
Abstract
Objective:
To assess parental decision-making preferences when caring for a child with serious illness and to evaluate for an association between preferences and parental trust in physicians, and potential modification of this association by parental anxiety or depression.
Methods:
We analyzed cross-sectional data from 200 parents of 158 children in the United States who had life-threatening illnesses and whose attending physicians thought that the parents would have to make major medical decision in the next 12 to 24 months. Parents completed measures of decision-making preferences, trust in physicians, anxiety, and depression.
Results:
Higher reported levels of trust were associated with lower preferences for autonomous decision making (Spearman correlation = −0.24; 95% confidence interval [CI] = −0.36 to −0.01; p < 0.008). Among parents with higher levels of trust, increasing anxiety scores were associated with decreasing preference for autonomy, whereas among parents with lower levels of trust, increasing anxiety scores showed an increasing preference for autonomy (regression coefficient = −0.01; 95% CI = −0.02 to −0.001; p ≤ 0.03).
Conclusions:
Decreasing trust in physicians is associated with a higher preference for autonomous decision making. Parents who have higher levels of anxiety exhibit this association more strongly. Decision support for parents of children with serious illness should use strategies to respect parental decision-making preferences, address potential distrust, and provide mental health support to parents who are anxious or depressed.
Introduction
Parents of children with serious illness often participate in complex decisions about their child's medical care.1–4 Shared decision making between clinicians, patients, and parents or other family members is recommended in both pediatric and adult medical care and includes assessing how much the patient or family member wants to be involved in the decision.5–8 Research has shown that both adult patients and parents of pediatric patients vary in their decision-making preferences with some preferring to make the decisions themselves (autonomous), some wishing to collaborate with the physician, 9 and some preferring that the physician make the decisions (delegate).1,10
Some experts describe shared decision making as a process that allows for all three types of decision-making preferences, namely by modifying the process according to patient or parent preferences. 11 Parents of children with serious illness may experience distress if their decision-making preferences are not respected and they either do not have enough say in the decisions or they are forced to take responsibility for decisions that they do not feel they have the knowledge or expertise to make.12,13 The prevailing models of medical decision making emphasize individual autonomy and omit relational aspects and key psychosocial factors that may influence how much patients and parents want to be involved in decisions.4,14,15
One factor that can potentially influence decision-making preferences is how much the patient or parent trusts their physician.16,17 Higher levels of trust in physicians predict higher levels of adhering to recommended preventive medical care,18,19 and lower levels of trust in physicians predict higher levels of distress in cancer patients over time. 20 One study found that older age, minority status, higher education, and poorer health among patients predicted lower levels of trust in their physician. 21 Another study found that patients with high levels of trust in their physician were more likely to prefer that the physician make decisions, whereas those with low levels of trust were more likely to prefer to make decisions themselves. 22
Trust and parent decision-making preferences are particularly fundamental in the context of serious pediatric illness because of the complex situations, multiple specialists, and the triadic nature of interaction between clinicians, parents, and patients.23,24 Poorly implemented attempts at shared decision making with patients and parents that are not based on decision-making preferences may lead to regret (e.g., the parents feeling responsible if the outcome of the decision is poor), and loss of trust in physicians if parents think the physicians are giving up on the child.13,24 Once parents lose trust in clinical staff, confrontations and adversarial interactions over difficult decisions may become more likely. 25
Mood and psychological distress may also influence both decision making and decision-making preferences.3,26 Parents of children with serious illness report high levels of anxiety and depression.27–30 Parents may experience additional anxiety and distress when making medical decisions for children, especially if there are adverse outcomes.31,32 Anxiety, distress, and time pressure may interfere with their ability to evaluate different options.33–35 Some parents may experience both distress and mistrust when making medical decisions for their child; for example, a qualitative study found that African American mothers of newborns reported frequent anxiety and distrust related to how they were treated by medical staff. 36
In light of the above, we sought to examine in a sample of parents of children with serious illness how parental decision-making preferences are related to their level of trust in physicians. We specifically hypothesized that lower levels of trust would be associated with higher preferences for autonomous decision making. We also hypothesized that parents' preferences would be associated with the presence of anxiety and depression and that this relationship would interact with the effect of trust.
Methods
Study design and participants
Participants were parents in the Decision Making in Serious Pediatrics Illness study, a mixed-method prospective cohort study on parental decision making for children with serious illness conducted at The Children's Hospital of Philadelphia from September 2010 to December 2014. The hospital's Committee for the Protection of Human Subjects approved the protocol for this study.
Parents were defined as the adults who had primary decision-making responsibilities for the index patient and included biological parents, adoptive or foster parents, and members of the extended family. Parents were eligible if their children were patients at The Children's Hospital of Philadelphia; had been admitted to the Pediatric Intensive Care Unit, Neonatal Intensive Care Unit, Cardiac Intensive Care Unit, or had been referred to the Pediatric Advanced Care Team for palliative care services; if the patient's attending physician thought that the patient had a serious illness and the parents would likely have to make a medical decision about a serious or life-threatening event or condition in the next 12–24 months; if their children were not able to make medical decisions because of age or impaired cognitive capacity; and if the parents spoke English.
Parents were not eligible if the parents were deemed by the physician to be emotionally overwrought by the clinical situation, did not speak English, or had lost custody rights; or if the child had died, had been discharged, had experienced a non-accidental injury, or (because this was part of a larger longitudinal study) if the physician thought the child might die within a month or less. The research coordinator approached parents and asked if they were willing to participate in a study of how parents make medical decisions for their children. Parents were asked to complete a 1-hour interview at baseline and a 20-minute interview at 24 months. The data reported in this article reflect only baseline data. Prospective data and additional aspects of the study have been previously reported.37–40
Measures
Parents were asked at baseline to report demographic data. Information about the complex chronic conditions (CCC) of the patients was obtained from medical records. Based on psychological theories of parental decision making, anxiety, and decision making,31–34,41 parents completed scales measuring: trust in physicians (Trust in Physician Scale), 16 and anxiety and depression (Hospital Anxiety and Depression Scale [HADS]).42,43 Parents also completed a scale regarding their preferred style of making medical decisions. The five options were: (1) make the final treatment decision; (2) make the final selection of treatment after seriously considering the doctor's opinion; (3) have the child's doctor and the parent share responsibility for all treatment decisions; (4) have the child's doctor make the final decision after seriously considering the parent's decision; or (5) have the child's doctor make all treatment decisions. 10 We used a version of this scale modified for use in pediatric settings that has been used successfully in previous studies. 1 See Supplementary Data for additional information about these measures.
Statistical analysis
Descriptive statistics and a correlation matrix were calculated for all study variables. The internal consistency of the Trust in Physician Scale was assessed by calculating corrected item to scale correlations and Cronbach's alpha coefficient. We derived the Total Trust Score by creating a sum of all items, after reverse scaling the negatively worded items. Higher values of the Total Trust Score corresponded with higher trust in the physician. The Total Trust Score as a continuous variable was used in all analyses. To display our interactions visually, we showed parents with a higher level of trust (Total Trust values greater than or equal to the median of Total Trust Score) and parents with lower trust (Total Trust values less than the median).
Spearman correlation with 95% confidence intervals (95% CI) and a two-sided test for zero correlation was used to evaluate the association between trust in physician and parent decision-making preference. A scatter plot of trust scores and average trust score versus parent decision-making preference was constructed, to visually display the relationship between trust scores and parent decision-making preference.
Ordered logistic regression was used to evaluate the relationship between parent decision-making preference, trust in physician (Trust Scores), and either self-reported anxiety scores or depression scores. Parent decision-making preference takes value 1 through 5 (with 5 indicating the highest preference for autonomy). The likelihood ratio test was used to test for the presence of an interaction between the level of trust and either anxiety or depression, comparing the full model with the model that excluded the interaction. Analyses were clustered by child to account for the fact that in some cases more than one parent of the same child participated in the study.
All analyses were conducted using Stata version 16.1 (Stata Corp, College Station, TX) with two-sided tests of hypotheses and a p-value <0.05 as the criterion for statistical significance.
Results
We enrolled 200 parents after approaching 295 parents regarding potential participation (68% participation rate). The most common reasons offered for declining to participate included “just don't want to” (n = 25/95, 26% of nonparticipants), “there is too much going on” (n = 21/95, 22% of nonparticipants), and “don't have enough time” (n = 16/95, 17% of nonparticipants).
The demographics of parents and their children are described in Table 1. Of 200 parents of 158 patients who participated, most (68%) were mothers, in the 21–34 age range (56%), non-Hispanic (90%), and white (81%). Most parents were married (86%) and had greater than a high school education (84%). Many parents had full-time employment (50%) and many reported financial hardship (46%).
Demographic and Clinical Characteristics of 158 Children and 200 Parents
Many patients have more than one condition, thus percentages total more than 100%.
Financial hardship defined as having reported having at least some financial difficulties.
The 158 patients were mostly younger than 1 year (69%), male (54%), non-Hispanic (87%), and white (75%). Many had private or employer-based insurance (43%), and many had one or more CCC, with congenital (70%) and respiratory (56%) being the most common.
The baseline scores of the decision-making preferences and the HADS are described in Table 2. The Trust in Physician Scale is described in detail in Table 3 including the item description and the mean response for each question.
Decision-Making Preferences and Hospital Anxiety and Depression Scale
HADS, Hospital Anxiety and Depression Scale; SD, standard deviation.
Descriptive and Psychometric Properties of Trust in Physician Scale
Five-point response scale: 1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree, where a high total score represented trust in physicians. Cronbach's α = 0.88.
Reverse-coded items.
Used for graphs only.
We found that higher reported levels of trust were associated with lower preferences toward autonomous decision making (Spearman correlation = −0.24; 95% CI = −0.36 to −0.10; p < 0.008) (Fig. 1).
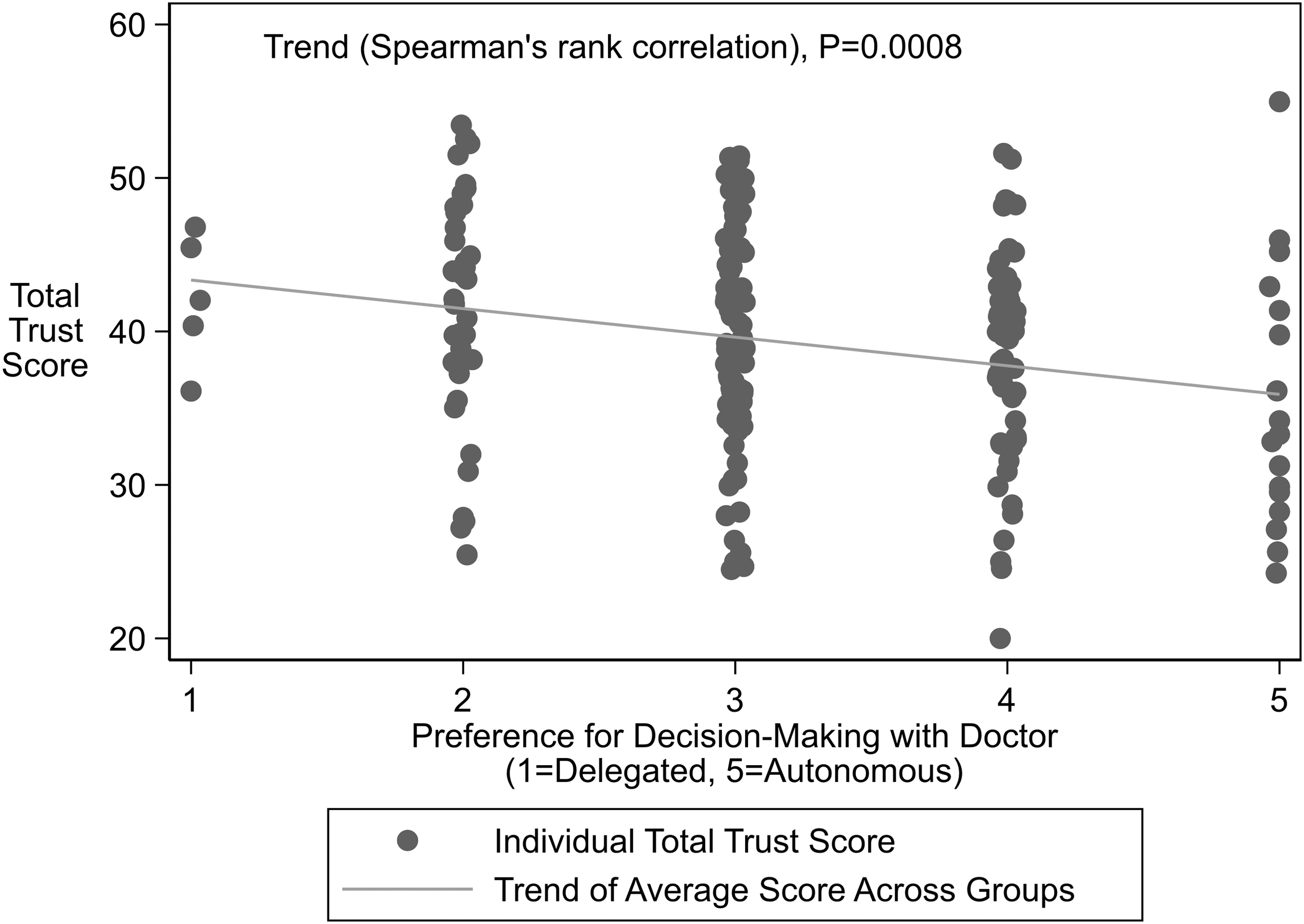
Higher Trust in Physicians Score associated with decreasing preference toward autonomy in decision-making. Higher Trust in Physician Score indicates increased trust in physicians.
Parents' self-reported level of anxiety was not associated with decision-making preference (regression coefficient = −0.004; 95% CI = −0.07 to 0.08; p = 0.9). Level of anxiety and of trust, however, exhibited a statistically significant interaction (regression coefficient = −0.01; 95% CI = −0.02 to −0.001; p = 0.03) relating to decision-making preference (Fig. 2). Among parents with higher levels of trust, increasing anxiety scores were associated with decreasing preference for autonomy, whereas among parents with lower levels of trust, increasing anxiety scores showed an increasing preference for autonomy.
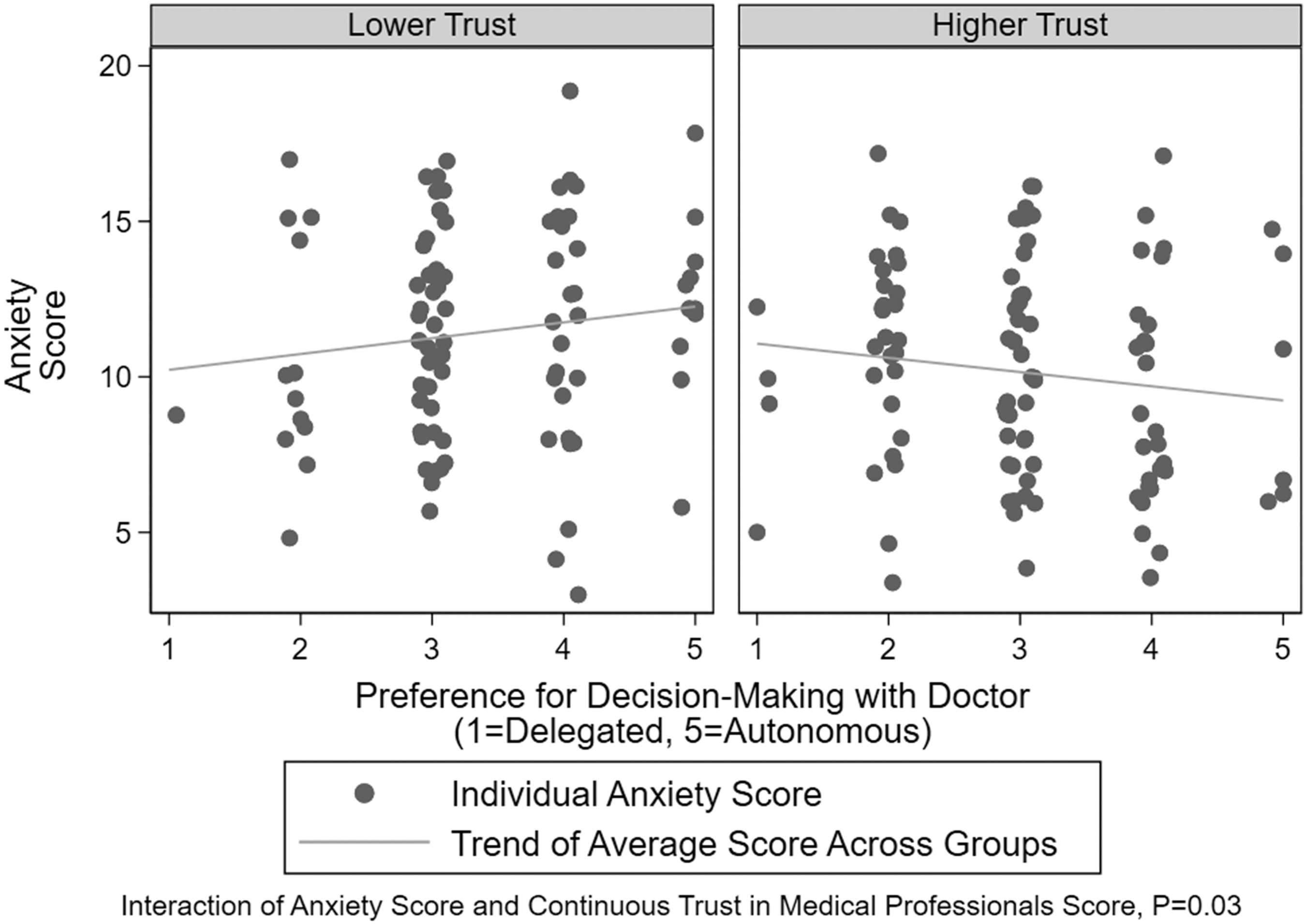
Association of Anxiety Score and Decision-Making Preference modified by level of Total Trust Score. Higher Anxiety Score indicates increased anxiety with 0–7 being a normal score, 8–10 being a borderline abnormal score, and 11–21 as an abnormal score.
Parents with higher self-reported levels of depression tended toward more autonomous decision-making preferences, but not to a statistically significant degree (regression coefficient = 0.07; 95% CI = −0.01 to 0.15; p = 0.07). Compared with the level of anxiety, the level of depression and of distrust trust exhibited a weaker and not statistically significant interaction (regression coefficient = −0.01; 95% CI = −0.02 to 0.001; p = 0.08) relating to decision-making preference (Fig. 3). Among parents with lower levels of trust, higher depression scores were associated with increasing preference for autonomy, while among those with higher levels of trust, depression scores were not associated with preference for autonomy.
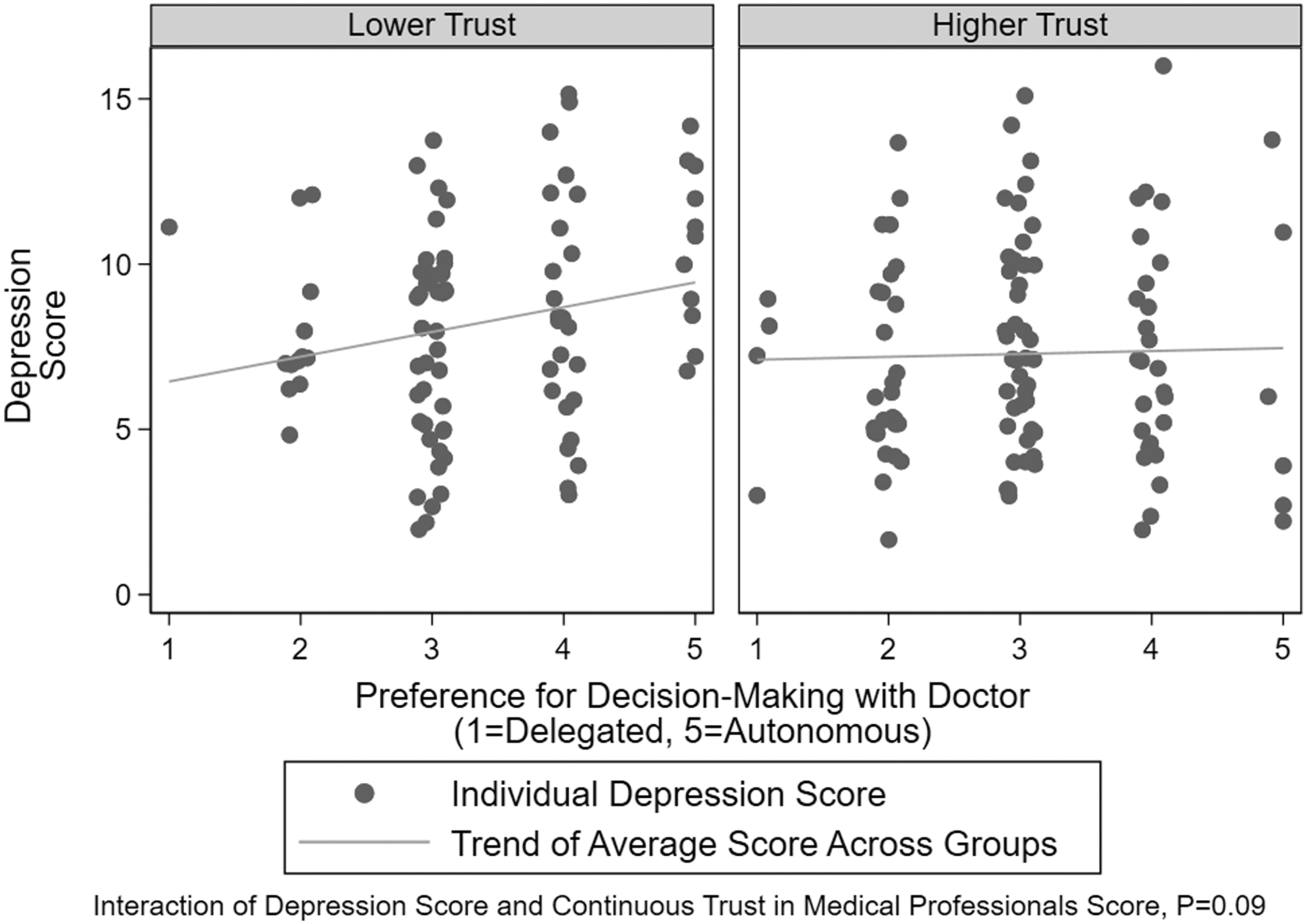
Association of Depression Score and Decision-Making Preference modified by level of Total Trust Score. Higher Depression Score indicates increased level of depression with 0–7 being a normal score, 8–10 being a borderline abnormal score, and 11–21 as an abnormal score.
Since previous studies have found that patient sex, race, age, private insurance status, and education level have been associated with scores on the Trust in Physician Scale, 44 we constructed a multivariable ordered logistic model containing these covariates for the parents and with decision-making preference as the outcome of interest and the total distrust score as the main prediction. None of these covariates were associated with the outcome (Supplementary Table S1), and the association of the Total Trust Score with the outcome slightly increased after adjustment for these covariates.
Discussion
We found that parents making a decision for their seriously ill child were more likely to prefer sharing a decision with their doctor, although a substantial minority endorse, or lean toward, the extremes of autonomous decision making and delegation to the doctor. A novel finding of our study was that parents who reported lower levels of trust in physicians were more likely to report a preference for autonomous decision making regarding the care of their child. Furthermore, we found that parents with low trust scores and higher levels of anxiety were more likely to express a preference for autonomy. Parents with higher levels of trust showed a greater preference for sharing decision making even if they had higher anxiety scores. These relationships did not change when we adjusted for sex, race, age, private insurance status, and parent education.
A similar relationship in adults between trust and patient preference for participation in decision making has been observed, finding that respondents who reported a preference for autonomy also had lower trust. 22 That study showed very few patients preferred autonomy and most of their respondents preferred shared or passive participation in decision making. Our current study is consistent with our previous findings showing that parents report a preference that their children's doctor and the parent share responsibility for the decision, while a sizable minority prefers to make the decisions themselves (autonomous) or mostly themselves 34.7%. 1
The Trust in Physician Scale has previously been used with parents of pediatric patients (Pedi-TiPs), 44 although mostly in an ambulatory care setting. Moseley et al. found associations between trust and demographic factors such as sex, older parent age, private insurance status, parent education greater than high school level, and not having a child age <3 years. They also found an association between lower trust and parents who identified as African American or “other” race, which has been seen in some other studies, although not all.21,45–48 We did not find these associations in our study, although our sample was predominately white and non-Hispanic.
Our finding that parents who exhibit low trust also report an increasing preference for autonomy as their anxiety scores increase has not been previously reported in the literature, to our knowledge. We know that parents of children with serious illness suffer a high incidence of anxiety.49,50 We also know that anxiety impairs decision-making capacity,33,34,51 which raises concerns if these parents prefer to make decisions autonomously. Trust is a fundamental part of the doctor–patient or doctor–parent relationship and is particularly important in the setting of serious illness 52 for patients and families. 24 A single event, such as receiving bad news delivered in an insensitive manner, or of feeling that one's concerns are being disregarded or dismissed by the care team, can cause parents profound distress 53 and increase anxiety, distrust, and dissatisfaction with care. 54 Furthermore, parents making decisions for their seriously ill children are particularly vulnerable to decisional regret. 13 In our study, we found that as the trust level goes up, parent preference for decision making trends toward shared and delegated, despite increasing anxiety scores. In other words, despite being anxious, parents with higher levels of trust preferred to interact with providers and participate in the sharing or delegating decision making and may be critical to lessen the burden of decision making and mitigate decisional regret. Some evidence suggests that factors used to engender trust in parents might be designed, studied, and translated into training programs.55–57
Those parents with high trust and greater depression may prefer less autonomy, as suggested in Figure 3, although this finding did not reach statistical significance. Long-term outcomes for parents after the death of a child are known to include depressive episodes, and other health problems are more likely to arise or be exacerbated in the presence preexisting depression. 58 Depression, trust, and decision-making preferences among parents may be an interesting area of future research and may help guide providers regarding when to be more proactive in the decision-making process.
These findings should be interpreted in light of both the strengths and limitations of this study. The strengths of our study included using a rigorous investigation with validated quantitative measures and assessments with a sample of parents of children with a diverse range of serious illness and conditions. The study was also grounded in well-established psychological theories of parental decision making and how anxiety may influence decision making,31–34,41 giving depth to our findings and interpretation of the novel empirical data regarding the relationships of trust, emotion, and decision-making preference. The study's limitations include data collection from a single hospital site where we enrolled only English-speaking parents. We did not find associations found in previous studies between race and trust, although this may be in part because the participants were predominately white and non-Hispanic. Also, the scales may be measuring independent variables. For example, the trust in physicians scale, because it asks questions regarding the perception of the trustworthiness of physicians as a profession rather than an individual may not correlate with the questions being asked on a decision-making preference scale. The associations described here do not imply causality, and further research is required to understand the relationships between these factors. More is needed to understand how trust in physicians and decision-making preference change over time and under different circumstances. Finally, we did not adjust for multiple statistical tests.
With these caveats kept in mind, three aspects of our findings warrant additional research with a longitudinal cohort: first, do some parents become distrustful because of negative experiences with providers or the medical system in general or do these parents start with a preference for autonomous decisions and low levels of trust of providers; second, does parental trust change over time and under what circumstances (e.g., does parent trust go down if a child continues to decline over time); and third, are there certain factors influencing trust that can be used as the basis for interventions to engender trust among patients and families and improve parent outcomes?
Conclusions
To the best of our knowledge, this is the first study in pediatrics to examine trust and decision-making preferences, and the first to look at how trust, anxiety, and depression might influence parent decision-making preferences. Parents who have lower levels of trust in physicians and report anxiety may prefer to make the medical decisions for their seriously ill child without help from physicians. Among parents with higher trust in physicians, anxiety was associated with greater preference for shared and delegated decision making. Clinicians may need to adopt strategies to respect the decision-making preferences of these parents without increasing their distrust and provide additional mental health support to parents who are anxious.
Footnotes
Authors' Contributions
All authors read and approved the final article. V.N.M. participated in the design of the study, analyzed data, interpreted results, and drafted the initial article. D.L.H. revised the article and created the data set used for analyses. J.S. analyzed data and revised the article for key intellectual content. C.F. obtained funding, participated in the design of the study, analyzed data, interpreted results, and revised the article for key intellectual content.
Funding Information
This study was supported by the National Institutes of Health's National Institute of Nursing Research (Grant No. R01NR012026).
Author Disclosure Statement
The authors have no financial relationships or conflicts of interest relevant to this article to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.