
Abstract
Introduction:
Xinmailong injection (XMLI) is a common Traditional Chinese Medicine for treating chronic heart failure (CHF) in China. However, strong evidence-based medical evidence for XMLI is lacking.
Purpose:
To evaluate the efficacy and safety of XMLI in patients with CHF.
Methods:
PubMed, the Cochrane Library, Web of Science, Embase, China National Knowledge Infrastructure, Wanfang Database, VIP Database for Chinese Technical Periodicals, and Chinese Biomedical Literature Database were searched to identify randomized controlled trials (RCTs) of XMLI for CHF from the inception of the databases to November 2, 2024. The Cochrane risk of bias tool for randomized trials (RoB 2) was used to evaluate the quality of studies, and STATA 17.0 software was used to perform a meta-analysis of left ventricular ejection fraction (LVEF), left ventricular end-diastolic diameter (LVEDD), brain natriuretic peptide (BNP), N-terminal pro-brain natriuretic peptide (NT-proBNP), 6-min walking distance (6-MWD), and adverse reactions. The quality of evidence was rated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Results:
Twenty-three RCTs comprising 2643 patients were included. Meta-analysis showed that compared with those under conventional Western drug treatment (CWT), combined XMLI and CWT effectively increased LVEF (mean difference [MD] = 6.66, 95% confidence interval [CI] [5.23, 8.09], Z = 9.12, p < 0.001) and 6-MWD (MD = 44.01, 95% CI [28.63,59.38], Z = 5.61, p < 0.001) and reduced LVEDD (MD = −4.19, 95% CI [−5.55, −2.83], Z = −6.05, p < 0.001), BNP (MD = −178.84, 95% CI [−230.29, −127.40], Z = −6.81, p < 0.001), and NT-proBNP (MD = −490.95, 95% CI [−729.40, −252.50], Z = −4.04, p < 0.001). There were no statistically significant differences between the two adverse reactions (risk ratio [RR] = 1.47, 95% CI [0.73,2.99], Z = 1.08, p = 0.28). The GRADE assessment rated adverse reactions as moderate-quality evidence, while LVEDD, BNP, NT-proBNP, and 6-MWD were classified as low-quality evidence, and LVEF was categorized as very low-quality evidence.
Conclusions:
This systematic review demonstrates that combining XMLI with CWT is effective and safe for managing CHF and offers an evidence-based adjunctive therapeutic strategy. Further high-quality clinical trials are required to investigate the prognostic implications and long-term outcomes.
Introduction
Heart failure (HF) is the end stage of various cardiac diseases. It is a complex clinical syndrome resulting from structural or functional cardiac abnormalities, characterized by dyspnea, fatigue, pulmonary congestion, and peripheral edema. 1 The global incidence of HF increases with age. Among individuals aged >45 years old, the incidence rate is 0.8%. As age increases by 20 years, the incidence may intensify by 1.3%. The five-year mortality rate following diagnosis is as high as 67%, causing a large economic burden on the global health care system. 2 In clinical practice, the treatment agents for chronic heart failure (CHF) primarily include diuretics, β-blockers, angiotensin-converting enzyme inhibitors, mineralocorticoid receptor antagonists, and sodium-glucose cotransporter 2 inhibitors. However, despite high-dose diuretic therapy, volume overload persists in some patients after discharge. In advanced HF, even with optimal pharmacological treatments, systolic and diastolic dysfunctions persist, and HF symptoms remain unresolved. 3 Therefore, CHF treatment remains highly challenged.
Traditional Chinese Medicine (TCM) has a long history in the treatment of CHF, and the use of TCM alone or combined with Western medicine improves patient prognosis. 4 –6 Xinmailong injection (XMLI) is a bioactive peptide preparation extracted from Periplaneta americana. The primary active ingredients are adenosine, inosine, protocatechuic acid, and pyroglutamate dipeptides. 7 Clinical studies have demonstrated the therapeutic potential of XMLI in CHF. However, current studies are limited by small sample sizes and insufficient evidence, and the systematic analysis lacks literature updates and fails to reveal the influence of baseline indicators on outcomes. 8 This study aims to systematically evaluate the efficacy and safety of XMLI in CHF treatment.
Materials and Methods
The protocol for this meta-analysis has been registered in PROSPERO (no. CRD42024574757) and reported per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (2020). 9
Search strategy
Two reviewers (S.-W.Z. and J.-P.C.) searched PubMed, the Cochrane Library, Web of Science, Embase, China National Knowledge Infrastructure, Wanfang Database, VIP Database for Chinese Technical Periodicals, and Chinese Biomedical Literature Database, from the database inception to November 2, 2024. The search terms included “Xinmailong Injection,” “Xinmailong,” “heart failure,” “chronic heart failure,” “randomized controlled trial (RCT),” “RCT,” and “randomized.” The search algorithm focused on the search terms mentioned in the title, abstract, and keywords. No language restrictions were imposed. The detailed search strategies are presented in Supplementary Table S2.
Inclusion and exclusion criteria
The inclusion criteria were (1) population: patients diagnosed with CHF; (2) intervention: the combination of XMLI with conventional Western drug therapy (CWT); (3) control: CWT alone based on HF guidelines 1,2 ; (4) outcome: primary: left ventricular ejection fraction (LVEF); secondary: left ventricular end-diastolic diameter (LVEDD), brain natriuretic peptide (BNP), N-terminal pro-brain natriuretic peptide (NT-proBNP), 6-min walking distance (6-MWD), and adverse reactions. Studies reporting at least one outcome measure were included; (5) study design: RCTs, regardless of blinding or allocation concealment.
The excluded criteria were (1) animal experiments or cellular studies, (2) literature reviews or meta-analyses, (3) case reports, (4) literature with inconsistent data or incomplete access to key information, (5) clinical studies with clearly erroneous designs, and (6) duplicate publications.
Data extraction and literature quality assessment
Two trained reviewers (S.-W.Z. and H.-Q.Z.) independently conducted a literature search and screening. Disputed studies were discussed or assessed for inclusion by a third author (H.-X.L.). Excel was used to organize the required information. If essential information in the original article was unclear, erroneous, or ambiguous, the corresponding author was contacted via email. Studies were excluded if the actual effective original data were unavailable.
According to the Cochrane Handbook, 10 two evaluators (S.-W.Z. and X.L.) independently assessed the quality of the included studies using the Cochrane risk of bias tool for randomized trials (RoB 2). The assessment included seven domains, such as the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Differences in opinion were resolved through the involvement of a third author (H.-X.L.), if necessary.
Statistical analysis
The meta-analysis was conducted using STATA 17.0 software. Risk ratio (RR) was used as the effect size for dichotomous variables. For continuous variables, the means and standard deviations of the differences before and after treatment were used, with the mean difference (MD) serving as the effect size. Each effect size was reported with a 95% confidence interval (CI). 11,12 According to the recommendations of the Cochrane Handbook and study design characteristics, a random-effects model using the DerSimonian–Laird method was adopted by default for the meta-analysis. The heterogeneity of the included studies was analyzed. I 2 ≤ 50% indicated low heterogeneity, and I 2 > 50% indicated substantial heterogeneity. Subgroup analyses were performed to investigate the sources of heterogeneity. Sensitivity analyses were performed to assess the robustness of the results. A funnel plot and Egger’s test were performed to analyze publication bias when the number of studies exceeded ten. p-Value <0.05 was considered statistically significant.
Evaluation of the quality of evidence
Two evaluators (S.-W.Z. and J.-P.C.) assessed the quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. The quality of evidence rating for each outcome was assessed based on the risk of bias, inconsistency, indirectness, imprecision, and other considerations.
Results
Literature screening results
According to the search strategy, 766 studies were examined. After removing the duplicates, 266 studies remained. A total of 208 studies that did not meet the inclusion criteria were excluded after reading the titles and abstracts. Twenty-three studies were included after reading the full text, comprising 2643 patients. Figure 1 illustrates the literature search process. Table 1 summarizes the basic characteristics of the included studies.

Studies screening flowchart.
Characteristics of Included Studies
① BNP;② NT-proBNP;③ LVEF;④ LVEDD;⑤ 6-MWD;⑥ adverse reactions.
6-MWD, 6-min walking distance; BNP, brain natriuretic peptide; C, control group; CWT, conventional Western drug therapy; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; NR, data not reported in the original study; NT-proBNP, N-terminal pro-brain natriuretic peptide; T, treatment group; XMLI, Xinmailong injection.
Risk of bias assessment
Ten studies described the randomization method, whereas 13 only mentioned randomization without specifying the method. Only one study mentioned allocation concealment. Two studies reported double blinding. No studies mentioned statistical blinding. Overall, one study was classified as low risk, while 22 were rated as having some concerns. The bias analyses are presented in Figure 2.

Risk of bias summary
Primary outcome
A total of 21 studies that explored LVEF and comprised 2445 patients were included. A random-effects model was adopted for the analysis based on a priori methodological considerations. The XMLI group was more effective in increasing LVEF compared with CWT (MD = 6.66, 95% CI [5.23,8.09], Z = 9.12, p < 0.001) (Fig. 3). The heterogeneity test suggested significant heterogeneity (I 2 = 90.97%, p < 0.001). No significant sources of heterogeneity were identified in subgroup analyses stratified by mean age, LVEF, treatment course, and sample size (Table 2). No outliers were observed in the sensitivity analysis (Supplementary Fig. S1).

Forest plots for left ventricular ejection fraction (LVEF).
Subgroup Analysis of LVEF
CI, confidence interval; LVEF, left ventricular ejection fraction; MD, mean difference.
Secondary outcomes
Left ventricular end-diastolic diameter
Eleven studies explored LVEDD, including 1185 patients. A random-effects model indicated that the XMLI group was more effective in reducing LVEDD levels compared with CWT (MD = −4.19, 95% CI [−5.55, −2.83], Z = −6.05, p < 0.001) (Fig. 4). Significant heterogeneity existed (I 2 = 81.87%, p < 0.001). Subgroup analyses stratified by mean age, LVEF, treatment course, and sample size revealed no significant sources of heterogeneity (Table 3). Sensitivity analysis showed that there were no data outliers (Supplementary Fig. S2).

Forest plot for left ventricular end-diastolic diameter (LVEDD).
Subgroup Analysis of LVEDD
CI, confidence interval; LVEDD, left ventricular end-diastolic diameter; LVEF, left ventricular ejection fraction; MD, mean difference.
Brain natriuretic peptide and N-terminal pro-brain natriuretic peptide
Eight studies, including 978 patients, considered the BNP levels. A random-effects model was adopted. Combined XMLI and CWT more effectively reduced BNP levels than did CWT alone (MD = −178.84, 95% CI [−230.29, −127.40], Z = −6.81, p < 0.001) (Fig. 5). Heterogeneity tests showed I 2 = 96.16% (p < 0.001), indicating the presence of substantial heterogeneity. No significant sources of heterogeneity were identified in subgroup analyses stratified by mean age, LVEF, treatment course, and sample size (Table 4). Sensitivity analysis revealed that there were no data outliers (Supplementary Fig. S3).
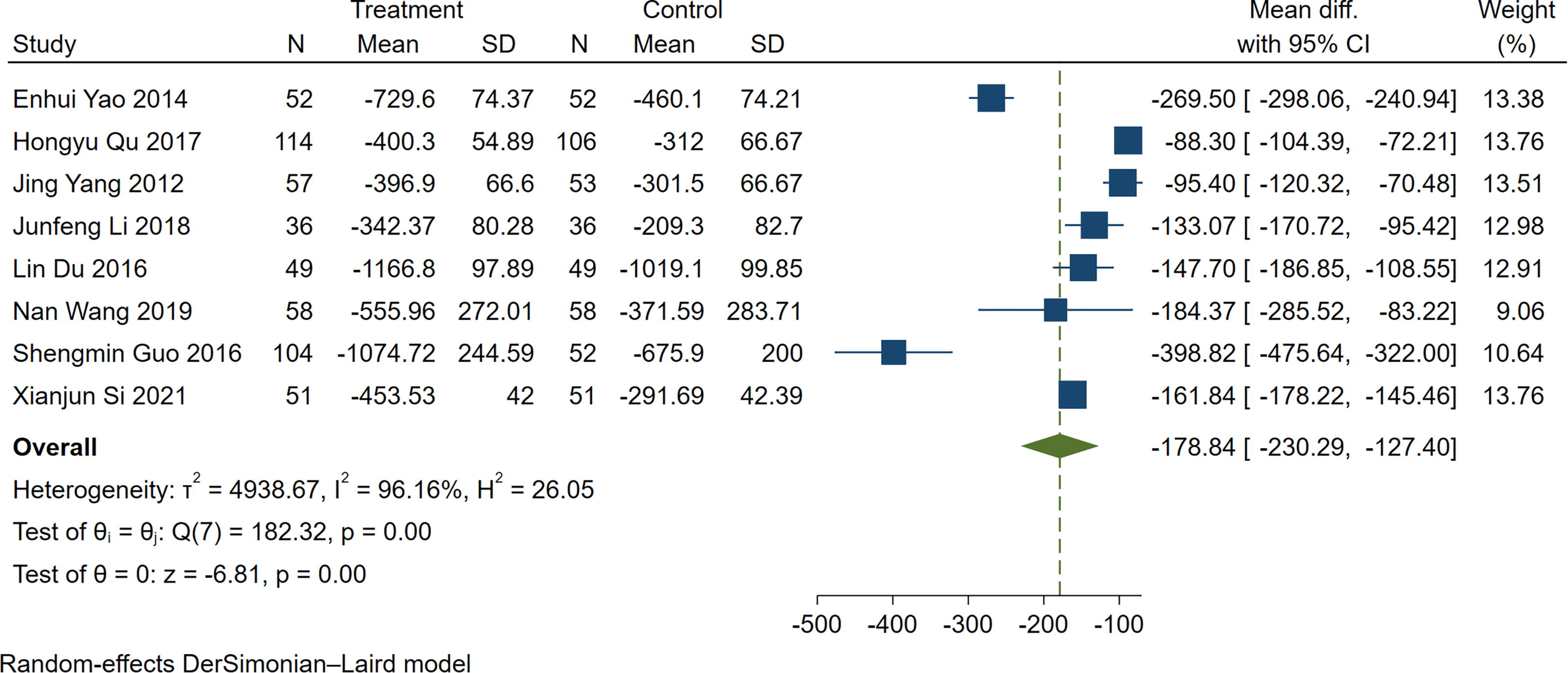
Forest plots for brain natriuretic peptide (BNP).
Subgroup Analysis of BNP
BNP, brain natriuretic peptide; CI, confidence interval; LVEF, left ventricular ejection fraction; MD, mean difference.
Nine studies explored the NT-proBNP levels in 915 patients. A random-effects model indicated a greater improvement in NT-proBNP levels in the XMLI group (MD = −490.95, 95% CI [−729.40, −252.50], Z = −4.04, p < 0.001) (Fig. 6). The heterogeneity test suggested significant heterogeneity (I 2 = 90.44%, p < 0.001). Subgroup analyses stratified by mean age, LVEF, treatment course, and sample size revealed no significant sources of heterogeneity (Table 5). Similarly, the sensitivity analysis showed no outliers (Supplementary Fig. S4).

Forest plot for N-terminal pro-brain natriuretic peptide (NT-proBNP).
Subgroup Analysis of NT-proBNP
CI, confidence interval; LVEF, left ventricular ejection fraction; MD, mean difference; NT-proBNP, N-terminal pro-brain natriuretic peptide.
6-min walking distance
Thirteen studies involving 1606 patients mentioned the 6-MWD. A random-effects model indicated that the XMLI group had a longer 6-MWD (MD = 44.01, 95% CI [28.63,59.38], Z = 5.61, p < 0.001) (Fig. 7). There was significant heterogeneity among the included studies (I 2 = 92.90%, p < 0.001). No sources of heterogeneity were identified in the subgroup analyses (Table 6). Sensitivity analysis revealed that there were no data outliers (Supplementary Fig. S5).

Forest plot for 6-min walking distance (6-MWD).
Subgroup Analysis of 6-MWD
6-MWD, 6-min walking distance; CI, confidence interval; LVEF, left ventricular ejection fraction; MD, mean difference.
Adverse reactions
Fifteen studies investigated adverse reactions, nine of which reported no adverse reactions. Six studies reported adverse reactions, including hepatic dysfunction, skin itching, palpitations, and other conditions (Supplementary Table S3). The incidences of adverse reactions were 1.9% and 1.3% in the XMLI and CWT groups, respectively. A random-effects model indicated no statistically significant difference in adverse reaction rates between the XMLI and CWT groups (RR = 1.47, 95% CI [0.73,2.99], Z = 1.08, p = 0.28) (Fig. 8). The studies showed no heterogeneity (I 2 = 0.00%, p = 0.99).

Forest plot for adverse reactions.
Publication bias
Funnel plots, including LVEF, LVEDD, and 6-MWD, were used to assess publication bias for the outcomes in more than 10 included studies (Supplementary Figs. S6–S8). Egger’s test showed that there was a publication bias for LVEF (p = 0.032), and no significant publication bias for LVEDD (p = 0.477) or 6-MWD (p = 0.946).
GRADE quality grading of evidence
The quality of evidence for all outcomes was assessed using GRADE. Adverse reactions were rated as moderate-quality evidence; LVEDD, BNP, NT-proBNP, and 6-MWD were classified as low-quality evidence; and LVEF was rated as very low-quality evidence. The results are presented in Supplementary Table S4.
Discussion
XMLI is a new national Class II drug with independent intellectual property rights for treating patients with CHF with qi and yang deficiency, as well as blood stasis. 36 Cluster and factor analysis of TCM patterns in 768 patients with CHF revealed qi deficiency, yang deficiency, and blood stasis as the primary syndromes. 37 This systematic review included 23 RCTs with 2643 patients, evaluating the efficacy and safety of XMLI for CHF treatment based on LVEF, LVEDD, BNP, NT-proBNP, 6-MWD, and adverse reactions.
The LVEF and LVEDD reflect systolic and diastolic cardiac functions, respectively. Based on the LVEF, CHF is classified into HF with reduced ejection fraction (HFrEF), HF with mildly reduced ejection fraction, and HF with preserved ejection fraction. 38 Studies have demonstrated that patients with HFrEF had a higher risk for cardiovascular mortality, rehospitalization, and sudden cardiac death. Prognosis improved significantly when the LVEF increased by ≥10% and exceeded 40%. 2 Adam et al. found that even slight increases in the LVEF (5% and 10%) correlate with significant improvements in quality of life. 39 The LVEDD reflects cardiac volume loading and is associated with cardiac remodeling. 40 Research indicated that LVEDD was negatively correlated with quality of life in patients with HF. 41 Our study showed that the combination of XMLI with CWT resulted in a 6.66% increase in LVEF and a 4.19 mm reduction in LVEDD compared with those under CWT alone, suggesting a potential improvement in prognosis and quality of life.
BNP and NT-proBNP are biochemical markers of CHF that are primarily produced by cardiomyocytes. Their levels increase when cardiomyocytes are subjected to stress, volume loading, and certain hormonal stimuli, reflecting the severity of HF. 42 The European Society of Cardiology uses BNP and NT-proBNP as exclusion criteria for CHF. 1 BNP and NT-proBNP reflect the prognosis of patients with CHF. A systematic review of 19 studies showed that each 100 ng/L increase in admission BNP levels was associated with a 35% higher relative all-cause mortality risk. 43 A study involving 7039 patients reported that a 1-unit increase in the log-transformed discharge BNP value was correlated with a 34% increased risk of 1-year mortality. 44 At discharge, patients with a <50% reduction in NT-proBNP had a 57% higher rehospitalization or death risk. 45 In a study of 599 patients with dyspnea, those with NT-proBNP levels of >986 pg/mL had a 2.88-fold higher mortality rate than did those with NT-proBNP levels of ≤986 pg/mL. 46 Our study suggested that, compared with CWT alone, the combination of XMLI and CWT reduced BNP and NT-proBNP levels by 178.84 and 490.95 ng/L, respectively, potentially improving prognosis and disease progression in patients with CHF.
The 6-min walk test is a simple and effective method for assessing cardiac function and activity capacity in patients with CHF. Patients walking ≤200 m had an approximately 20% higher all-cause mortality rate than those walking >200 m. A 25-m improvement in 6-MWD may be clinically significant, while a 50-m improvement may indicate a more improved health status. 47,48 In this study, the combination of XMLI and CWT increased the 6-MWD by 44.01 m compared with that under CWT alone, potentially improving patients’ health status.
Our study indicated that the incidence of adverse reactions was slightly higher in the XMLI group (1.9%) than in the CWT group (1.3%), but there was no statistically significant difference between the two groups. Adverse reactions associated with XMLI combined with CWT primarily included hepatic dysfunction, skin itching, palpitations, and headaches, whereas those in the CWT group primarily included headaches, hepatic dysfunction, and skin itching. No severe adverse events were observed in either group. The available evidence suggests that the combination of XMLI and CWT may be considered safe. However, owing to limitations in the reported adverse reaction data (e.g., 8 out of 23 studies did not assess safety outcomes), further research is required to confirm its safety profile.
The use of insect medicines has a long history worldwide. 49 In Brazil, ants are used to treat asthma, impotence, and arthritis, whereas in Japan, bees and their products aid in treating conditions such as freckles, hemorrhoids, and constipation. Because of their resilience and widespread presence, cockroaches have also garnered attention. 50 In Europe, cockroaches are used to treat strokes, and in South India, wine containing cockroach ashes is used to treat bladder stones. P. americana is a cockroach species considered significant in complementary and alternative medicine. TCM believes that P. americana invigorates blood and reduces swelling. 36 Modern research has revealed that P. americana extracts exert multicomponent, multitarget effects and are used to treat ulcerative colitis, cancer, wound healing, cardiovascular disease, and other conditions. 51 –54
With the advancements in modern scientific research methodologies and the refinement of evidence-based medical frameworks, the clinical value of herbal compound formulations and monomeric components in the prevention and treatment of cardiovascular diseases is garnering attention. Their multicomponent, multitarget regulatory networks have been progressively elucidated. 55 –61 XMLI, extracted from P. americana, was approved by the Chinese State Food and Drug Administration in 2006 for CHF treatment and exerts therapeutic effects on CHF through multiple mechanisms.
Ventricular remodeling is the core pathological mechanism underlying the onset and progression of CHF. When the heart suffers pathological injuries such as myocardial ischemia or pressure overload, the ventricles undergo adaptive changes in structure, morphology, and function. Although these changes transiently maintain cardiac output in the early stages, prolonged progression causes decompensatory alterations, including diminished myocardial contractility and reduced ventricular compliance, triggering a vicious HF cycle. Ventricular remodeling involves multiple pathological mechanisms, such as cardiomyocyte hypertrophy, myocardial fibrosis, inflammation, and oxidative stress. 62 –64 Excessive cardiomyocyte hypertrophy leads to energy metabolism disorders and contractile dysfunction. Previous studies have demonstrated that GATA binding protein 4 (GATA4), a key pro-hypertrophic transcription factor, can activate multiple HF-associated genes. 65 XMLI inhibits the phosphorylation of extracellular signal-regulated kinases 1 and 2 (ERK1/2), protein kinase B (AKT), and glycogen synthase kinase-3β, as well as suppresses the protein expression of GATA4, reversing cardiac structural remodeling and contractile dysfunction. 66 Cyclic guanosine monophosphate (cGMP), an intracellular second messenger molecule synthesized by guanylyl cyclase, regulates cellular growth, fibrosis, myocardial contraction, and cardiac remodeling through the activation of its downstream effector, cGMP-dependent protein kinase G (PKG). 67 Studies have shown that Sacubitril/valsartan can improve diastolic left ventricular stiffness by activating the cGMP-PKG signaling pathway and may serve as a therapeutic target for HF. 68 Similarly, XMLI regulates the cGMP-PKG pathway and improves myocardial fibrosis. 69 Autophagy, a lysosome-dependent process, degrades damaged organelles, misfolded proteins, and other harmful components to sustain cellular homeostasis and metabolic balance, playing a crucial role in myocardial fibrosis. 70 –72 XMLI can regulate autophagy and ameliorate cardiac fibrotic remodeling and LVEF by activating the phosphatidylinositol 3-kinase (PI3K)/AKT pathway and inhibiting the ERK1/2 and p38 mitogen-activated protein kinase signaling pathways. 73 Inflammation and oxidative stress contribute significantly to the pathogenesis and progression of CHF. 74 –76 XMLI reduces pro-inflammatory markers such as tumor necrosis factor-α and interleukin-6 and increases superoxide dismutase levels, inhibiting ventricular remodeling. 77,78 Additionally, XMLI can directly modulate Ca2+ channels to promote Ca2+ influx into cardiomyocytes, which is similar to the action of positive inotropic agents. 79 In summary, XMLI inhibits ventricular remodeling by regulating cardiomyocyte hypertrophy, myocardial fibrosis, inflammation, and oxidative stress and enhances myocardial contractile function by promoting Ca2+ influx, exerting therapeutic effects in CHF.
Strengths and Limitations
Our study suggests that the combination of XMLI and CWT effectively improves laboratory indices, cardiac function, and exercise tolerance in patients with CHF, potentially contributing to a better prognosis. Recent studies have demonstrated that XMLI combined with CWT has a satisfactory safety profile. This study provides new evidence-based support for XMLI as a complementary therapeutic option for patients with CHF. However, this study had some limitations.
First, the quality of the included studies was poor. Only 10 studies (43.4%) mentioned the randomization methods, 1 (4.34%) mentioned allocation concealment, 2 (8.69%) mentioned double blinding, and none mentioned blinded evaluation of personnel conducting statistical analyses, indicating a risk of selection bias. Second, the original studies did not comprehensively report the specific drug names or dosages used in the CWT. Third, heterogeneity persisted despite the subgroup analyses, possibly because of variations in the detection equipment and differences in CWT protocols. Fourth, Egger’s test suggested a publication bias in the LVEF results, possibly because studies with positive findings were more frequently published. Fifth, this study investigated the effect of combining XMLI with CWT on the prognosis of patients with CHF; however, the conclusions were based solely on clinical physicochemical indices without a direct analysis of rehospitalization or all-cause mortality rates.
Future studies should focus on the following aspects to further investigate the efficacy of XMLI in CHF. First, high-quality clinical trials should be conducted with a randomized, triple-blind, placebo-controlled design. Second, clinical trial reports should follow standardized protocols and provide detailed documentation of baseline characteristics, including specific medications and dosages used in CWT. Finally, in addition to existing outcome measures, prognostic indicators, such as rehospitalization rates, cardiovascular mortality, and all-cause mortality, should be evaluated.
Conclusions
This study demonstrates the efficacy and safety of combining XMLI with CWT for CHF treatment, providing an additional therapeutic option for patients with CHF. However, further high-quality clinical trials focusing on long-term prognoses are required to validate these findings.
Footnotes
Authors’ Contributions
S.-W.Z. conceptualized the study, searched and screened qualified studies, assessed the risk of bias, analyzed data, and drafted the article. J.-P.C. conceptualized the study, searched qualified studies, and drafted the article. H.-Q.Z. screened qualified studies, analyzed data, and visualized images. X.L. conceptualized the study, assessed the risk of bias, and corrected the article. H.-X.L. supervised the data search and analysis process and corrected the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (grant numbers: 82205098) and Scientific Research Program Project of Hebei Provincial Administration of Traditional Chinese Medicine (grant numbers: B2025055).
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.