
Abstract
Abstract
Background:
Toileting independence is considered to be important factors for achieving a “good death” for terminally ill patients.
Aim:
To clarify the period from loss of the ability to access toilets independently to death in end-stage cancer patients.
Design:
Observational study.
Setting/Participants:
The medical records of all end-stage cancer patients who had died while using home care services provided by Medical Corporation Kagayaki General Home Care Clinic between September 2011 and August 2017, were retrospectively reviewed.
Results:
A total of 220 patients were included. The median time from total dependence in toileting to death was 6.0 (95% confidence interval: 5.0–7.0) days. When the duration was 7 days or shorter and 21 days or shorter, the cumulative death rate was 55.9% and 86.4% respectively.
Conclusion:
A large percentage of terminally ill cancer patients maintained the ability to access toilets independently until very close to the end of their lives, so the duration of total assistance needed was shorter. These findings may be useful to make a care plan to support achieving “good death” for patients.
Introduction
Toileting independence is a fundamental activity of daily living (ADL), which maintains patients' dignity.1,2 In fact, loss of abilities necessary for personal hygiene, walking, and transfer as basic ADL decrease the quality of life,2,3 and require advanced caregiving skills. 4 Families' insufficient caregiving skills may lead to the necessity of hospitalization.5,6
Preventing/reducing care dependency, loss of dignity, and heavy caregiving burdens are other important factors, which increase families' and patients' mental distress, and make achieving a good death difficult. Steinhauser, et al. elucidated the concept of a good death’, which includes “Affirmation of the Whole Person” as a subconcept. 7 In the fundamental care, it is emerged that failure to meet the toileting needs affected patients' dignity the most. 8 For Japanese people, the concept of “Not being a burden to others” contributed to a good death. 9 If any of the factors that contribute to a good death are missing, a good death may be difficult to achieve, and this could in turn lead patients to consider euthanasia or physician-assisted suicide (PAS). 10 In these respects, the prediction of survival after declines in ADL, loss of toileting independence, and the provision of related information may contribute to the maintenance of patients' dignity, reduction of caregiving burdens, and decision making regarding the continuation of home care.
Therefore, this study examined the period from loss of the ability to access toilets independently to death in end-stage cancer patients receiving home care, and additional aim was to explore predictors of death within a short period (1 week).
Methods
Subjects
The prospectively collected medical records of all cancer patients who had died using home care services provided by Medical Corporation Kagayaki General Home Care Clinic, primary care clinic with providing specialized palliative care in the community, between September 2011 and August 2017, were retrospectively reviewed. Among these, we included the patients who could access toilets independently on the initial referral and who continued to receive home care without being hospitalized until their death. On the other hand, we excluded those who were unable to excrete independently at the time of the initial home visit, who became bedridden at an unspecified time, and who died suddenly. We defined “Ability to toilet independently” as a sequence of actions: getting out of bed; moving to toilet; excreting; getting back to bed, independently without any support. Therefore, “loss of ability to toilet” implies that there was a problem in the sequence of actions.
ADL and survival calculation
The duration of total assistance, which was defined as the period from loss of the ability to access toilets independently until death, was individually investigated.
Study items
The study items were as follows: the age and gender; scores from the Eastern Cooperative Oncology Group (ECOG) Performance Status (PS), Palliative Prognostic Index (PPI), 11 and Prognosis in Palliative Care Study Predictor Models-A (PiPs-A) 12 ; the history of cerebrovascular/neurological disorder or spinal disease; the presence/absence of dyspnea, lower limb paralysis, delirium, loss of appetite, a 5% or more marked decrease in the body weight within one month, dysphagia, lower limb edema, pressure ulcers, and an established diagnosis of dementia; vital signs (systolic blood pressure, heart rate, respiratory rate, oxygen saturation level, and body temperature) on the day when it became difficult to access toilets independently; the necessity of oxygen inhalation, fluid therapy, urinary catheterization, and fecal disimpaction; presence/absence of hepatic, bone, or distant metastasis (excluding those to the liver/bone); duration of disease; opioid use; family structure (solitary/nonsolitary); and primary lesion.
Statistical analysis
A Kaplan–Meier curve was created based on the duration of total assistance and survival rates. In addition, the patients were divided into three groups based on their durations of total assistance: 7 days or shorter, 14 days or shorter, and 21 days or shorter, to calculate the proportion of each group.
Patients who died within one week and those who survived longer were divided into shorter and longer survival groups, respectively, to perform univariate analysis. Multiple logistic regression analysis was also performed using dyspnea, delirium, loss of appetite, and PS scores, which are considered as prognostic predictors for the PPI, 11 in addition to factors showing p < 0.2 in univariate analysis.
Data collected through the medical record review were descriptively and statistically summarized and quantified as mean ± standard deviations or medians and ranges (minimum-maximum values). For comparison among the groups, the t test, Mann–Whitney U test, chi-square test, or Fisher's exact test were used, according to the type of data. Multiple logistic regression analysis was based on the stepwise method for variable selection. The significance level was set at 0.05 in all cases. All these statistical procedures were performed using SPSS version 22 (IBM Japan Ltd., Tokyo).
Ethical considerations
The study was conducted with the approval of the Ethics Committee of General Home Care Clinic (approval number: 2017-01).
Results
Patients' backgrounds
Excluding those who were unable to excrete independently at the time of the initial home visit (90), those who became bedridden at an unspecified time (25), and those who suddenly died (5: bleeding from the tumor: 1, ruptured esophageal varix: 1, cardiac infarction: 1, cerebral hemorrhage: 1, and unknown cause: 1), 220 patients were included (Fig. 1). All patients used home care services. Table 1 outlines the patients' backgrounds when included.
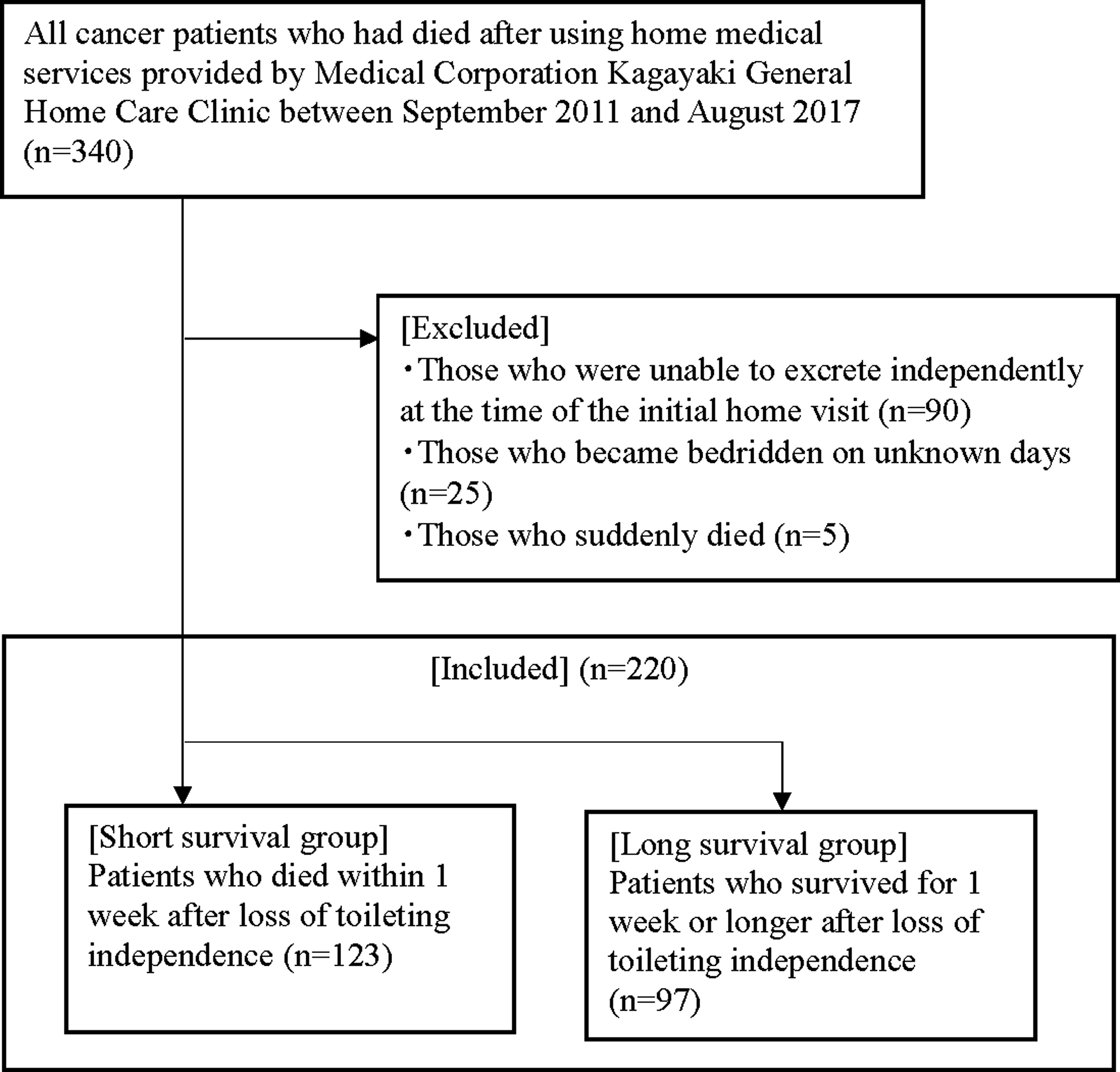
Subject inclusion flowchart.
Patients' Backgrounds When Included (When It Became Difficult to Access Toilets Independently)
ECOG; PiPs-A: Prognosis in Palliative care Study predictor models-A; SD, standard deviation.
Primary endpoint: ADL and expected survival times
The median duration of total assistance was 6.0 (95% confidence interval: 5.0–7.0) days (Fig. 2). The cumulative death rate for each duration of total assistance was as follows: 7 days or shorter: 55.9%, 14 days or shorter: 75.5%, and 21 days or shorter: 86.4% (Fig. 3).
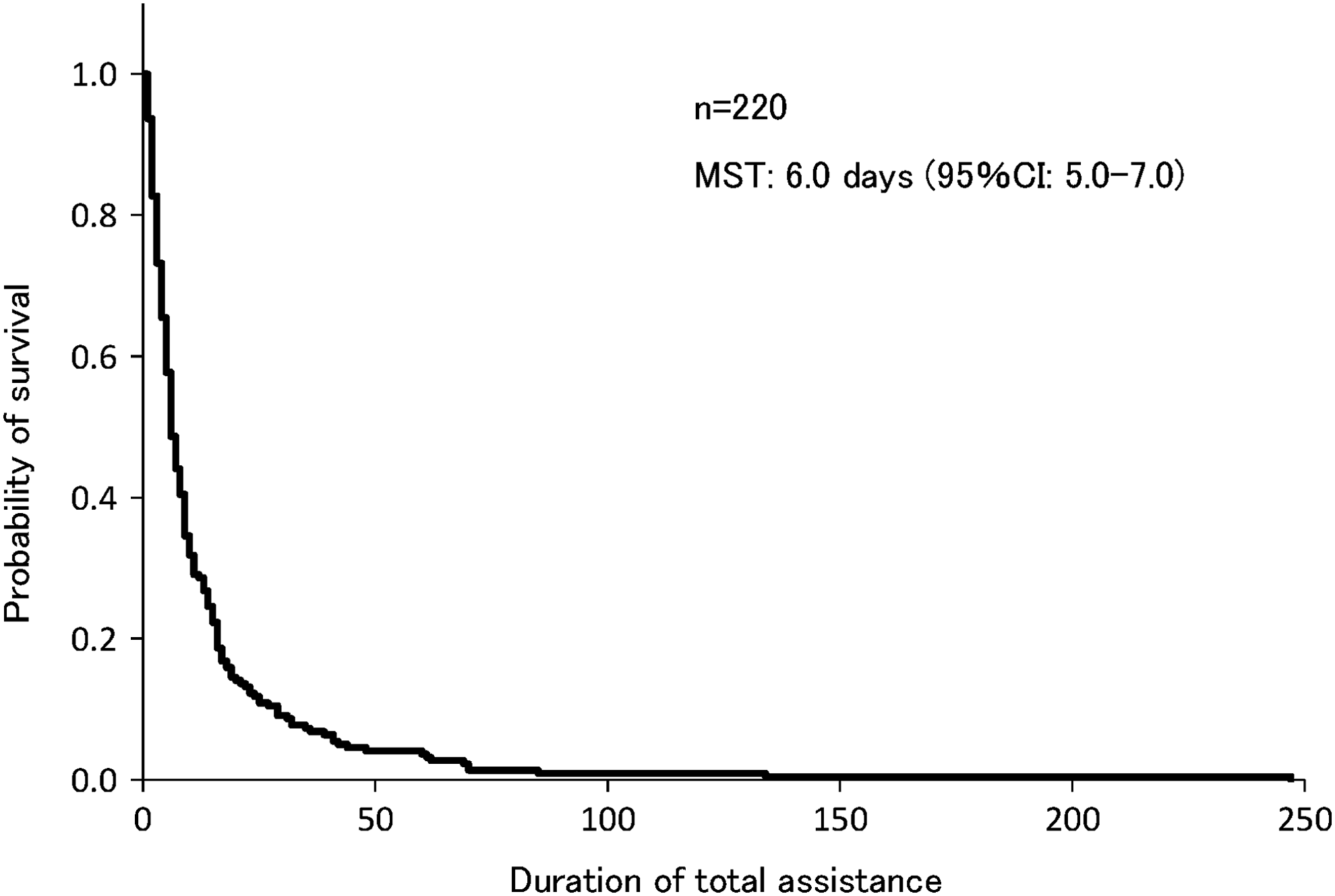
Expected survival times. The duration of total assistance was defined as a period from loss of toileting independence to death. CI, confidence interval; MST, median survival time.
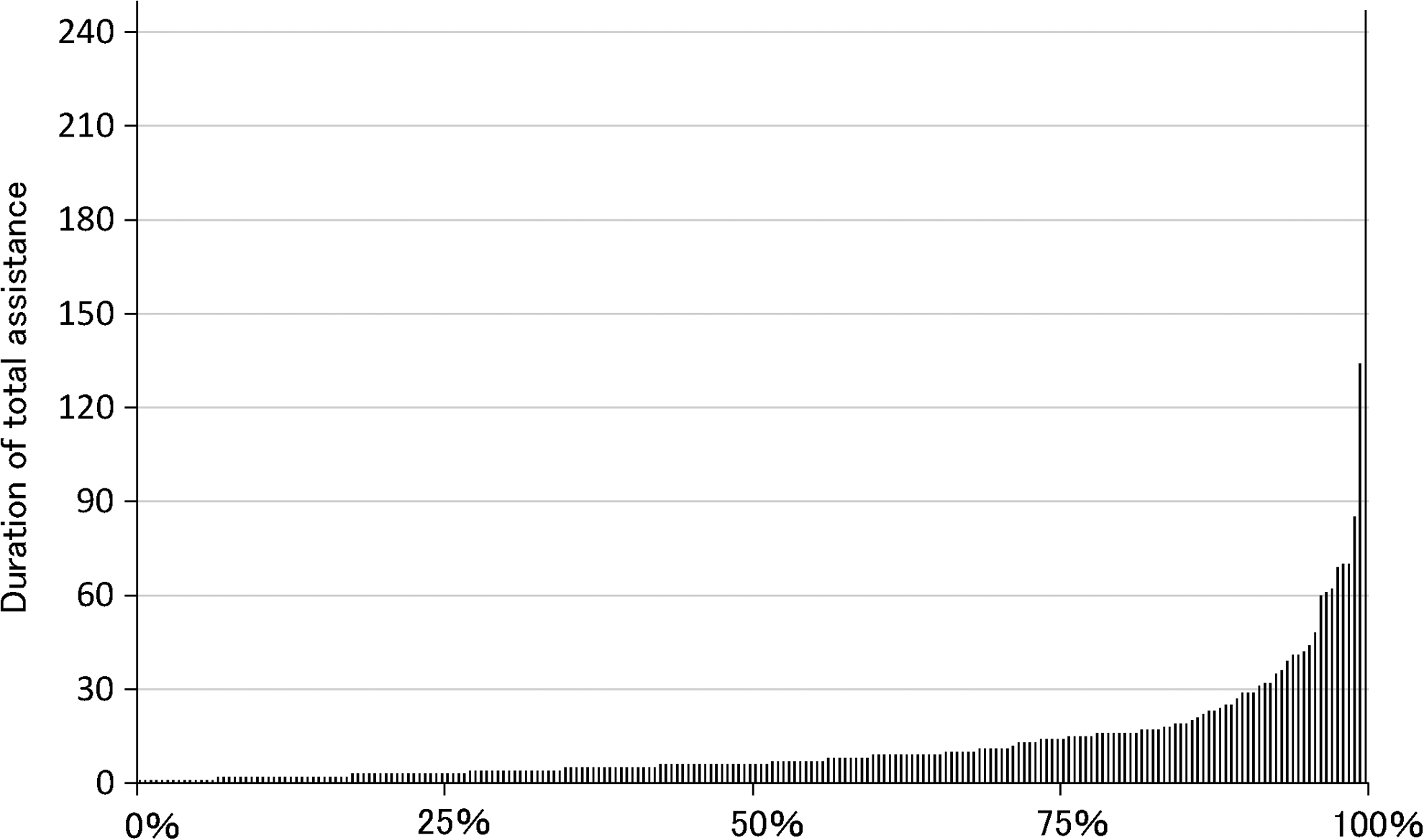
Duration of total assistance and its distribution. The longitudinal axis indicates the period from the initiation of total assistance (loss of toileting independence) to death (duration of total assistance). Each bar represents the duration of total assistance required for each patient. From the left to right, the length of the bar or the duration increases (n = 220). During the period of total assistance, 50%, 75%, and 90% of patients died within 6, 14, and 27 days, respectively.
Predictors of death within one week
In these cases, hepatic metastasis and loss of appetite increased the probability of death within one week. Positive factors for a one-week or longer survival were lower limb paralysis due to metastatic cancer, pressure ulcers, dementia, and distant metastasis, excluding those to the liver. Related significant differences, among dyspnea, an abnormal heart rate, and leukemia were not observed (Table 2).
Predictors of Death within One Week
Discussion
The results clarified the survival distribution of patients requiring total assistance. Notably, the present study demonstrated that the walking ability of cancer patients receiving home care is maintained to some extent until their last days, and the median period from loss of mobility until death is as short as six days. It is known that various vital reactions occur at the end of life, following a rapid loss of mobility due to declines in ADL.13,14 It is inevitable that the ability to access toilets independently gradually decreases. A prolonged period of the loss of mobility to access toilets independently could in turn lead to a loss of patients dignity and thus potentially increase the risk of euthanasia/PAS. 15 Additionally, when supporting home care users, excretion management is a common challenge, occasionally leading to the necessity of hospital admission in Japan. 6 However, the present study indicated that the duration of total assistance is actually short, and patients' and their families' care-related burdens may not be as heavy as previously considered. For the aforementioned reasons, loss of dignity, and the risk of euthanasia/PAS might be limited at least in cancer patients.
Another interesting finding was that hepatic metastasis and appetite loss increase the probability of death within one week. To date, prognostic predictors of death within a short period (1 week) have been examined only using biomarkers, 16 and the majority of such tools are designed to predict survival times longer than three weeks. 17 Our results suggested marked influences of metastasis to major organs and loss of the ability to orally ingest nutrients on the prognosis.18,19 As tools to predict the one-week prognosis based on specific clinical symptoms are unavailable at present, the factors shown to be associated with death within one week in the present study may prove important for patients' and families' decisions on continuing home care.
The study has some limitations: First, as this is a retrospective single-center study, the generalization of the results should be considered in future studies. However, the similarity between the curve of survival shown in Figure 1 and that representing the rate of losing mobility immediately before death 13 may support the conclusions. Second, it was difficult to clarify the exact moment when the patients' mobility was lost, and it only covered the patients who died. These may have led to the estimation of their survival times at slightly lower than actual values. Third, there may have been unmeasured, unknown confounders. Finally, the backgrounds of patients admitted to hospitals remained unclear, and hospitalization itself may have resulted in a selection bias.
Despite these limitations, this study may be useful to reduce patients' and their families' psychological burden regarding excretion care. The provision of these findings to patients and families may also prevent undesired, unplanned hospital admission and euthanasia/PAS, consequently allowing patients to die naturally in their homes, with their dignity maintained.
Conclusion
Nearly half of the home care cancer patients were able to access toilets and excrete independently until one week before death, revealing that the period from loss of such an ability until death is short. As these findings may support patients' and families' decision making, they should be re-examined in prospective studies and shared among healthcare professionals in end-of-life care.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.