
Abstract
Abstract
Background:
High-quality care for seriously ill patients aligns treatment with their goals and values. Failure to achieve “goal-concordant” care is a medical error that can harm patients and families. Because communication between clinicians and patients enables goal concordance and also affects the illness experience in its own right, healthcare systems should endeavor to measure communication and its outcomes as a quality assessment. Yet, little consensus exists on what should be measured and by which methods.
Objectives:
To propose measurement priorities for serious illness communication and its anticipated outcomes, including goal-concordant care.
Methods:
We completed a narrative review of the literature to identify links between serious illness communication, goal-concordant care, and other outcomes. We used this review to identify gaps and opportunities for quality measurement in serious illness communication.
Results:
Our conceptual model describes the relationship between communication, goal-concordant care, and other relevant outcomes. Implementation-ready measures to assess the quality of serious illness communication and care include (1) the timing and setting of serious illness communication, (2) patient experience of communication and care, and (3) caregiver bereavement surveys that include assessment of perceived goal concordance of care. Future measurement priorities include direct assessment of communication quality, prospective patient or family assessment of care concordance with goals, and assessment of the bereaved caregiver experience.
Conclusion:
Improving serious illness care necessitates ensuring that high-quality communication has occurred and measuring its impact. Measuring patient experience and receipt of goal-concordant care should be our highest priority. We have the tools to measure both.
Introduction
H
This article suggests a conceptual framework for the processes that contribute to goal-concordant care and that may assist in quality improvement, accountability schemes, or both. We identify quantifiable variables for these processes, review challenges and opportunities related to measuring them, and examine how they may be implemented.
Communication, Shared Decision Making, and Quality Measurement in Serious Illness
A serious illness carries a high risk of mortality AND either negatively impacts a person's daily function or quality of life, OR excessively burdens their caregivers. 2 Communication plays several roles in the experience of patients with serious illness. First, serious illness frequently requires complex decision making, which entails communication about the risks, benefits, and uncertainties of treatment. Second, serious illness may not only directly limit one's cognitive ability, but it also heightens anxiety for patients and families, 3 undermining critical thinking abilities. 4 Clinicians, therefore, must respond to emotion when attempting to convey understandable and actionable care options. Finally, treatment decisions typically involve the risk of hastened mortality or prolonged dying, which raise the stakes of communication.
National consensus bodies promote shared decision making (SDM) as the dominant model for communication in such settings.5,6 Experts define SDM as “an interpersonal, interdependent process in which the healthcare provider and the patient relate to and influence each other as they collaborate in making decisions about the patient's healthcare.” 7 Clinicians may influence patients by sharing medical knowledge and experience, and patients may influence clinicians by disclosing values and goals relevant to the application of that knowledge. This patient-centered process intends to support the receipt of goal-concordant care.
Existing national quality frameworks for seriously ill patients inadequately capture this outcome or the communication processes and qualities that likely facilitate it. National Quality Forum-endorsed process measures encourage the documentation of treatment preferences or “care plans,” activities that presuppose, but fail to guarantee, that high-quality communication has taken place (Table 1). Most existing quality measures refer implicitly or explicitly to life-sustaining treatments alone. Several assess the utilization of hospice or of potentially nonbeneficial treatments near the end of life (EOL).
Quality reporting program.
Physician quality reporting system.
This measure is also included in NCP domain 7.2
BFS, bereaved family survey; HHCAHPS, Home Health Consumer Assessment of Healthcare Providers and Systems; ICU, intensive care unit; IDT, interdisciplinary team; PQRS, physician quality reporting system; QRP, quality reporting program; VA, Department of Veterans Affairs.
Recognizing these shortcomings, several national organizations promote goal-concordant care as a quality indicator for seriously ill patients.8–10 Yet, measuring goal-concordant care directly poses formidable methodological challenges, including documentation of nonspecific or potentially irrelevant treatment preferences, poor documentation of those preferences, instability of preferences over time, and challenges related to determining “agreement” between preferences and outcomes. 11 Because of these challenges, healthcare systems may consider measuring indicators that either predict goal concordance or result from it.
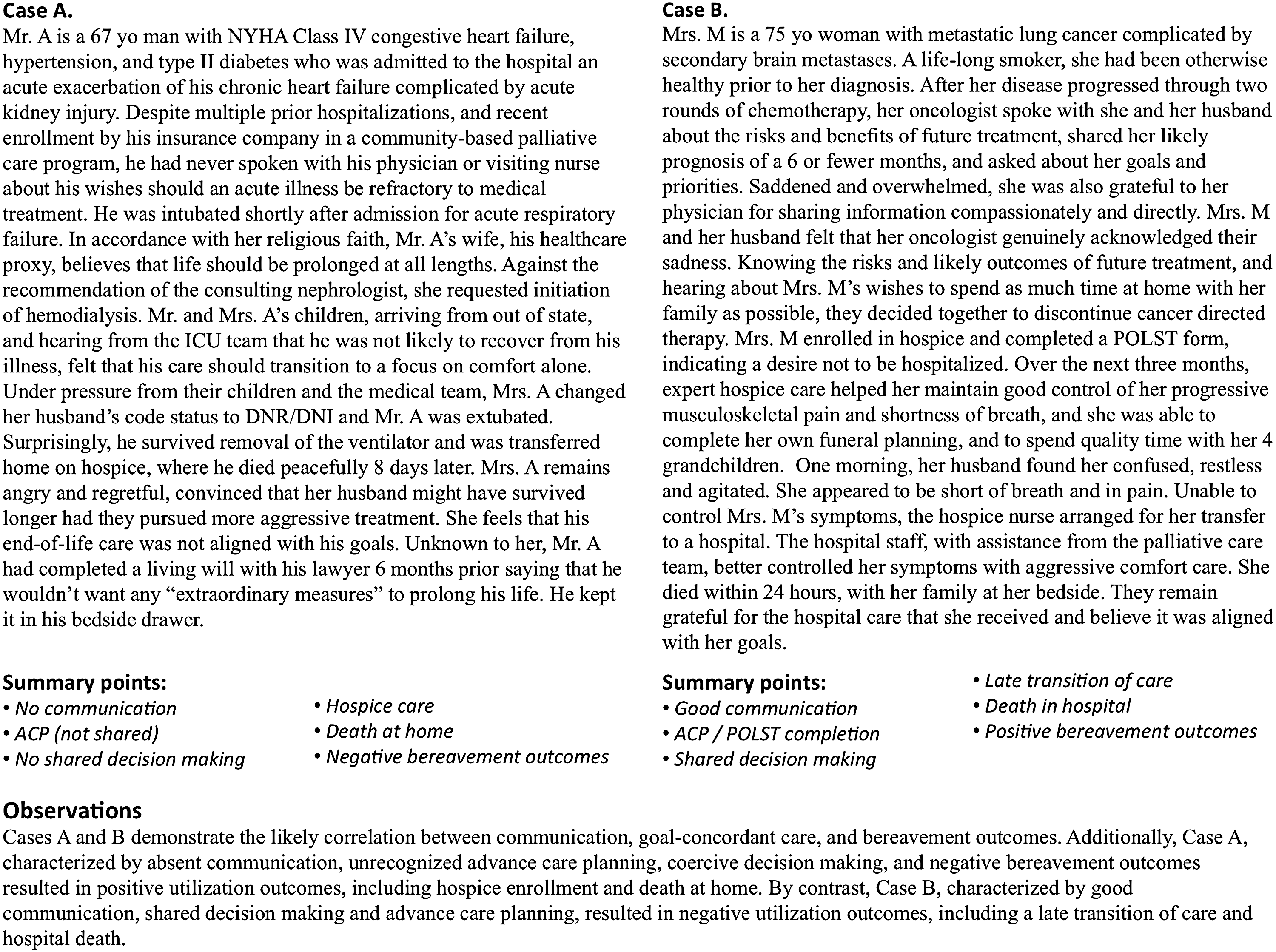
The complexity of measuring the quality of serious illness communication and goal-concordant care cannot be underestimated, and are evident from clinical experience. Figure 1 highlights two prototypical cases that illustrate this complexity. For example, patients like the man in Case A may have several markers of what might be considered high-quality care by traditional measures, but receive care that is perceived as discordant and results in poor bereavement outcomes. The converse, as in Case B, may also be true. Understanding the relationship between communication and goal-concordant care may support quality improvement efforts by identifying the most appropriate targets for quality measurement.
Cases illustrating the complexity of quality measurement of communication and goal-concordant care.
A Conceptual Model of the Relationship Between Communication and Goal-Concordant Care
A conceptual model illustrating the relationship between high-quality communication and goal-concordant care (Fig. 2) suggests candidate quality measurement domains. Communication quality in serious illness comprises at least four mutually reinforcing processes: information gathering, information sharing, responding to emotion, and fostering relationships. 12 These elements directly shape patient experience and, when done well, help patients feel known, informed, in control, and satisfied, thus improving well-being and quality of life.12–14 Good communication also enhances trust and therapeutic alliance,15–17 which lay the groundwork for SDM. 18
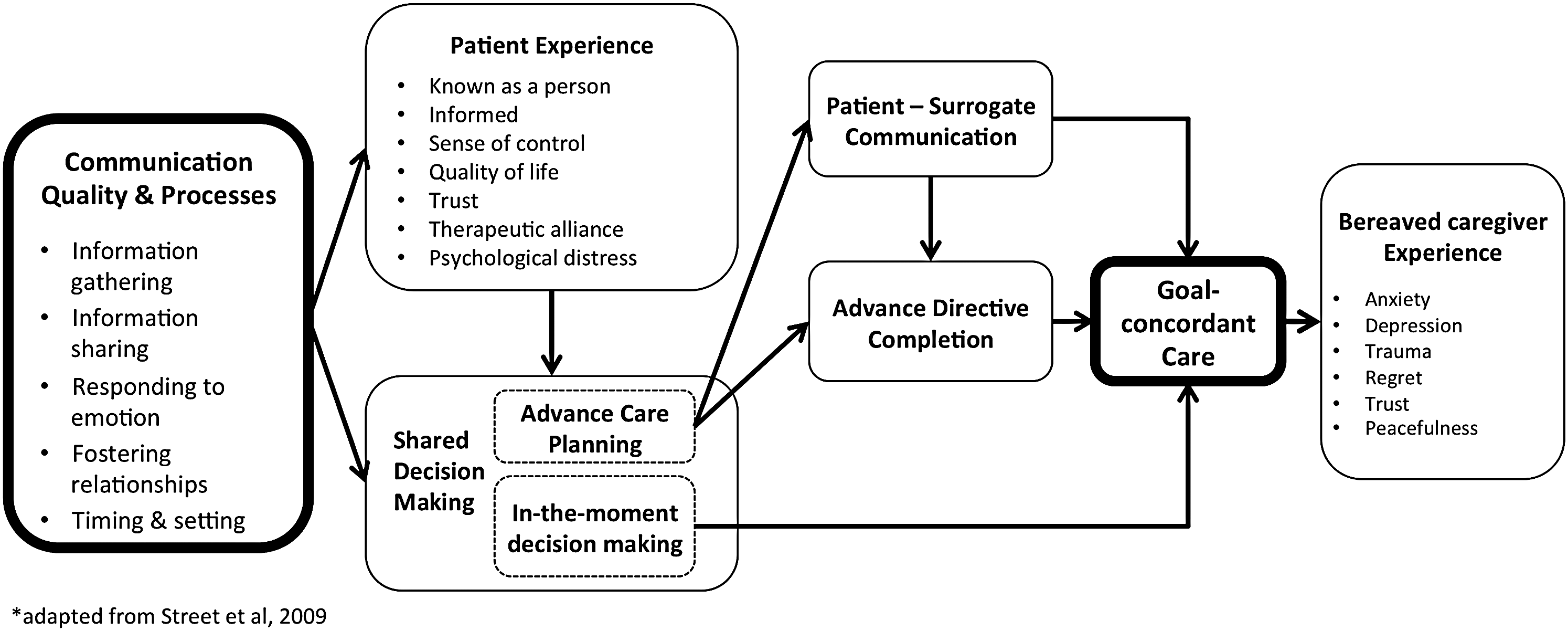
Clinician–patient communication improves patient and caregiver experience enables shared decision making, and mediates goal-concordant care. Adapted from Street et al. 27
SDM may occur in anticipation of future medical decisions during a time of decisional incapacity, known as advance care planning (ACP), or “in the moment,” when there is an immediately relevant decision to be made for a patient with capacity. ACP may result in goal-concordant care indirectly through either patient–surrogate communication and informed surrogate decision making at the time of critical illness, or clinician interpretation of an advance directive (AD). 19 By contrast, in-the-moment decision making may lead directly to goal-concordant care.
The receipt of goal-concordant care likely shapes the bereaved caregivers' experience as well. The perception that their loved one received care aligned with their values mitigates anxiety, depression, trauma, and regret, and enhances trust, peacefulness, and satisfaction with care. 20 When care is perceived as misaligned, the opposite may be true.
Measuring Communication and Its Outcomes: Challenges and Opportunities
Our model recognizes that multiple factors affect goal-concordant care. Table 2 presents a taxonomy of potential measures that correspond to these factors. Many are supported by evidence, some are currently used as quality indicators, and others are theoretical.
EOL, end of life; n/a, not applicable; POLST, physician's orders for life-sustaining treatment.
Criteria for assessing quality measures include their importance, validity, usability, and feasibility. 21 While we believe that these measures meet the threshold of importance, many require further testing for validity, usability, and feasibility. Common measurement challenges include the so-called “denominator problem,” 22 that is, uncertainty about which population should be measured, and the timing of measurement—at what points in the disease trajectory or post death should we survey patients or caregivers?
Communication quality and processes
Barriers to collecting and analyzing the content of clinical encounters, through recordings or medical record documentation, impede the goal of directly measuring the quality of communication. 23 An audio- or video-recorded medical encounter permits unfiltered analysis of communication content and is thus the measurement gold standard. To date, privacy concerns and logistical complexities have limited recording of communication to research studies.24–30 However, as the boundaries of private and public communication increasingly blur, and personal recording devices proliferate, we might soon easily record all clinical encounters. Advances in natural language processing and machine learning, offer the hope of analyzing recorded encounters at scale.
As an alternative to direct observation, these same technologies also make analysis of electronic health record (EHR) data increasingly feasible.31,32 Currently, EHR documentation poorly approximates actual communication, 33 yet health systems can mitigate this challenge by implementing documentation templates that capture key domains of communication. For example, documentation of illness understanding, information preferences, prognostic communication, and patient goals, values, and treatment preferences suggest high-quality communication by recording elements of SDM. 18
Survey instruments to assess patients or family members' perspectives on the quality of communication have been used as outcomes in randomized trials, but may be difficult to implement in clinical practice.34–37 The Consumer Assessment of Healthcare Providers and Systems (CAHPS®) surveys and Family Evaluation of Hospice Care measures also assess communication, although in a limited way.38,39 More robust communication-focused instruments could be systematically deployed to seriously ill patients at key inflection points in the serious illness trajectory, including at the time of diagnosis, and enrollment in post-acute and hospice care. Cross-validation of these with direct communication measurements will contribute to our understanding of their respective validity. 23
One need not measure communication quality to measure its occurrence. Quality improvement programs, such as the Serious Illness Care Program, 24 have demonstrated the feasibility of measuring the timing and setting of communication among seriously ill patients; researchers in Canada have recently validated a set of quality indicators that include communication processes. 40
Patient experience
Prospective or retrospective surveys may be used to directly or indirectly assess patient or family experience of communication quality.41–43 Patient ratings of communication and experience overlap conceptually and in practice, but are not the same. Therefore, it is important to assess both. Patient experience measures have driven improvement in care quality by enhancing adherence to recommended treatment processes, and are associated with improved outcomes and patient safety.44,45 Quality of life measures may also reflect patient experience, but most focus predominantly on the physical illness experience, which may respond less to communication.35,46,47 Ideally, clinician–patient communication helps patients feel known as people, informed, and in control of their care, measures of which remain underdeveloped.
Depression and anxiety commonly burden seriously ill patients and their families.48–51 Poor clinician communication can inadvertently contribute to these symptoms and interventions to improve communication have reduced symptoms of depression and anxiety.52,53 Conversely, well-intentioned communication may result in unintended consequences, including increased patient or family distress.36,54,55 For these reasons, a comprehensive assessment of communication outcomes and goal-concordant care should include measurement of anxiety, depression, or complicated grief as markers of the distress that poor communication or goal discordant-care may cause.
Shared decision making
Systematic and expert reviews highlight the difficulties of promoting, participating in, and measuring SDM.56–59 Systems may more feasibly measure the processes and anticipated outcomes of SDM, such as ACP or ACP engagement, than patient perceptions regarding the collaborative nature of their communication experience. 60 Studies measuring ACP processes demonstrate mixed outcomes. For example, the Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments (SUPPORT) study showed no meaningful improvements in care among patients randomized to an intervention that included ACP. 61 However, the Respecting Choices model of ACP has been shown to decrease hospitalizations and to improve caregiver awareness of patient wishes and perceived goal-concordant care.62,63
Patient–surrogate communication
Measuring patient–surrogate communication also carries benefit. 24 First, uninformed surrogates complicate end-of-life decision making. Second, surrogates commonly assess patient's wishes incorrectly and apply them inconsistently; neither surrogate assignment nor prior discussion of patient treatment preferences improve alignment on treatment choices in hypothetical scenarios. 64 Finally, patients vary in how much leeway they wish to give surrogates, with some deferring to surrogates even when decisions contradict previously stated preferences. 65 Furthermore, factors unrelated to clinician–patient communication (such as the patient–surrogate relationship) determine patient–surrogate communication. Despite these complexities, measuring patient–surrogate communication may facilitate quality improvement efforts to improve surrogate understanding of patient's wishes and may address gaps in our understanding of the mechanism by which ACP results in goal-concordant care.
AD completion
Several quality frameworks support documentation of treatment preferences in an AD.9,66,67 However, AD completion remains a problematic quality indicator for several reasons. First, ADs do not always reflect SDM.68–70 Second, patients' preferences may change as their illness progresses making previously completed AD no longer accurate.71,72 Third, ADs inconsistently demonstrate their impact on the delivery of goal-concordant care, with a majority of studies showing little association between the two. 73 Finally, limited portability and inconsistent interpretation by family and clinicians limit implementation of ADs.70,73 Legal documents, such as living wills, are not universally accessible. Portable medical orders, such as Physician's Orders for Life-Sustaining Treatment (POLST) or Medical Orders for Life-Sustaining Treatment (MOLST), have been shown to influence location of death in accordance with stated preferences, 74 but patient selection remains unclear and some have raised concerns about their interpretability and degree of patient centeredness. 75 Because they are increasingly utilized and will remain part of the complex landscape of serious illness care, 76 we should measure their completion and impact on goal-concordant care.
Goal-concordant care
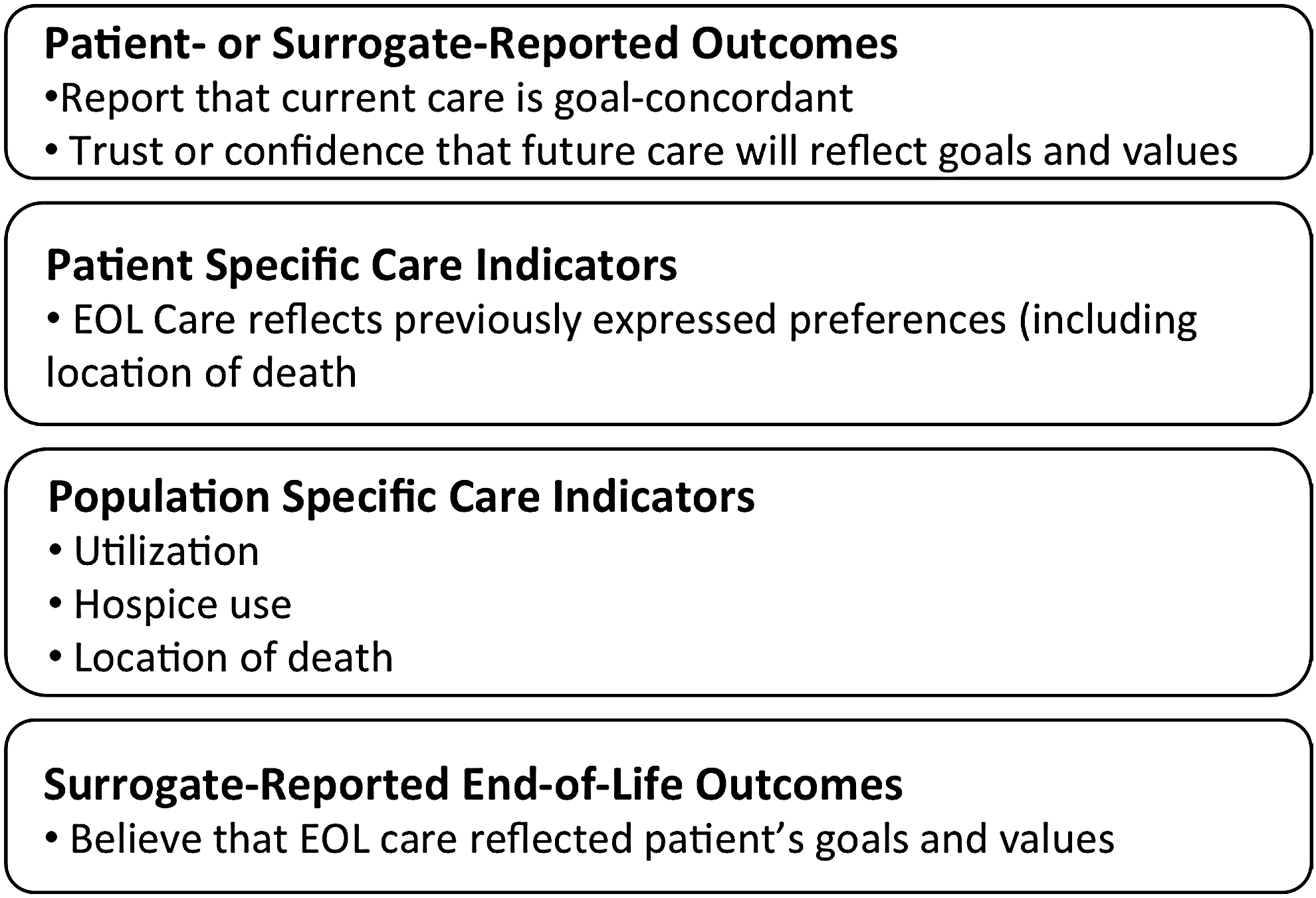
Healthcare systems can assess goal-concordant care in four ways (Fig. 3): (1) patient- or surrogate-reported outcomes of goal-concordant care, (2) patient-specific care indicators, (3) population-specific care indicators, and (4) bereaved caregiver reports of whether end-of-life care was goal concordant.
Measurement domains for goal-concordant care.
While not widely used, patient-reported assessments of goal-concordant care present an opportunity to measure goal-concordant care before death. The SUPPORT investigators measured goal-concordant care by assessing agreement between patient preference for care focused on life extension or comfort, and patient assessment of whether or not current care aligned with that preference. 61 Patients frequently value conflicting or contingent goals equally, 77 making such a “forced choice” to some degree a false one. However, it may help clarify a patient's highest priority, and whether or not a health system helps meet it. There may be other ways to prospectively assess goal-concordant care, including a single-item measure to assess confidence that a patient's current or future care aligns, or will align, with their goals and values.
Patient-specific outcomes compare a known preference, usually communicated through an AD or portable medical order, and an end-of-life outcome, including care utilization or location of death. Uncertainty about the timing of preference measurement and methodological constraints related to identifying deceased patients and collecting utilization data from multiple settings complicate these approaches. Additionally, patients may provide general guidance for care that may not easily translate into specific care options.
Population-specific outcomes include trends in healthcare utilization over time and location of deaths.78,79 Comparison to survey data about care preferences may suggest a population-level goal concordance of care. 80 Such measures may help shape policy, and a recent study suggests that they may be meaningful for individuals, as less hospital care and more hospice care relate to higher caregiver-reported EOL care-quality outcomes. 20
Measuring bereaved caregiver's perceptions regarding the goal concordance of their loved one's end-of-life care remains an untapped domain of quality assessment. While surrogates commonly predict patient's wishes inaccurately in hypothetical scenarios, 64 their shared experience with the dying patient may be the closest thing we have to the patient's own voice. 81 Because preferences can change as illness progresses, surrogates' beliefs about patient's goals may be more accurate than those previously recorded by patients. A recent study found that, when compared with caregivers who reported goal-concordant care, those reporting goal-discordant care rated the quality of communication and quality of care lower. 82 Limitations of this approach include the potential for multiple biases83–85 and challenges identifying surrogates. However, the Veterans Affairs administration's Bereaved Family Survey 86 and several mortality follow-back studies have demonstrated the feasibility of this approach.87–89
Bereaved caregiver experience
Finally, measuring the bereaved caregiver's experience represents an important quality measurement opportunity. When patients die, their loved ones are left to grieve, cope, and reconsider the care that took place over the patient's illness trajectory. Healthcare resulting in bereaved caregivers feeling more anxious, depressed, traumatized, or regretful may reflect poor-quality EOL care and communication.90,91 We do not know if a lack of perceived goal concordance predicts complicated grief, or other negative outcomes, but such a relationship is plausible and should be investigated.
Recommendations
The cases in Figure 1 demonstrate the likely correlation between communication, goal-concordant care, and bereavement outcomes. The measurement challenges illustrated by these scenarios inform our recommendations for quality measures that should be implemented now in the care of seriously ill patients, and recommendations for the future. Specifically, they illustrate the need for specific goal-concordant care measures.
Implementation-ready measures
Three quality indicators appear ready for implementation in cohorts of seriously ill patients: (1) timing and setting of serious illness communication; (2) patient (or surrogate) experience of communication and care; and (3) caregiver bereavement surveys that include assessment of perceived goal concordance of end-of-life care.
First, we advocate for measurement of when, where, and with whom communication happens, because it has the potential to drive improvement in the frequency, timing, and quality of communication. Communication is a prerequisite for delivering goal-concordant care, and sufficient evidence exists to suggest the benefit of timely, high-quality communication. Measuring this process is likely to have greater impact than measurement of AD completion alone.
Second, measurement of patient experience of communication and care will reflect the quality of communication and serious illness care as a whole. Some patient experience measures remain underdeveloped; others, including quality of life are valid, reliable, and meaningful.
Third, we advocate measurement of goal-concordant care through caregiver bereavement surveys, specifically by asking questions to assess whether caregivers believe that their loved one received care consistent with their values and preferences.
Future measurement candidates
We recommend prioritizing three quality indicators for further development: communication quality, prospective patient or family assessment of goal-concordant care, and the bereaved caregiver experience. First, applying existing tools and technology to the direct measurement of communication remains limited by data access and privacy concerns. These obstacles are surmountable. Doing so could revolutionize serious illness care by placing the clinician–patient communication in a position that reflects its primacy in patients' illness experiences. Second, prospectively assessing patient or surrogate-reported goal-concordant care may present real-time opportunities to improve communication and care. Preliminary findings from ongoing studies suggest that this outcome may be responsive to communication interventions. Third, attending to bereaved caregivers' experiences will shape our understanding and delivery of serious illness care. Some aspects of their experience may reflect neither communication quality nor goal-concordant care. The experience of the bereaved matters. If the deceased could speak, this would likely be the thing that many would say matters most.
The proposed quality measures highlight research priorities in serious illness communication, particularly as we consider their applicability to accountability programs. We must understand the responsiveness of these measures to interventions; assess at multiple time points the relationship between current, prospective, and retrospective reports of goal-concordant care and actual care outcomes; and assess the relationships between and relative impact of clinician–patient communication on patient–surrogate communication, AD completion, and goal-concordant care.
Conclusion
As we consider opportunities for systematic quality measurement in seriously ill patients, we advocate for ensuring that communication has occurred, and for measuring its impact. The most important outcomes of communication, and indeed all of serious illness care, are the patient experience and the receipt of goal-concordant care. We have the tools to measure both.
Future research can address knowledge gaps. Yet, the lack of complete data should not stop implementation in the short term. Negative patient experiences and the delivery of goal-discordant care currently cause harm to patients and families. Our intolerance of these outcomes must be matched by our willingness to measure them.
Footnotes
Acknowledgments
The authors thank Gordon and Betty Moore Foundation, Cambia Health Foundation, and Joanna Paladino, MD.
Author Disclosure Statement
No competing financial interests exist.