
Abstract
Abstract
Purpose:
Reducing intraocular pressure (IOP) seems to be the only treatment that slows progression in glaucoma. The IOP can be decreased by pharmaceutical treatment, laser [selective laser trabeculoplasty (SLT)] treatment, or surgery. Prostaglandin analogues have been postulated to share action mechanisms with SLT and to possibly diminish the effects of SLT treatment. The aim of the current study was to investigate the effects of prostaglandin analogues in inflammation and IOP reduction after SLT treatment.
Methods:
Prospective nonrandomized study. One hundred and eighteen patients were included in the study. Inclusion criteria: Glaucoma (open-angle or pseudoexfoliation glaucoma) patients who will be treated with SLT. Inflammation was measured with a laser flare meter (Kowa FM-500). Measurements were made before SLT and then 2 h, 1 week, and 1 month after SLT treatment. IOP was also checked at the same time intervals. The SLT treatment was performed over 90°. All patients were divided into two groups: those receiving prostaglandins analogues and those treated with nonprostaglandin analogues.
Results:
Inflammation before and after SLT showed no significant difference between the groups at all the time intervals studied (t-test, before: P=0.16; 2 h: P=0.14; 1 week: P=0.12; and 1 month: P=0.36). IOP reduction showed no significant difference between the groups (t-test, P=0.31).
Conclusions:
SLT treatment effects do not seem to be influenced by the use of prostaglandin analogues.
Introduction
The ALT was introduced about 30 years ago and involves the use of a blue/green argon laser (major wavelength peaks at 488 nm and 514 nm) to treat the anterior part of the trabecular meshwork and thereby improves aqueous flow and thus reduces IOP. The SLT is a rather new treatment alternative. It involves using a frequency-doubled, Q-switched Nd:YAG laser (532 nm) that delivers a low-energy, large spot, very brief pulse to selectively targeted cells of the trabecular meshwork. This laser application is thought to stimulate the pigmented trabecular meshwork cells and thus facilitates improved aqueous outflow. The SLT treatment may hold clinical advantages over the ALT treatment.
The ALT treatment induces inflammation in the anterior chamber due to the fact that the laser disrupts cells in the trabecular meshwork. Martinez-de-la-Casa et al., 4 when using the laser flare meter (Kowa FM-500), reported lower inflammation in the anterior chamber when comparing SLT with ALT treatment. Little information is to be found in the literature regarding inflammation status in the anterior chamber after SLT treatment and the influence of medications on inflammation after SLT treatment.
Topical prostaglandin analogues have been demonstrated to be effective medications for lowering IOP.5–7 These agents have been shown to lower IOP mainly by increasing uveo-scleral outflow.8–10 However, Alvarado et al. 11 showed in a translational model that prostaglandin analogues could have direct effects on the trabecular meshwork as well. Studies on the effects of medications and particularly prostaglandin analogue medications in SLT results are controversial. Scherer 12 showed, in a retrospective study, a greater average IOP reduction after SLT when patients were treated with prostaglandin analogues. On the other hand, Alvarado et al. 11 showed that prostaglandin analogues may interfere with SLT, thus decreasing SLT effects. Singh et al., 13 in a retrospective study published in 2009, did not find that prostaglandin analogues affected outcomes after SLT.
The aim of the current study was to investigate the influence of prostaglandin analogues in inflammation and IOP reduction after SLT treatment.
Methods
Study design and methods
This was a prospective nonrandomized comparative study to assess the effects of prostaglandin analogues in inflammation and IOP reduction after SLT treatment.
Inclusion criteria: Patients suffering from glaucoma, primary open angle glaucoma (POAG), or pseudoexfoliation glaucoma (PXFG), who underwent SLT. If both eyes were treated, then one eye was chosen at random to be included in the study. Patients were included consecutively. All patients were treated with at least one kind of IOP-lowering topical medication.
Exclusion criteria:
• Patients treated with cortisone or immunosuppressive drugs. • Patients suffering from ocular or systemic inflammatory diseases. • Patients who cannot be treated with SLT due to the eye's characteristics (shallow anterior chamber) or bad collaboration. • Patients treated with Pilocarpine (miosis makes laser flare measurements very difficult).
Patients coming to the Glaucoma Department at the St. Erik Eye Hospital for SLT treatment who fulfilled the inclusion criteria were asked to participate in the study. Patients were enrolled between January 2009 and December 2009. The study was approved by the Ethical Committee at the Karolinska Institutet (approval No. 2009/1). Informed consent was obtained. The authors confirm adherence to the tenets of the Declaration of Helsinki.
A comprehensive medical and ocular history was obtained. All patients were asked about present inflammatory diseases and treatments. Ophthalmological examination was performed before including patients in the study. Visual acuity, IOP measurements, optic nerve status, gonioscopy, and the presence or absence of exfoliation were registered. Visual acuity was recorded using a Snellen's chart. The IOP was measured using a Goldmann's applanation tonometer. Gonioscopy was performed in a darkroom using a goniolens with an undilated pupil, and the anterior chamber angle was classified into 0-IV (according to Shaffer) and pigmentation was classified into 0–3. Pupils were dilated and exfoliation was checked; exfoliation was registered as present or absent. Then, the optic nerve status was evaluated using a 90-D lens. IOP, slit-lamp, and laser flare measurements were made before SLT and then 2 h, 1 week, and 1 month after SLT.
The SLT is a Q-switched, frequency-doubled Nd:YAG, wavelength around 532 nm. The SLT uses a single pulse (pulse duration 3 ns) and the spot's size is estimated to be 400 μm. In the current study, SLT treatment was performed over 90° with the SLT Solo laser (Ellex) using some 25–30 spots applied to the trabecular meshwork. Traditionally, 180° of the trabecular meshwork is treated, but a study published by Chen et al. 14 showed similar effects when 90° of the trabecular meshwork was treated. The initial energy used was 0.9 mJ. The energy was increased or decreased until bubble formation appeared and was then decreased by 0.1 mJ for the remainder of the treatment. The energy used in the current study was in the range 0.9–1.1 mJ.
All patients continue with the same medical treatment after SLT. No patient was treated with corticoids, NSAIDs, or apraclonidine before or after SLT treatment.
Outcome parameters
The primary outcome of this study was inflammation. Flare measurements were made with a laser flare meter (Kowa FM-500). The Kowa FM-500 is based on the measurement principle of detecting scattered laser light. The intensity of the scattered light (directly proportional to the amount of particle flare) is measured by a photo-multiplier, which generates an electric signal. Flare measurements in the study were made before SLT (baseline) and then 2 h, 1 week, and 1 month following SLT.
The unit of measurement employed by the FM-500 is photon counts per millisecond (pc/ms). A 1+ seen in the slit-lamp corresponds to a laser flare photometry value of 28.3±4.8 pc/ms and a flare of 3+ to a value of 82.5±5.2 pc/ms according to Guex-Crosier et al. 15 Herbort et al. 16 have shown that even normal eyes express a normal flare measured to be 4 pc/ms. Laser flare measurements were made at least five times according to Shah et al. 17 and the average value was calculated. The IOP was checked using a Goldmann's applanation tonometer (Haag Streit). Measurements were made at the same time intervals as for the flare measurements.
To analyze the effect of prostaglandin analogues on SLT efficacy, the eyes were categorized according to whether they received a topical prostaglandin analogue (travoprost, latanoprost, or bimatoprost) alone or in combination with other glaucoma medications in the patients' glaucoma pharmaceutical therapy before SLT treatment. The eyes that did not receive prostaglandin analogues included those treated with other topical agents (carbonic anhydrase inhibitors, α-2 agonists, or β-blockers). All included patients were on pharmaceutical treatment for at least 3 months before SLT and continued with the same pharmaceutical treatment at least 1 month after SLT.
Statistical considerations
Laser flare: Measurements were made in both groups: those treated with prostaglandin analogues and those treated with other agents. A two-tailed t-test was performed to test the difference between the two groups at each time interval (before SLT and 2 h, 1 week, and 1 month after SLT). Significance level was 5%.
IOP: Measurements were compared before SLT (baseline) and 1 month after SLT. Measurements were made in both groups: those treated with prostaglandin analogues and those treated with other agents. A two-tailed t-test was performed to test the difference between the two groups. Significance level was 5%.
Sample size was estimated, with alpha=0.05, power 0.95, estimated standard deviation (SD)=2, and in order to detect a difference of 2 pc/ms between the groups, 26 patients were needed in each group. All statistical analysis was performed using STATA statistical software (Statacorp).
Results
Demography
A total of 118 eyes (patients) were identified during the study period, of which 78 eyes received prostaglandin analogues and 40 eyes received nonprostaglandin agents. All participants attended their appointments. The average age was 72.53 (SD: 10.3) years. The gender distribution was 46.25% men and 53.75% women. Diagnosis distribution: 46.25% POAG and 53.75% PXFG (see Table 1).
Two-tailed t-test.
Fisher's exact test.
IOP, intraocular pressure; SLT, selective laser trabeculoplasty; POAG, primary open angle glaucoma; PXF, pseudoexfoliation; SD, standard deviation.
Endpoints
Inflammation: Flare was measured at the four different time intervals—before SLT and 2 h, 1 week, and 1 month after SLT in eyes treated with prostaglandin analogues and eyes treated with nonprostaglandin analogues. No significant difference in flare was found between the two groups at any of the time intervals tested (t-test, before: P=0.16; 2 h: P=0.14; 1 week: P=0.12; and 1 month: P=0.36) (Fig. 1).
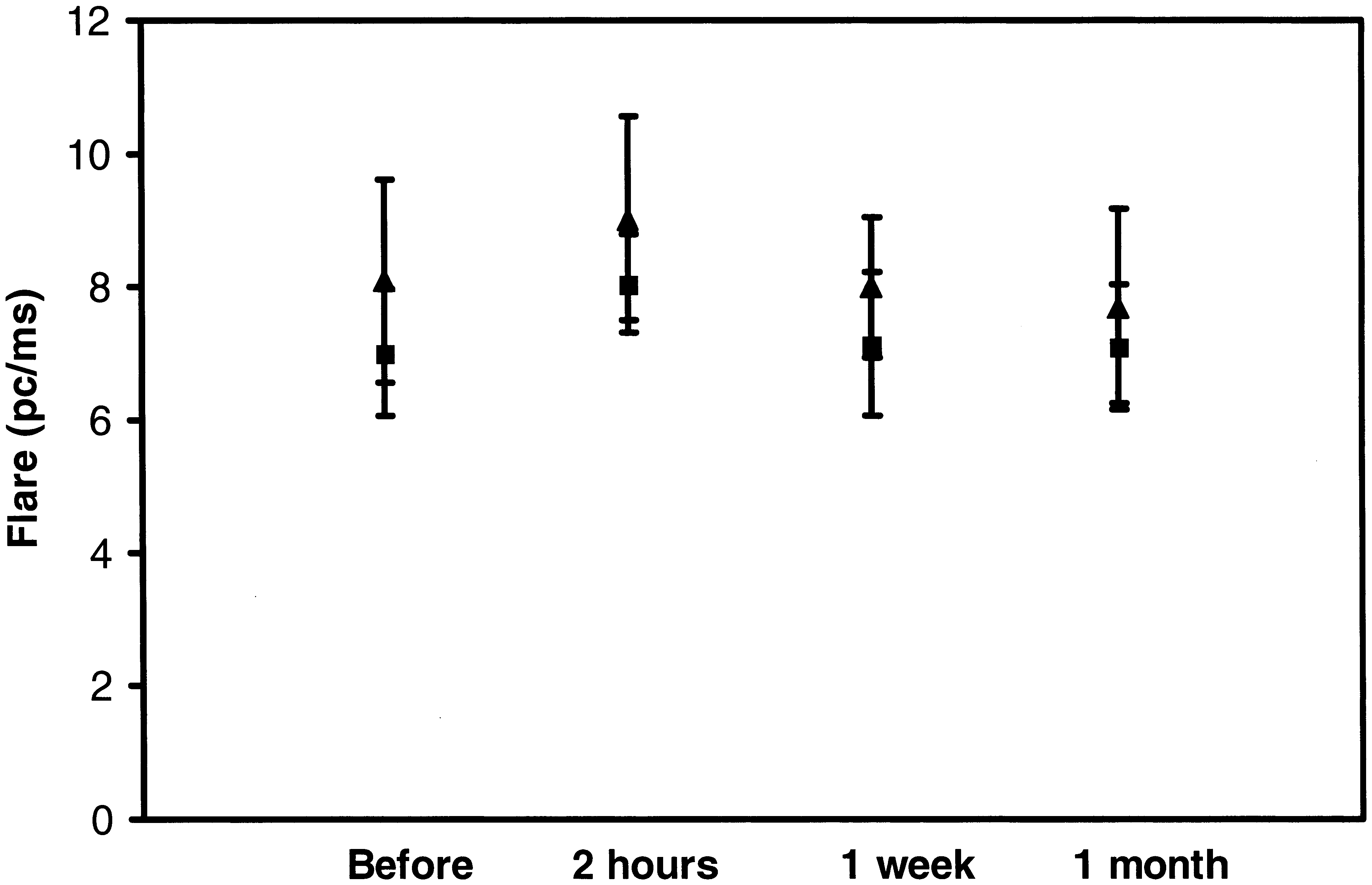
Flare measurements in both groups at different time points after SLT treatment; the bars represent 95% confidence interval for the mean. ▴ represents the mean for prostaglandin analogues group. ▪ represents the mean for the nonprostaglandin analogues group (t-test, before: P=0.16; 2 h: P=0.14; 1 week: P=0.12; 1 month: P=0.36). SLT, selective laser trabeculoplasty.
Intraocular pressure: The IOP reduction 1 month after SLT in the eyes treated with prostaglandin analogues was 6.35 mmHg, while the IOP reduction in the eyes treated with nonprostaglandin agents was 5.77 mmHg. The difference was not significant (t-test, P=0.31) (Fig. 2).
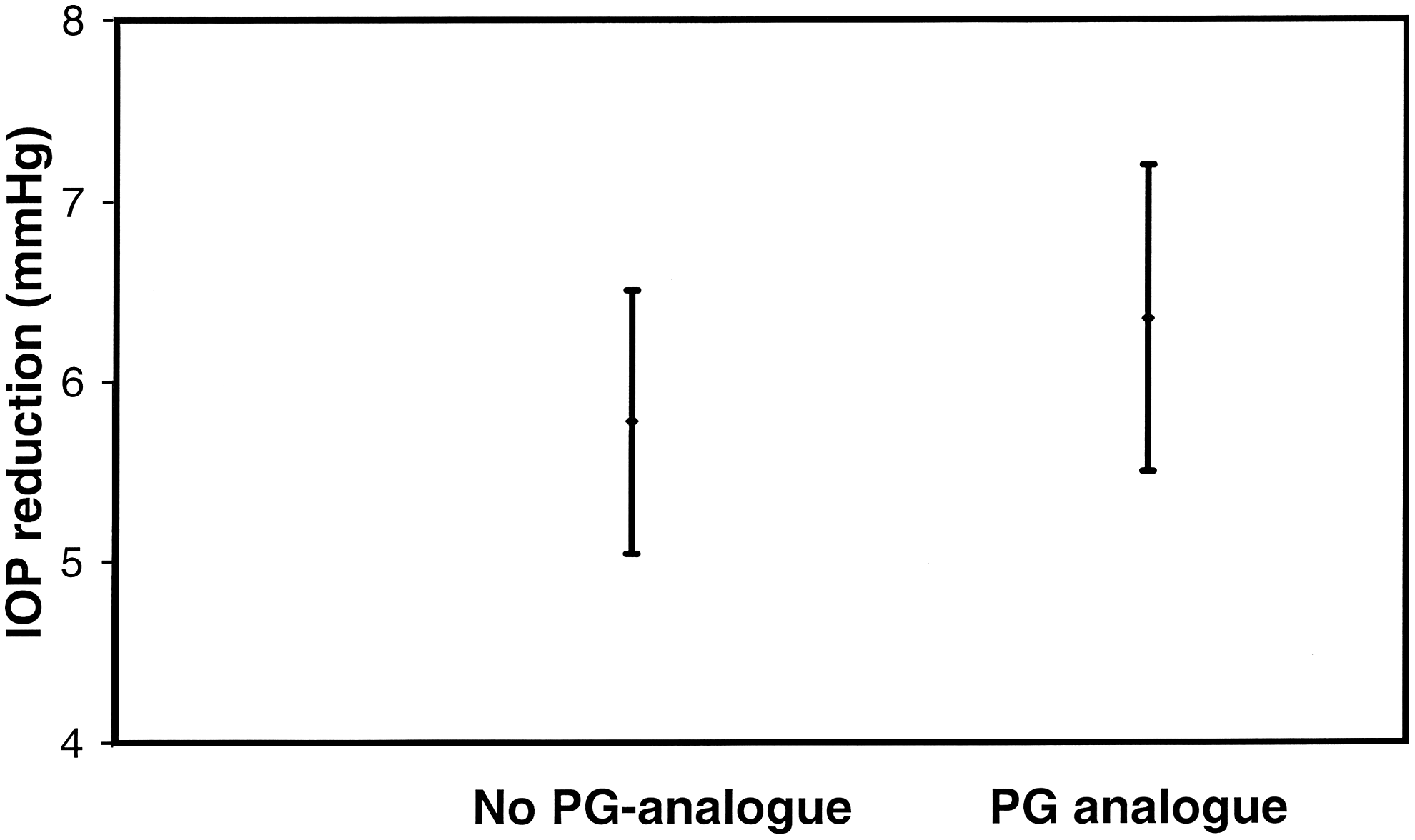
Intraocular pressure (IOP) reduction comparing before SLT and 1 month after SLT treatment; the bars represent 95% confidence interval for the mean (t-test, P=0.31).
Discussion
The current prospective study showed that prostaglandin analogues did not induce inflammation after SLT treatment when the eyes were treated over 90°. Information about inflammation after SLT treatment is scarce. One of the first studies published is the one written by Latina et al. 18 with 180° SLT showing that 83% of SLT-treated eyes exhibited mild-to-moderate inflammation, appearing within 1 h after treatment, decreasing by 24 h after treatment, and nearly resolved in all cases within 5 days. Martinez-de-la-Casa et al. 4 evaluated inflammation using the same device as the one used in this study, the Kowa laser flare meter, and found significantly lower flare readings after SLT than ALT.
The fact that the eyes were treated with 90° SLT must be taken into consideration. In comparable studies, the eyes have been treated with 180° SLT. The lower laser energy dose used in this study can in some way explain why there is no difference in inflammation between eyes treated with prostaglandin analogues and those not. However, all eyes (prostaglandin analogue users and nonusers) were treated with SLT in a similar manner using the same amount of laser energy.
Prostaglandins are common mediators in the inflammatory response. It has been postulated that prostaglandin analogues could induce inflammation in the eye. In vitro studies have shown that prostaglandins released by endothelial cells exhibit strong chemoattractant activity for neutrophils and macrophages 19 and that latanoprost can significantly increase the expression of apoptotic markers. 20
In vivo studies with cases of macular edema or uveitis have been described in patients at high risk for inflammatory reactions.21,22 No inflammation due to prostaglandin analogues was found in the current study when 90° of the trabecular meshwork was treated with SLT. Inflammation pathways in the eye for prostaglandin analogues are not well described. The SLT treatment and prostaglandin analogues probably follow different inflammation pathways. Inflammation markers were not investigated in the current study. Further in vivo or in vitro studies are needed to elucidate the roll of different markers as well as inflammation pathways after SLT treatment.
With regard to the hypotensive effect of SLT, we found a significant IOP reduction after treatment. The absolute mean IOP reduction in all the treated eyes in the current study was 6.06 mmHg, from a baseline of 23.66 to 17.60 mmHg after 1 month. These results correlate well with the findings published by Latina et al., 18 who found a mean IOP reduction of about 6 mmHg 4 weeks (1 month) after SLT and then the mean IOP reduction decreased toward 5.8 mmHg after 26 weeks. Several studies have been published after Latina's initial report. In general, these studies reported a mean IOP reduction in the range of 4–6 mmHg in the short term (approximately 6 months). 3 In the current study, no difference in IOP reduction was found when comparing prostaglandin analogue users with nonusers. The results are in line with previous results published by Singh et al. 13 However, Scherer 12 described a difference in IOP reduction when comparing prostaglandin analogue users and nonusers when the baseline IOP was 17.75 mmHg. IOP levels before SLT treatment in different studies might be considered. The baseline IOP in the current study was 23.66 mmHg. The SLT efficacy decreases with lower IOP. 23 It is possible to speculate that with a lower baseline IOP, the effects of eye drops are more prominent than the effects of SLT and this can explain the reason why Scherer found a difference between the groups. In an article published in 2009, Alvarado et al. 11 described in a translational model (in vitro-in vivo) a possible common action mechanism for prostaglandin analogues and SLT. The authors concluded that prostaglandin analogues and SLT may share the same pathway (at the trabecular meshwork) for IOP reduction. The authors recommended that prostaglandin analogues might be discontinued before SLT treatment to achieve a good IOP reduction with SLT treatment. According to Alvarado et al., the IOP reduction after SLT treatment found in the prostaglandin analogue users group might be lower than in the group of nonusers. We did not find any difference. Comparisons among studies are difficult to perform due to the differences in the populations studied, diagnosis, follow-up periods, laser protocols, and so on.
One of the limitations of the study is the relatively short follow-up period of 1 month. The reason for this short follow-up is that the study focused principally on inflammation after SLT treatment. According to previous studies,4,18 inflammation decreases 1 month after SLT treatment. Further, after this time, some patients from each group have their glaucoma medication discontinued or SLT treatment repeated and this can alter the results. Considering IOP, several previous studies have indicated that IOP remains stable at 6 months 18 and 18 months. 24 Therefore, the 1 month IOP values are likely to be predictive of future IOP control.
Another possible limitation is selection bias. Patients were recruited at a tertiary care center where patients usually require more treatment. It is also necessary to consider the high number of patients exhibiting pseudoexfoliation. Pseudoexfoliation is a common finding among patients in Northern Europe. Pseudoexfoliation prevalence in northern Sweden is estimated to be 23% at 66 years and 61% at 87 years. 25 In our study, 53.75% of all patients showed pseudoexfoliation, in part due to the high pseudoexfoliation prevalence in Sweden, but also due to the fact that pseudoexfoliative glaucoma generally needs additional therapy and SLT seems to be a good alternative. The high prevalence of pseudoexfoliation in our study population may introduce selection bias.
To the best of our knowledge, this is the first study investigating the influence of prostaglandin analogues and inflammation in the anterior chamber after SLT treatment treating just 90°, without any kind of antiinflammatory treatment before or after SLT, and using a quantitative method to measure inflammation in the anterior chamber. The overall lower inflammation levels found were probably due to the fact that a small amount of the trabecular meshwork was treated with consequently decreased total energy delivered.
Footnotes
Acknowledgment
Marcelo Ayala was supported by a grant from the Signhild Engkvist's Foundation.
Author Disclosure Statement
No competing financial interest exists.