,170,171 Compared with other opioids, the side effects of methadone (thirst, nausea/vomiting, constipation, somnolence, drowsiness) were similar.109,115,150,151 Previous studies may not have fully evaluated cardiac side effects (QT prolongation and torsades de Pointe) and drug interactions due to few long-term follow-up studies.173,174 There is a lack of experience in the administration of methadone in Japan, and it is limited to those switching from prior opioids. As such, the Committee did not recommend methadone for opioid-naive patients. Based on the above, the Committee concluded that switching to methadone when other opioids are ineffective is strongly recommended [1B].
Buprenorphine
There were 16 RCTs on buprenorphine.103–107,121,131,138,165,175–181 Buprenorphine was more analgesic than placebo177,178 and was comparable to other strong opioids.107,121 Adverse effects of buprenorphine were similar to or less than those of other strong opioids.104,138,175 However, in these studies, buprenorphine was administered in patches, injections, sublingual tablets, oral medications, or an epidural, which differs to the administration method in Japan (patch and injection). The conversion rate of buprenorphine with other strong opioids and the relationship between dose and analgesic effect has not been fully investigated. In addition, there is a lack of clinical experience in Japan, and there is no immediate-release buprenorphine. The dose should be gradually increased from the minimum dose, which is not suitable for rapid and reliable analgesia. 182 Due to the above, the Committee concluded that buprenorphine is conditionally recommended [2B].
Adjuvant analgesics
Antidepressants
There were nine RCTs on antidepressants.53,183–190 In these studies, duloxetine, 189 amitriptyline,183–185,187,190 imipramine,53,186 and fluvoxamine 188 were administered (overlapping). Six of the nine studies reported the effectiveness of antidepressants in cancer pain.183,184,186,188–190 In particular, for neuropathic cancer pain and metastatic bone pain, antidepressants enhanced the analgesic effect of opioids.188–190 Adverse effects of antidepressants were more frequent than placebo. 184 From the above, the Committee concluded that as adjuvant analgesics, antidepressants in combination with opioids are conditionally recommended [2C].
Anticonvulsants or gabapentinoids
There were eight RCTs on anticonvulsants or gabapentinoids.181,191–197 In all studies, anticonvulsants or gabapentinoids were used in combination with strong opioids. Six of the seven studies of gabapentinoid or gabapentinoids in combination with opioids demonstrated effectiveness.181,192,193,195–197 Adverse effects of anticonvulsants or gabapentinoids were more frequent than placebo.191,195,197 From the above, the Committee concluded that anticonvulsants or gabapentinoids in combination with opioids for metastatic bone pain or neuropathic cancer pain as adjuvant analgesics are conditionally recommended [2C].
Antiarrhythmics
There were four RCTs on antiarrhythmics.198–201 All studies compared lidocaine to a placebo. In two of those studies, lidocaine was more analgesic than placebo.198,199 One study reported that lidocaine had more adverse effects than placebo, and another reported that it was comparable.199,200 Committee members agreed from clinical experience that some cancer pain patients would benefit from lidocaine. Based on the above, the Committee concluded that as adjuvant analgesics, lidocaine in combination with opioids for neuropathic cancer pain is conditionally recommended [2C].
Ketamine
There were three RCTs on ketamine with opioids.202–204 One study found that ketamine had a significantly higher analgesic effect than placebo. 203 Intrathecal administration of ketamine and morphine reduced the required dose of morphine compared with morphine alone, but the analgesic effect was not compared. 204 In one high-quality RCT, the analgesic effect of ketamine was comparable to that of placebo for cancer pain that could not be relieved by strong opioids or adjuvant analgesics, and ketamine had more adverse effects than placebo. 202 Ketamine is presumed to be effective against neuropathic cancer pain associated with central sensitization, but has not been clinically tested in patients with this type of pain alone. 205 Some guidelines in other countries do not recommend regular administration of ketamine for neuropathic cancer pain. 4 The Committee concluded that the combination of ketamine and opioids is conditionally recommended [2C]. However, after administration, carefully observe the analgesic and adverse effects, and consider whether to continue administration within a short period.
Steroids
There were 17 RCTs on steroids.206–222 Five studies found that steroids had significantly higher analgesic effects than placebo,207,208,217,219,221 and four studies showed no difference in analgesic effects.209,213,215,220 Steroids had a significant analgesic effect in all four studies where steroids were used in combination with other treatments (opioids, nerve blocks and bone cement, radiation therapy).211,217,218,221 Five of nine studies evaluating adverse effects described only the content of adverse effects, but did not compare them to controls.207–209,211,213 The remaining four studies found no adverse effects of steroids.215,218–220 For most of these, the study period was less than one month, where the adverse effects of long-term steroid administration may not be thoroughly evaluated.223,224 Based on the above, the Committee concluded that steroids for nerve compression pain (including spinal cord compression syndrome), bone pain that worsened transiently after radiation therapy, or intracranial hypertension headache associated with brain metastasis or carcinomatous meningitis, are conditionally recommended [2C].225,226
Management of opioid-induced adverse effects
Constipation
There were 11 RCTs on opioid-induced constipation (OIC).227–237 Due to the lack of RCTs in cancer patients, studies in noncancer patients receiving opioids were also included.227–234 In all five studies on naldemedine, naldemedine significantly improved the symptoms of constipation.231,234–237 In three of the five studies on lubiprostone for noncancer patients, lubiprostone improved constipation compared with placebo.227–229,232,233 Naldemedine and lubiprostone each had more side effects than a placebo. For OIC, osmotic laxatives (magnesium oxide, lactulose) and colon-stimulating laxatives (senna, picosulfate) are commonly administered in clinical practice in Japan. Some guidelines recommend laxatives as the first-line drug for OIC as it is effective in most patients, very safe, and inexpensive.
Peripheral μ opioid receptor antagonists (PAMORA) are recommended for refractory OIC that does not improve with laxatives.238,239 Based on the above, clinical practice of the committee members, other guidelines, 240 and systematic reviews, 241 the Committee concluded that laxatives at the start of opioid treatment (so-called prophylaxis) and for OIC are strongly recommended [1C], and that PAMORA for refractory OIC is conditionally recommended [2B]. The Committee also concluded that other constipation treatments (such as lubiprostone) could not be recommended due to lack of experience with these drugs for OIC.
Nausea and vomiting
There were 18 RCTs on the treatment of opioid-induced nausea and vomiting (OINV).59,62,104,107,123,135,136,153,161,179,242–249 In a study in which antiemetics were routinely administered at the start of opioid treatment, the effect of antiemetics was comparable to placebo. 242 In one study, no clinically significant difference in efficacy was detected because the study was interrupted. 245 Changing opioids did not improve OINV. 246 In comparison between opioids, tramadol and morphine had more OINV.107,123,161,248 In comparison between opioid administration routes, there was no difference in OINV.59,62,120 Administration of antiemetics for OINV is common in clinical practice in Japan. From the above, the Committee concluded that the administration of antiemetics for OINV is strongly recommended [1C]. However, the Committee reached no agreement on which antiemetic drug to recommend, and it was conditionally recommended that opioid switching and changes to the administration route occur when antiemetics do not improve nausea and vomiting.
Sedation
There were four RCTs on the treatment of opioid-related sedation.250–253 In one study comparing caffeine with placebo, caffeine showed no effect on sedation. 250 In three studies on methylphenidate, methylphenidate improved drowsiness, cognitive function, motor function, and mental activity, and the adverse effects were comparable to placebo.251–253 In Japan, only certified physicians and pharmacies can prescribe methylphenidate, and only for narcolepsy, attention-deficit and hyperactivity disorder. Therefore, opioid dose reduction or change is generally performed for opioid-related sedation in Japan. The Committee discussed caffeine and pemoline as alternatives to methylphenidate, but prescribing pemoline was rare, and its effects were unclear. Based on the above, the Committee cannot make explicit recommendations for psychostimulants (methylphenidate, caffeine, pemoline) for opioid-related sedation.
Pharmacological treatment procedure
The selection of specific opioids based upon the pathology of cancer pain
There were five RCTs on the selection of the specific opioids, depending on the pathology of cancer pain (site and type of pain, primary organ).104,125,150,151,254 All five studies found no significant difference in efficacy or adverse effects between the compared opioids. Based on the above, the Committee cannot recommend the administration of specific opioids for cancer pain based upon pathological conditions (primary organ, pain site/type).
Opioids for patients with renal dysfunction
There were no RCTs on opioid selection for patients with severe renal dysfunction. Therefore, observational or cohort studies (seven studies)255–261 and case accumulation studies (five studies)262–266 were reviewed. In these studies, morphine and oxycodone metabolite levels in blood were elevated in patients with renal dysfunction.256–258,260 Several studies concluded that elevated levels of opioids in blood was associated with the adverse effects.258,262,266 On the other hand, studies have shown that fentanyl and hydromorphone have fewer adverse effects.263,266 Nevertheless, there is insufficient evidence and quality research to recommend specific opioids for patients with severe renal dysfunction.
From a previous systematic review, 267 guidelines for opioid administration to patients with renal dysfunction, 268 Japanese clinical guidelines for renal dysfunction, 269 and the experience of committee members, the Committee concluded as indicated in Table 3. For patients with severe renal dysfunction (eGFR <30 mL/min), injections of fentanyl or buprenorphine are recommended [1C]. Careful administration of hydromorphone, oxycodone, methadone, and tramadol were recommended, while administration of morphine and codeine was to be avoided. If unavoidable, administration should be for only a short period with a low dose.
Opioids for Patients with Renal Dysfunction
If the administration is required, start administration with a low dose for a short period.
Start administration with low doses of fentanyl and buprenorphine injections.
The selection of strong or weak opioids as initial opioids for cancer pain
There were three RCTs on strong and weak opioids as initial opioids for cancer pain.102,270,271 In these RCTs, strong opioids were more analgesic than weak opioids as the initial opioid for moderate cancer pain. Regarding the adverse effects of these drugs, the studies yielded inconsistent results. From the above, the Committee concluded that as the initial opioid for moderate-to-severe cancer pain, strong opioids are strongly recommended [1B], and weak opioids are conditionally recommended [2C].
Continuous intravenous or subcutaneous opioid injection for rapid pain relief
There were two RCTs on continuous intravenous or subcutaneous opioid injection for rapid pain relief.90,272 Compared with oral morphine, intravenous morphine could relieve pain faster. 90 There was no difference in the analgesic effect of morphine between subcutaneous injection and intravenous injection. 272 However, both studies used intermittent rather than continuous administrations, and did not directly address the clinical questions. Considering the recommendations of other guidelines4,7 and the clinical experience of members, the Committee concluded that for faster analgesia for severe cancer pain, starting opioids with continuous intravenous or subcutaneous infusion is recommended.
Opioids for breakthrough cancer pain
There were 23 RCTs on opioids for breakthrough pain.244,273–294 Transmucosal fentanyl had a stronger analgesic effect on breakthrough pain than placebo.244,273,274,278,279,281–284,286–289,294 The analgesic effect of transmucosal fentanyl within 30 minutes was stronger than oral morphine immediate-release preparation, but the analgesic effect after 30 minutes was similar. 290 The analgesic effect of morphine injection (intravenous injection, subcutaneous injection) within 30 minutes was stronger than transmucosal fentanyl, but it was similar at 30 minutes. 277 Adverse effects were higher with transmucosal fentanyl compared with placebo.273,279,282,287,289,294 Considering the time to effect, ease of administration, and cost (transmucosal fentanyl is more expensive than rescue drug), the Committee concluded that rescue medicines (oral morphine/oxycodone/hydromorphone immediate release, bolus of opioid injection, or opioid suppository) for breakthrough pain are strongly recommended [1B], with transmucosal fentanyl conditionally recommended when analgesia is delayed or insufficient despite oral rescue medication [2A].
Switching or rotating opioid medicines
There were five RCTs on switching or rotating opioid medicines.123,127,179,249,295 In all five studies, opioid switching relieved pain. However, these studies did not compare the switching and nonswitching groups, and the findings did not directly address the clinical questions. Other guidelines recommend switching opioids when increasing the dose of opioids does not relieve pain as expected, or when adverse effects do not improve sufficiently.3,4 Other guidelines conclude that no clear recommendations can be made for opioid switching and that opioid switching should be tailored to the individual patient's condition. 5 Based on the recommendations of other guidelines3,4 and the clinical experience of each member, the Committee concluded that switching or rotating opioid medicines is conditionally recommended [2C].
Patient-controlled analgesia
There were six RCTs on patient-controlled analgesia (PCA) devices for breakthrough cancer pain.43,296–300 In all six studies, there was no difference in analgesic effect based on the type of opioid and administration method. However, the PCA device was used in both the intervention and control groups, and the study results did not directly address the clinical questions. Considering that PCA devices are commonly used in clinical practice, the Committee concluded that PCA is conditionally recommended when the patient, family, and caregiver had a good understanding of it [2D]. 301
Discussion
This revision is the first major revision since the last edition, published in 2010. The guideline was based on the previously announced guidelines of the European Association for Palliative Care (EAPC), 3 European Society for Medical Oncology (ESMO), 4 National Comprehensive Cancer Network (NCCN), 7 and World Health Organization (WHO). 5
In the previous revision, we recommended the selection of analgesics according to the WHO pain relief ladder. In this revision, cancer pain was classified into three categories using NRS, similar to the guidelines of ESMO and NCCN, and the drug was defined according to the pain intensity, to help general practitioners evaluate cancer pain and select drugs. There was insufficient evidence to discuss the choice of opioids. Most of the evidence is derived from studies during the product development phase, where many have a noninferiority study design. Therefore, similar to WHO guidelines, the Committee did not recommend specific opioids due to a lack of evidence for the superiority of specific opioids and the slight cost difference between opioids in Japan.
Methadone was conditionally recommended for cancer pain that could not be removed with other strong opioids due to a lack of experience in administration. The EAPC, ESMO, and NCCN guidelines state that experts should prescribe methadone. In Japan, methadone was approved in 2013, and it can only be administered by doctors who have completed e-learning. Transmucosal fentanyl for breakthrough pain was selected as a second-line drug because of its high cost (the lowest dose of fentanyl sublingual tablet is five times the price of the lowest dose of immediate-release morphine).
For OIC, general laxatives were recommended as prophylactic and therapeutic agents, similar to the guidelines of EAPC, ESMO, and NCCN, due to sufficient experience with them and low drug prices. Naldemedine was recommended when the laxative effect was inadequate, similar to the ESMO and NCCN guidelines. For opioid-induced vomiting, the previous revision of the guideline recommended prophylactic administration. Due to a lack of evidence and the Committee's agreement, this revision did not recommend prophylactic administration similar to the guidelines of EAPC and ESMO. For opioid drowsiness, EAPC, ESMO, and NCCN guidelines recommend methylphenidate, but methylphenidate is a restricted prescription drug in Japan, and other psychostimulants lack evidence. As such, these drugs were not recommended in this guideline.
Opioid switching is not recommended in the WHO guidelines. However, like the other guidelines, the Committee conditionally recommended opioid switching due to the common clinical practice in Japan. Although the ESMO and WHO guidelines mention the recommendation of bisphosphonates, the Committee agreed not to administer this drug for the primary purpose of analgesia and excluded it from the guidelines.
The most critical limitation in the guideline development process is a general lack of evidence that directly addresses the clinical questions. Several of the recommendations in this guideline are strong recommendations based on the low level of evidence. Many of the studies adopted in systematic reviews had little directness to the actual clinical practice, and many treatments could not be recommended based on the evidence alone. It was necessary to coordinate the actual empirical treatments but customarily widely practiced in Japan, collected through the guideline committee and the external committee members, with the rigorous methodology for handling evidence, such as GRADE. To ensure that even general practitioners who do not specialize in palliative medicine can make better treatment choices, we discussed the certainty of evidence and the balance between benefit and harm, patient preferences and values, cost, and feasibility, and even interventions with a low evidence level were strongly recommended when there was unanimous agreement among the committee members.
It will be necessary to conduct high-quality studies in the area of cancer pain management in the future and continually update this guideline to improve the quality of pain management in cancer patients.
Conclusion
This is the first major revision of the JSPM's pharmacological treatment recommendations for cancer pain, with the goal of directing best practice at this time. Due to a lack of evidence, most of the recommendations were based on a consensus among committee members and foreign guidelines. The most significant change was to classify pain into three categories using NRS: mild (1–3), moderate (4–6), and severe (7–10), and indicate drugs by pain intensity. We recommended acetaminophen and NSAIDs for mild cancer pain and strong opioids for moderate-to-severe cancer pain. No specific strong opioids were presented as first-line drugs. Methadone is recommended only for pain that other opioids do not improve. Switching or rotating opioid medicines is conditionally recommended.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.