
Abstract
Abstract
Advance care planning (ACP) improves end-of-life care for patients and their caregivers. However, only one-third of adults have participated in ACP and rates are substantially lower among African Americans than among whites. Importantly, ACP improves many domains of care where there are racial disparities in outcomes, including receipt of goal-concordant care, hospice use, and provider communication. Yet, few studies have examined the effectiveness of ACP interventions among African Americans. The objectives of reducing disparities in the quality of palliative care for older African Americans through improved advance care planning (EQUAL ACP) are as follows: to compare the effectiveness of two interventions in (1) increasing ACP among African Americans and whites and (2) reducing racial disparities in both ACP and end-of-life care; and to examine whether racial concordance of the interventionist and patient is associated with ACP. EQUAL ACP
Introduction
Although all seriously ill patients are at risk for poor quality care, the risk is even greater among African Americans.1-3 In the last months of life, compared to whites, African Americans more commonly experience high-cost, low-quality care characterized by untreated pain, avoidable hospitalizations, poor communication with providers, receipt of care inconsistent with their preferences, and lower rates of hospice enrollment.1-3 These disparities are likely to worsen with the growing population of older adults. Between 2015 and 2030, the number of adults who are 65 years of age and older is expected to increase from 50 million to over 70 million.4,5 While the proportion of non-Hispanic whites will increase by 59%, the proportion of older African Americans (largest minority group of older adults) will increase by 115%.1,5 Because older African Americans have worse self-reported health, more disability, and higher rates of serious life-limiting illness, targeted approaches are needed to improve the quality of care for this vulnerable population.6-8
Advance care planning (ACP) improves many domains of care where there are racial disparities in outcomes, including receipt of goal-concordant care, provider communication, family satisfaction, preventable hospitalization, and hospice use.7,9 Among caregivers of patients who die, ACP is also associated with less depression and anxiety. Despite the benefits of ACP and the beliefs among the vast majority of Americans, including African Americans, that ACP is important, as few as 30% of adults have participated in ACP.7,9 Rates of ACP are substantially lower among African Americans than whites across age groups.1,3,7,10 Currently, we do not know the extent to which these differences reflect fixed cultural or individual values or modifiable community-based, provider, and health system factors.
Although a large body of research has examined factors that may explain lower rates of ACP among African Americans,7,10-12 few studies have examined the effectiveness of interventions to promote ACP for this group. Current research is limited by small samples that focus on a single disease population and include short-term follow-up. To date, no large studies have compared the effectiveness of two or more widely used or evidence-based interventions to facilitate equitable ACP and improve care for seriously ill African Americans and their caregivers.9,13,14
ACP, among African Americans, is influenced by a complex interaction of historical, personal, interpersonal, and system factors, including sociodemographics, mistrust in the health care system, access to care, religion and spirituality, family, community, and clinician interactions.10,15 Based on these factors, the current opportunities to improve ACP for African Americans using existing interventions include the following: (1) adopting a broader view of ACP with less emphasis on legal directives; (2) ensuring equal access to ACP interventions; (3) use of interventions that increase ACP knowledge and consider health literacy; (4) creating trusting relationships with peers; (5) and addressing clinician barriers to ACP through the use of processes that do not rely on them to initiate ACP. With this framework, we developed the study, Reducing Disparities in the Quality of Palliative Care for Older African Americans through Improved Advance Care Planning (EQUAL ACP). This article describes the study protocol for EQUAL ACP, a comparative effectiveness trial of two ACP interventions among seriously ill, older African Americans and whites.
Materials and Methods
Study overview
The overall goal of EQUAL ACP is to compare the effectiveness of two different ACP interventions in increasing ACP and promoting equitable palliative care outcomes among seriously ill, older African Americans and whites. EQUAL ACP includes a longitudinal, multisite, matched pair (patient and surrogate decision maker), cluster randomized trial and a qualitative study (semistructured interviews and analysis of ACP conversations) to describe the ACP experience of participants. The study will include 800 older adults residing in 5 states.
This study protocol was reviewed and approved by Institutional Review Boards (IRBs) across study sites, including Duke University Health System IRB (Pro00091633), which serves as central IRB for University of Alabama at Birmingham and two federally qualified health centers in South Carolina; Emory University IRB (IRB00103144); and University of Texas Southwestern (STU 052018-047). Study participants receive $50 for each data collection survey (four time points—total of $200), qualitative interview (random sample), or after-death interview (surrogates of patients who die during study).
Objectives and hypotheses
The primary aims of EQUAL ACP are to compare the effectiveness of a structured ACP approach to a patient-guided, self-management approach in the following: (1) facilitating ACP among older adults within each racial subgroup (African American and whites) and (2) reducing disparities in ACP between racial subgroups. Our secondary aims are to (1) determine if racial concordance of patient and lay ACP facilitator is associated with the effectiveness of the intervention in promoting ACP; and (2) among decedents, compare the effectiveness of the two ACP interventions in reducing racial disparities in receipt of care consistent with patient preferences, caregiver distress, satisfaction with care, and health care utilization in the last six months of life. The aim of the qualitative component is to describe racial differences in the experience of ACP, including beliefs, values, and goals, which may inform approaches to ACP.
EQUAL ACP will test the following hypotheses: (1) compared to a patient-guided, self-management approach, a structured ACP approach will result in the following: (a) higher rates of ACP among study participants within each racial subgroup and (b) smaller differences in rates of ACP between racial subgroups; and among decedents, smaller racial differences between subgroups in patient and caregiver outcomes. (2) Study participants in both racial subgroups who receive either ACP intervention from a lay ACP facilitator of the same race (vs. of a different race) will have higher rates of ACP.
Setting
We will enroll patients receiving care in 10 clinics in 5 states (2 clinics in each state), including Alabama, Georgia, North Carolina, Texas, and South Carolina. These sites are in the Deep South, an area where more than one-third of African Americans reside and where disparities in health outcomes are most pronounced.5,16 With the exception of the two federally funded health centers in South Carolina, all clinics are affiliated with an academic medical center. All the clinics are primary care practices and one is a geriatric medicine practice.
Population
Table 1 includes eligibility criteria of participants. The criteria capture older adults with serious illness defined as those at high risk of mortality, functional decline, or hospitalization. 17 Patients are eligible if they are English speaking, community dwelling, ≥65years of age, non-Hispanic, and white or African American and have a serious illness (advanced cancer, renal, liver, lung, or heart disease), and two or more unplanned hospitalizations in the last year; and ≥80 years of age along with dependence in one or more activities of daily living. Providers may refer patients to the study regardless of diagnosis if they “would not be surprised if patient died in the next 12 months.”18,19 Although the surprise questions are a poor screening tool for mortality in a primary care population, it has been significantly associated with one-year mortality over and above age, gender, and comorbidities when used by primary care physicians to identify patients at high risk of death. 19 We added the surprise question to our eligibility criteria to allow providers to refer patients to the study, who may not be identified by our electronic medical record (EMR) screening, but whom they believe are at high risk of death. Patients are excluded if they have an ACP (documented in EMR or reported by patient), reside in an institution, or would not be able to take part in the study protocol because of significant sensory or cognitive impairment. 20
Reducing Disparities in the Quality of Palliative Care for Older African Americans through Improved Advance Care Planning Eligibility Criteria
Assessed by telephone screen as score greater than two on six-item cognitive screener. 20
ACP, advance care planning; EMR, electronic medical record.
Enrolled patients are asked to identify one person who would help to make medical decisions for them if they become unable to make their own decisions. This may or may not be a person who also serves as a caregiver, assisting them with day-to-day care. Caregivers or surrogate decision makers who are named by the patient undergo telephone screening and are eligible to participate if they are ≥18 years of age and cognitively able to participate. Patients who do not identify a surrogate or caregiver or whose surrogates decline participation will still be allowed to participate.
Recruitment
Figure 1 includes the EQUAL ACP study flow. Potentially eligible patients with an upcoming appointment (three to four weeks out) at a participating clinic are identified by administrative data pull. Study personnel at each site screen EMRs to assess eligibility, and potentially eligible patients are mailed a letter from their primary care provider introducing the study. Patients who do not opt out of further contact by returning a post card or calling study office undergo telephone screening. Patients who are eligible and interested in participating complete informed consent. Once enrolled, patients provide name and contact information of a surrogate decision maker who is contacted by phone to complete eligibility screening and informed consent if he or she is interested in participating.
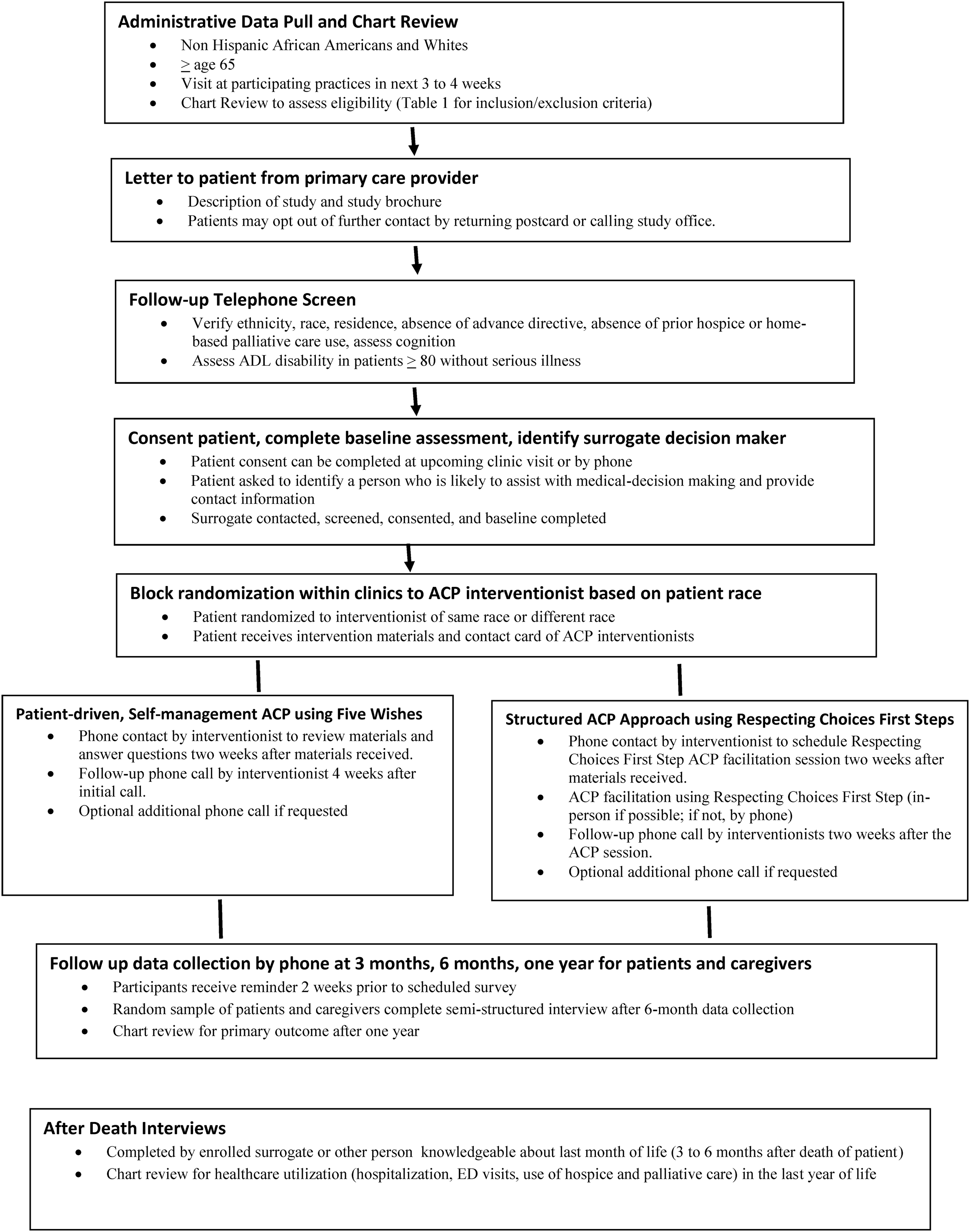
EQUAL ACP study flow. EQUAL ACP, reducing disparities in the quality of palliative care for older African Americans through improved advance care planning.
Intervention
Based on input of our stakeholders, we identified two ACP approaches for comparison: (1) a structured ACP approach using Respecting Choices First Steps and (2) a patient-driven, self-management approach, including a Five Wishes form. Both approaches are delivered by lay ACP facilitators. In addition to the materials and intervention described below, all participants receive state advance directive forms and a contact card with telephone number and picture of their assigned lay ACP facilitator.
Respecting Choices is an ACP program that has been implemented worldwide. Studies of Respecting Choices have shown an increase in the prevalence of advance directives, greater patient-surrogate congruence for treatment preferences, receipt of goal-concordant care, and decrease in health care utilization.21-24 A recent systematic review of Respecting Choices and related models noted limitations in research methods and inconsistency in findings related to ACP outcomes across published studies. 25 In addition, evidence on its use and outcomes in minority populations is limited.21,22 The Respecting Choices model includes three stages of ACP, First Steps, Next Steps, and Last Steps. First Steps is intended for those who have not planned. Next Steps involves ACP for those with advanced illness, and Last Steps involves expressing preferences as medical orders through the POLST paradigm. Although we are enrolling older adults with serious illness, we believe that First Steps is appropriate because (1) our study will include older adults who have not previously participated in ACP. First Steps is intended for those who have not planned. (2) A focus on specific treatments (Last Steps), rather than ACP as a process for sharing wishes for care in any way you choose, may not be consistent with values of some African Americans. 7 (3) ACP is not a one-time event. The goal of the intervention is to start to engage patients in ACP. Participants are encouraged to discuss their wishes with their providers who can focus more specifically on their disease, prognosis, and potential treatment options. Our intervention is one way to start to engage patients in ACP. (4) To ensure wide dissemination and rapid implementation of our findings, we are using lay facilitators who may have limited knowledge of specific disease processes.
Participants receive Respecting Choices materials that include general information about ACP and choosing a health care agent. Within two weeks, the patient is contacted by a lay ACP facilitator who sets up a time to meet with patient and surrogate decision maker for a 60-90-minute ACP session. The conversation focuses on identifying cultural, spiritual, and personal beliefs that influence treatment preferences, identifying a health care agent, and exploring goals for medical care. These meetings occur in person if possible (by phone if not). The lay ACP facilitator follows up with a phone call two weeks after the meeting to answer questions. Patients may request one additional follow-up call (Fig. 1).
Patients at clinics randomized to the patient-driven, self-management ACP approach receive the Five Wishes advance directive form and the Five Wishes Conversation Guide for Individuals and Families. Although Five Wishes has not been systematically studied, it is the most widely used advance directive in America with over 25 million copies distributed by 40,000 organizations. 26 Five Wishes is both a decision aid and an advance directive written in nontechnical language. The document allows patients to share their “wishes” for the following: the person they would like to serve as surrogate decision maker; the kind of medical care that they would like to receive; how comfortable they want to be; how they want people to treat them; and what they want their loved ones to know. Five Wishes is a legal directive in three of the five states (North Carolina, South Carolina, and Alabama) from which we will recruit patients, and can be used along with state directive forms in the other states. 26 Two weeks after participants receive the Five Wishes materials, a lay ACP facilitator contacts them by phone to review the materials and answer questions using a scripted protocol that we developed. The lay facilitator follows up four weeks later to answer questions and is available for an optional third call if requested (Fig. 1).
Randomization
EQUAL ACP is a cluster randomized trial, with randomization occurring at both the clinic (i.e., the cluster) and the patient level (Fig. 2). The two clinics in each state were randomly assigned to either the patient-driven self-management or the structured ACP approach through a blocked randomization scheme, with site as the block. We will enroll 40 African American and 40 white patients from each of the 10 clinics, for a total of 800 patients, half in each racial group. Within each clinic and racial group, patients are randomized in a 1:1 ratio to have the intervention delivered by either a racially discordant or concordant lay ACP facilitator. Thus, half of the patients in each racial group (200 in total) will receive the intervention from an ACP facilitator of their race and half from an ACP facilitator of a different race. Clinic-level and patient-level randomization schemes were developed in PROCPLAN (SAS v 9.4).
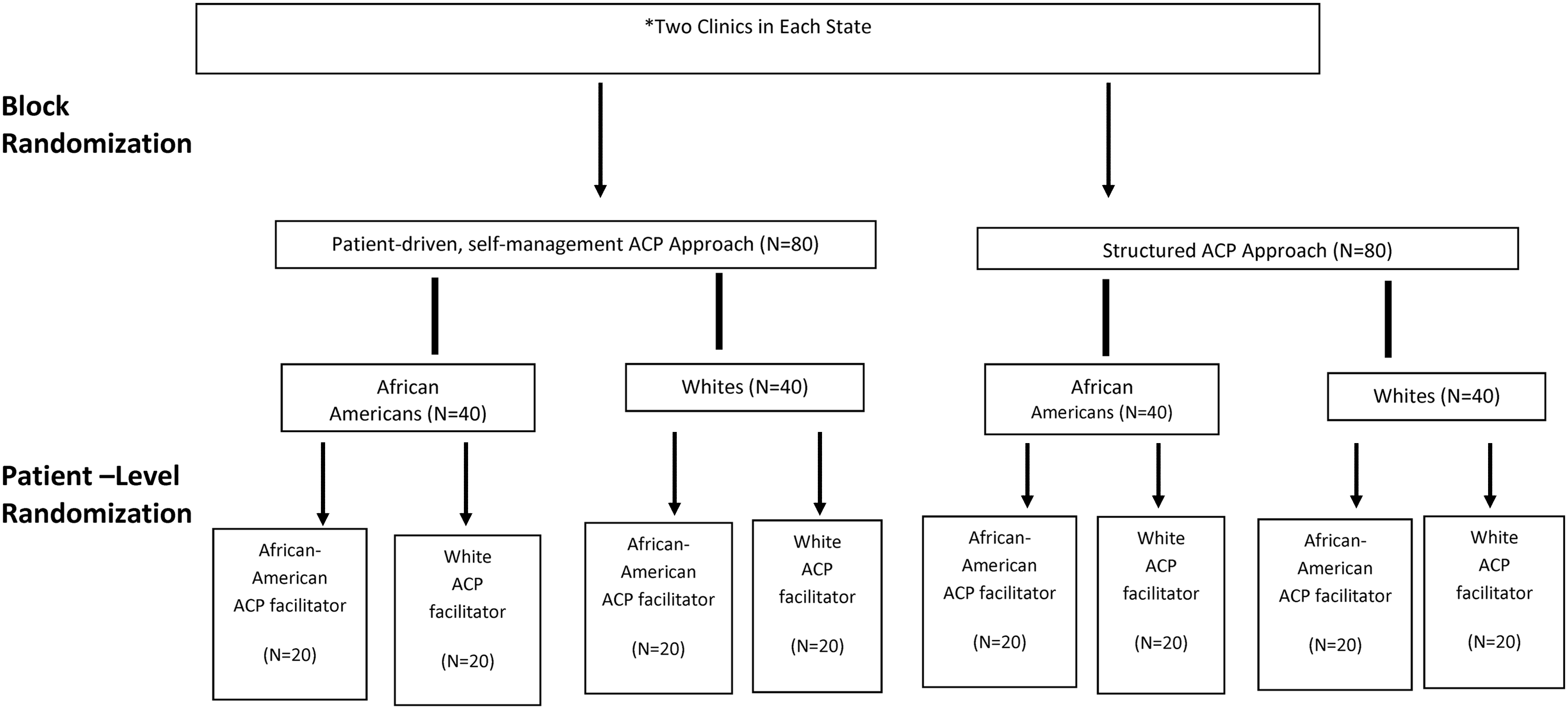
EQUAL ACP randomization scheme. There are a total of 10 clinics, 2 in each of 5 states. This figure shows randomization recruitment and for two clinics in one state. The two clinics in each state were randomly assigned to either the patient-driven self-management or the structured ACP approach through a blocked randomization scheme. We will enroll 40 African American and 40 white patients from each clinic for a total of 800 patients, half in each racial group. Within each clinic and racial group, patients are randomized in a 1:1 ratio to have the intervention delivered by either a racially discordant or concordant lay ACP facilitator. Thus, half of the patients in each racial group will receive the intervention from an ACP facilitator of their race and half from an ACP facilitator of a different race. ACP, advance care planning.
Outcome measures
Study measures are detailed in Table 2. The primary outcome for EQUAL ACP is formal or informal ACP one year after the intervention. Based on discussions with stakeholders (discussed in more detail in Patient and Key Stakeholder Engagement section), we adopted a broad definition of ACP. We defined ACP as any of the following: (1) completion of a formal document (HCPOA, living will, Five Wishes, POLST, or other legal directive) or an informal document (i.e., letter) naming a decision maker or describing preferences; (2) discussion with clinician documented in chart; and (3) patient report that he/she asked someone to make decisions for him/her or discussed values, goals, or preferences for future medical care with family, friends, or other surrogate decision-makers. We believe that this broad definition is the most patient-centered approach because it accounts for the fact that patients vary in how and with whom they choose to express their preferences for care. This is especially relevant for African Americans who are more likely to discuss their preferences with others than to complete advance directives. 7
Reducing Disparities in the Quality of Palliative Care for Older African Americans through Improved Advance Care Planning Study Measures
Surrogate answers based on his/her beliefs about patient experiences or preferences.
Our secondary outcomes are proximal, intermediate, and distal measures of the effectiveness of the ACP process. These include readiness to engage in ACP, beliefs about ACP, congruence between patients and surrogate decision makers regarding patients' preferences, and surrogates' comfort with end-of-life decision-making for patient. For patients who die during the study period, we will collect information on health care utilization (acute care use and palliative care use) during the last six months of life, and surrogates' satisfaction with end-of-life care and surrogate mental health outcomes.
In addition to our outcome measures, we included a number of measures to assess patient and caregiver factors that may both influence ACP and differ by racial groups. These include demographics, function, health literacy, trust in providers and the health care system, religiosity/spirituality, and perceived barriers to ACP.
Data collection
Our outcome measures will be assessed at baseline, three months, six months, and one year (Table 2). For patients who die, we will interview an enrolled surrogate or next-of-kin three to six months after patient's death. We developed a centralized tool for capturing data across study sites electronically using a custom participant tracking application and REDCap. 27 Trained clinical trial coordinators at each site collect and enter data into REDCap in real time. The tracking application and REDCap projects are housed on a secure database server at Duke with access limited to key personnel. Throughout enrollment and data collection, we will monitor data quality, accuracy, and timeliness.
Qualitative data collection
We will describe racial differences in the experience of the ACP process using qualitative analysis of a random sample of recordings of ACP conversations between patients and interventionists and interviews with participants from clinics in both arms of the study. The interviews will be completed after the six-month data collection using a semistructured interview guide to facilitate a thick description of the ACP experience in participants' own words, including barriers and facilitators to ACP; role of trust, spirituality, and family; and an evaluation of the interventions to identify the most and least helpful elements as well as additional components, which may be important to participants. We expect our final sample will include analyses of ∼50 African Americans and 50 whites (patients and caregivers) for each data collection method (ACP conversations and interviews) with purposive sampling based on sociodemographic factors, study site, and racial concordance between patient and ACP facilitator. All recordings will be transcribed and entered into Atlas.ti for data management. 28 We will analyze the data using techniques of directed content analysis, organizing the data, and identifying common themes in response to the a priori questions contained in the interview guide. 29
Analysis
The first three study aims involve analyses of the primary binary outcome (the presence or absence of formal/informal ACP one year after the intervention) with different groups of patients and comparisons. We will fit two separate generalized linear mixed models, one for African Americans (n = 400) and one for whites (n = 400). Each model will have an indicator variable for the structured ACP approach versus the patient-driven, self-management approach, and a clinic-level random effect to capture the intraclass correlation. We will use a single generalized linear mixed model to compare the effectiveness of the two ACP approaches in reducing racial disparities in ACP. This model will have an indicator variable for intervention group, a clinic-level random effect, and an indicator variable for race and the interaction between intervention group and race.
To examine the impact of racial concordance of the ACP facilitator on ACP, we will use generalized linear mixed models within four different subgroups (African Americans and whites within each of the two intervention groups). Each model will include an indicator variable for racially concordant versus discordant ACP facilitator and a clinic-level random effect. Finally, we will assess patient and caregiver outcomes for the subsample of patients who die during the study period with models that include an indicator variable for intervention group, a clinic-level random effect, an indicator variable for race, and the interaction between intervention group and race.
Sample size and power considerations
Our primary hypothesis is that, within each racial subgroup, a structured ACP approach will result in higher rates of ACP by one year than the patient-guided, self-management approach. Based on prior research, we assumed a rate of formal/informal ACP in the patient-driven, self-management ACP group ranging from a low of 20% to a high of 40%. Calculations assumed a type-I error of 5% and were completed using tests for two proportions in a cluster randomized design to account for intracluster correlations ranging from 0.01 to 0.02. 30 As described above, ACP will be ascertained from both self-report and by chart review over the one-year study period; therefore, we anticipate complete data on this outcome for all study participants. For each racial subgroup of 400 patients, we will have 80% power to detect minimum differences of 14.5%-18.4% in rates of ACP between the two ACP approaches. To examine racial disparities between the two ACP approaches, the effective sample size of this comparison is one-quarter the overall sample size. Assuming racial disparities in ACP rates ranging from 10% to 30%, we will have 80% power to detect differences in reduced disparities of 9%-18% between the two ACP approaches. Finally, for our continuous caregiver outcomes among decedents (e.g., satisfaction with end-of-life care), calculations were completed using tests for two means in a cluster randomized design; we will have 80% power to detect differences in effect sizes of 0.4-0.50 in racial disparities between the two ACP approaches.
Fidelity Monitoring
Our interventionists are lay ACP facilitators with no prior formal training. We developed a multipronged approach to monitor intervention fidelity. First, all interventionists completed standardized training. The lay ACP facilitators for Respecting Choices First Steps completed the corresponding ACP Facilitator Certification course. ACP facilitators working with participants from clinics in the other study arm completed training in using the scripted protocol that we developed for reviewing the Five Wishes materials and answering questions. Interventionists in both arms completed training in motivational interviewing, general principles of ACP, and completion of advance directive forms. Total in-person instruction ranged from 12 to 14 hours.
Second, during the four to six weeks after the in-person training, ACP facilitators practiced delivering the intervention with research staff at each local site, who had also completed training. After a series of practice sessions, the ACP facilitators were required to deliver the full intervention to a patient or stakeholder and demonstrate successful mastery (80%) of competencies relevant to their training.
Third, interventionists in each arm participate in separate monthly group calls where they share experiences delivering the intervention and receive feedback from research staff and instructors. Finally, ACP facilitators will record a random sample of their interventions throughout the course of the study. These will be reviewed using prespecified criteria to assess adherence to the study protocol and provide individual feedback.
Patient and Key Stakeholder Engagement
Our stakeholder engagement strategy ensures we solicit diverse perspectives from each of the study sites to inform and guide the study. EQUAL ACP has six local Stakeholder Advisory Councils (SACs)—four of them linked to the participating academic institutions and one for each of the South Carolina federally qualified health centers—and a central Stakeholder Advisory Board (SAB). Each SAC and the central SAB consist of 8-10 members, including African American and white patients and caregivers, clinicians, clergy, community educators, and health system leaders. The SAB includes representatives from national- and community-based organizations that aim to promote equitable care. All stakeholders participated in a one-hour webinar, Research 101, which provides information about the research process and stakeholder engagement.
To facilitate bidirectional communication and consistency across sites, we created standardized processes for engagement. SAC and SAB meetings (90 minutes) occur quarterly (in person and Webex) at each site and are facilitated by a member of the local research team. The research team develops a common agenda for all meetings and facilitators participate in a premeeting session to discuss the agenda. SAC facilitators record recommendations and input on a standardized form. These data are compiled and presented at the SAB meetings. Recommendations from the SAB are shared with full research team and local SAC members. During and between meetings, stakeholders offer input on study design, participant recruitment, interventionist training, measures, study materials, and dissemination of information about the study.
Potential Barriers to Study Success
The primary challenges to study success are participant attrition, loss of interventionists, maintenance of intervention fidelity (see Fidelity Monitoring section), and coordination of data collection. To reduce attrition, we will review the electronic medical record regularly to update contact information for participants, mail reminders to participants two weeks before data collection, and provide participants with a $50 incentive for each completed assessment. To address possible loss of interventionists, we will maintain at least four interventionists per site (two from each racial group) with training in Respecting Choices First Steps, and six interventionists (three from each racial group) who are trained in the patient-driven, self-management ACP protocol that can be delivered by telephone to patients across sites. To ensure the timely training of new interventionists, we have access to instructors for both study arms. To address potential issues with data management, we have developed standardized processes for data collection, organization, and storage, training of research personnel, and troubleshooting information technology issues locally and centrally by the EQUAL ACP Operations Team at Duke.
Dissemination
For the academic community, we will present our finding at scientific meetings and in peer-reviewed journals. Our stakeholders will assist us with implementing dissemination strategies that target their realms of influence, including health care organization and community groups. We will work with stakeholders to develop information that can be adapted for diverse audiences, with particular emphasis on cultural tailoring of information for African Americans and those with low literacy. Our efforts will be augmented by partnerships with local community engagement groups (e.g., CTSA), with established networks for widespread dissemination of information across diverse platforms. Based on our findings, our stakeholders will assist us with identifying next steps, which may include refinement of interventions, replication of study in other settings, or widespread dissemination in local health systems.
Discussion
ACP may significantly reduce racial disparities in the quality of end-of-life care. To our knowledge, EQUAL ACP is the first large, multisite study to compare the effectiveness of two evidence-based and/or widely used interventions to facilitate ACP and improve end-of-life care for older African Americans. The EQUAL ACP protocol was developed based on an extensive review of the literature and stakeholder input to identify historical, interpersonal, community, and system factors that may influence ACP. Although EQUAL ACP cannot address all of these factors, we identified several opportunities to improve ACP for African Americans within the context of existing interventions, including (1) a greater emphasis on the importance of ACP conversations with surrogates and providers even if patients do not complete legal documents; (2) flexibility in approaches to ACP based on individual preferences; (3) and the use of peer-to-peer interactions with lay ACP interventionists to build trust, increase ACP knowledge, and facilitate ACP. In addition, our protocol includes a qualitative component to describe the ACP experience of participants, identify gaps in existing interventions, and elucidate additional strategies or elements that assist with ACP. This information may be used in future studies to ensure that interventions address the range of factors important to African Americans. The findings of EQUAL ACP will inform efforts to develop and implement evidence-based palliative care interventions that promote equitable palliative care outcomes for older, seriously ill African Americans and their caregivers.
Footnotes
Acknowledgment
Funding: This study is funded by the Patient-Centered Outcomes Research Institute (Contract R-1609-36381).
Author Disclosure Statement
No competing financial interests exist.