
Abstract
Background:
Building on the 2017 Compendium of Health and Wellness Coaching (HWC) and its 2019 Addendum, the 2023 Addendum extends the scope of research by incorporating studies published from 2018 to 2022. This latest version continues to serve as a vital resource for practitioners and researchers, offering access to a comprehensive collection of studies spanning established and emerging health domains.
Methods:
The 2023 Addendum updates and expands the evidence base to evaluate HWC’s effectiveness across various conditions and settings. In this iteration, an expanded range of literature databases was explored to ensure inclusivity, categorizing articles into eight established health conditions—such as diabetes, heart disease, and obesity—while introducing two new categories reflecting research trends in respiratory conditions and chronic pain management.
Results:
The addendum includes findings from 212 articles, among which 115 randomized controlled trials (RCTs) demonstrate the effectiveness of HWC in improving patient-centered outcomes such as chronic care management, medication adherence, self-efficacy, and quality of life. Positive impacts were also documented on surrogate biomarkers, particularly in diabetes, hypertension, and cardiovascular care. All articles, including reviews and commentaries, are indexed with detailed methodologies and findings in an accessible spreadsheet format.
Conclusions:
Since its first iteration in 2017, the Compendium has grown to encompass over 480 articles, including more than 140 RCTs, illustrating the expanding role of HWC in health care. This evidence base underscores HWC’s utility as a key intervention for chronic disease management, preventive care, and whole-person health. Future research should focus on refining coaching methodologies, evaluating long-term outcomes, and exploring cost-effectiveness to enhance HWC’s delivery and impact across diverse populations and settings.
Introduction
Health and wellness coaching (HWC) employs evidence-informed tools and strategies to support individuals by enhancing understanding, developing skills, and fostering self-confidence in decision-making, thereby facilitating long-term behavioral changes that reduce morbidity linked to lifestyle-related conditions. 1 –6 HWC professionals partner and collaborate with other health care professionals to help patients identify, enact, and/or improve behavioral changes that would positively impact behavioral-centered outcomes (e.g., readiness for change, lifestyle changes, treatment adherence) and health care outcomes (e.g., quality of life, mental well-being, disease-relevant surrogate markers, and clinical measures). 7 –12 HWC has shown a significant impact in increasing the clinical benefit of standard-of-care and companion modalities, including remote monitoring, health education (e.g., cardiometabolic risks, culinary medicine), 13 and food programs (e.g., meal replacements, whole food prescriptions). 14 –18
Within the past decade, the field of HWC has seen a surge in scholarly and research attention, with a projected 18% increase in employment opportunities expected between 2020 and 2030. 1,19 Since 2017, the National Board for Health & Wellness Coaching (NBHWC) 20 and the National Board for Medical Examiners 21 introduced the first national board certification examination, setting high standards for training, assessment, and credentialing. The 2017 HWC Compendium 22 and its 2019 addendum 23 synthesized 18 years of HWC research, reflecting the field’s growing scholarly interest. In 2019, NBHWC and the Department of Veteran Affairs secured Category III Current Procedural Terminology (CPT) codes for HWC, crucial for the American Medical Association (AMA) approval of Category I codes. 24 In 2024, the Center for Medicare and Medicaid Service (CMS) added HWC CPT codes to the Medicare Telehealth List. 25 Notably, CMS requested, “In future evidence submissions, we would expect to see peer-reviewed literature, where the study population is typical of the Medicare population (for example, specific age bands in study populations), and the methods focus on evaluating utilization and outcomes (for example, claims data and analysis that includes the specific codes at issue).” The CMS request signals a pathway for advancing practice-based research studies and standardized HWC interventions as standard-of-care health care services, necessitating ongoing tracking of clinical and self-reported outcomes.
As the field increasingly aligns with scientific research, evidence-based practice, and documented service use, our team of researchers from the Mayo Clinic and the NBHWC has compiled 3 years of HWC literature. The aim of the 2023 Addendum is to update the 2017 HWC Compendium and 2019 Addendum to provide systematically researched and compiled discoveries that can aid HWC educators, researchers, and practitioners in accessing up-to-date knowledge and gaps to inform the continuous advancement of the HWC field.
Methods
The full detailed methodology is included in Supplementary Appendix. The 2023 Addendum was produced using methods that align with the 2017 HWC Compendium 22 and its 2019 Addendum. 23 The literature for the current addendum, with a legend of coding systems for article descriptions, is detailed in the Supplementary Data Repository in the Supplementary Appendix.
Notably, while a compendium methodically searches and compiles a concise collection and summary of a specific area, it does not statistically analyze data, nor does it specifically address study-based biases—the function of systematic reviews and meta-analyses. Ongoing efforts and forthcoming systematic reviews will methodologically synthesize, analyze, critically appraise, and interpret available data to inform future guidelines and recommendations.
Search strategy
A search was conducted by the senior authors of the compendium (A.M.A.D., J.M.W., G.A.S.) in collaboration with the medical librarian (T.J.B.). The comprehensive bibliographic search utilized multiple databases and search engines with dates ranging from January 1, 2005, to March 31, 2022, for English language citations. The detailed search strategy is shown in Supplementary Appendix.
Definition and criteria of HWC
We adapted the earlier HWC definition in line with the 2017 Compendium and NBHWC standards. 2 This allowed us to ascertain four HWC constructs for our inclusion criteria: (1) training (i.e., the health and wellness coach used behavior change theory and coaching processes), (2) patient-centered goal setting (i.e., the patient partially or wholly determined behavior change or health goals), (3) accountability (enacting a form of check-in and tracked progress), and (4) patient-coach continuity relationship (i.e., objectively defined by at least three coaching sessions with the same coach and client to establish rapport and engage in coaching processes).
Included studies
We included studies that featured coaching interventions that met the definition and criteria of HWC. We included original data-based (i.e., investigational) studies of any design (i.e., observational and interventional, comparative and noncomparative, systematic reviews and meta-analysis, state-of-the-art reviews) encompassing patients of any age, health status, type of HWC delivery modality (i.e., in-person, virtual/telemedicine, audio-only/phone), and in any setting. We also included other scholarly non-data-based article categories, including detailed commentaries, summary (nonsystematic) reviews, and program descriptions. We excluded short communications, letters, perspectives, and viewpoint articles.
Outcomes of interest
Outcomes of interest included patient-related biometric or psychometric outcomes relevant to health and wellness goals and processes. These outcomes included health-care-specific outcomes, quality of life, and daily lifestyle wellness goals, such as clinical improvements or worsening symptoms, surrogate biomarkers, quality of life, and functional outcomes (e.g., functional independence and care burden) and social isolation.
Results
Summary reporting
The search strategy for the 2023 Addendum identified 6325 articles, with 212 articles meeting the final eligibility criteria. The Supplementary Data Repository in the Supplementary Appendix details baseline characteristics for each included study, and Supplementary Figure SA1 in Supplementary Appendix is a flowchart of study selection. The 2023 Addendum revealed 115 randomized controlled trials (RCTs), indicating a noticeable increase in comparative research in Table 1 across the years, as summarized per condition. Additionally, there was a rise in qualitative studies, contextualizing the understanding of HWC feasibility, acceptance, and impact. Most studies reported follow-up outcomes of 12 months or shorter. The current literature is categorized into eight established conditions, in line with the earlier compendium and addendum: diabetes, obesity, heart disease, hypertension, cholesterol, cancer, wellness, and miscellaneous. Emerging categories included respiratory conditions and chronic pain management, reflecting the expanding role of HWC in addressing specific health care and well-being needs.
Summary of Number of Health and Wellness Coaching Original Data-Based Articles (2017, 2019, 2023)
Some of the mixed-methods studies may fall in more than one category (i.e., R and NR5). Non-data-based studies are not included in this count.
NR5, nonrandomized before–after studies; NR9, qualitative studies; other, all other; R, randomized controlled studies.
Diabetes and obesity management remained the most extensively studied conditions, while the wellness category showed a surprising decrease in studies in comparison with the earlier compendium and addendum. Notably, there was a considerable increase in HWC research focusing on underserved populations and technology-assisted interventions. Figure 1 illustrates the types and categories of included articles.
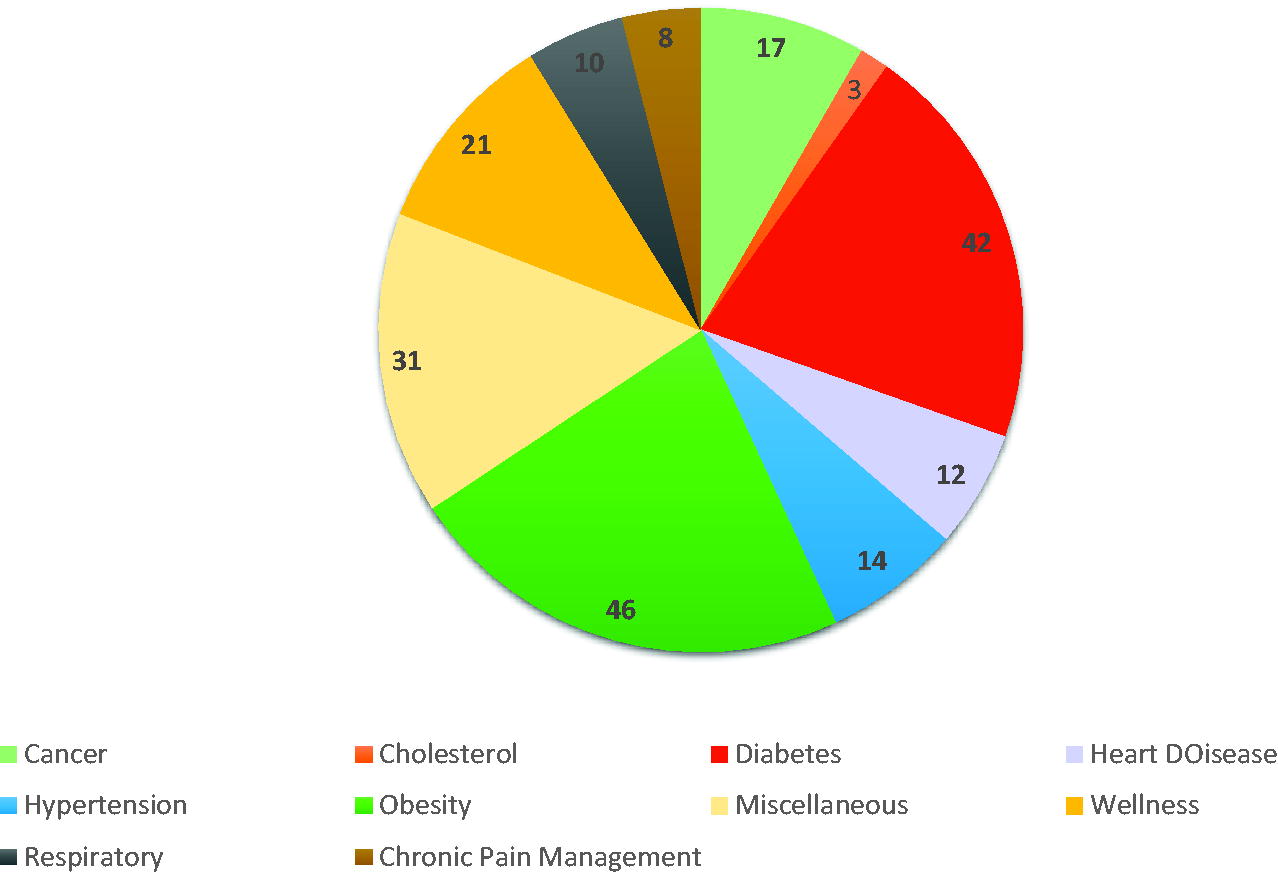
Original data-based studies in the 2023 Addendum to Compendium of Health and Wellness Coaching Literature.
An in-depth analysis of overall findings per category is summarized in Supplementary Appendix, while Supplementary Table SA1 in Supplementary Appendix provides a comparative analysis of findings from the 2017 Compendium and 2019 and 2023 addenda per condition/category. Here, we summarize the findings of the 2023 Addendum by category and condition.
Established conditions
Diabetes
The 2017 Compendium and 2019 Addendum featured 62 journal articles related to the effects of HWC in diabetes management, including 18 RCTs. The 2023 Addendum adds 46 new journal articles, including 44 original data-based (investigational) research studies and 4 other non-data-based scholarly (opinion, commentary) articles. Notably, this search uncovered 10 peer-reviewed studies predating 2018 that were not included in the earlier publications. Of the 44 original research studies, 21 were quantitative, 12 used mixed methods, 4 were qualitative, and 1 was a quality improvement study. Of these 42 studies, there were 28 RCTs (including 7 published before 2018), 8 pre–post pilot studies, 1 cohort study, 1 case series, 2 qualitative studies, and 1 quality improvement study. This trend of increasing RCTs may highlight a shift in conducting more rigorous and evidence-based HWC research.
The sample sizes were highly variable, ranging from 10 to 4156 participants. Interventions for diabetes ranged in duration from 1 to 48 months (mean 8.5 months), with coaching interventions averaging 13.4 months. Virtual coaching has become more prevalent, with only 33% of post-2018 studies using in-person or hybrid modalities compared to all studies prior to 2018. Outcomes across these studies were promising: 79% of those measuring glycated hemoglobin A1c reported decreases (i.e., positive change), particularly among RCTs, with additional impact, including improved lifestyle modification, medication adherence, and mental health indicators.
Obesity
The 2017 Compendium and 2019 Addendum featured 62 articles related to the effects of HWC on obesity, including 23 RCTs. The 2023 Addendum adds 47 articles: 46 original data-based (investigational) research studies (24 RCTs, 16 cohorts, and 6 other observational studies) and one summary review. Of the 46 original studies, 37 were quantitative and 9 used mixed methods.
The sample sizes were highly variable, ranging from 11 to 13,178 (mean of 2125) participants due to two large cohort studies, though RCTs averaged around 201 participants. HWC interventions spanned 2–36 months and included between 6 and 46 sessions. Positive outcomes were observed in 81.8% of studies for body weight and body mass index reduction, and additional benefits were noted in areas such as nutrition, physical activity, and mental health. These findings support the feasibility and efficacy of HWC in weight management, with virtual coaching becoming the more common delivery mode.
Heart disease
The 2017 Compendium and 2019 Addendum featured 20 articles, including 13 RCTs related to heart disease and HWC. The 2023 Addendum adds 12 original data-based (investigational) research studies, with 11 quantitative designs (11 RCTs) and 1 quality improvement study addressing both preventive and therapeutic outcomes for various cardiovascular diseases and heart conditions.
The sample sizes ranged from 42 to 1533 participants. Coaching interventions for heart disease typically ranged from 3 to 12 months, averaging 6.8 sessions, and utilized a variety of delivery methods, including telehealth. Studies reported improvements in clinical markers such as hemoglobin A1c, lipid profiles, weight, and mental health. Additionally, some studies highlighted the potential financial benefits of HWC for cardiovascular health, including one longitudinal case–control study measuring reductions in mortality and health care costs across 6 years. These results underscore HWC’s value in heart disease management, particularly in cardiometabolic risk reduction.
Hypertension
The 2017 Compendium and 2019 Addendum featured 34 articles, including 9 RCTs related to hypertension and HWC. The 2023 Addendum adds 14 original data-based (investigational) research studies (7 RCTs, 2 pre–post pilot trials, 2 cohort studies, 1 quasi-experimental trial, and 2 qualitative studies). The sample sizes ranged from 9 to 373 participants. Coaching interventions for hypertension ranged from 1 to 3 months and included 3 to 12 sessions, with telehealth being a frequently used delivery method in recent years. While all studies reported improved outcomes in blood pressure management, medication adherence, and lifestyle improvements, some studies did not reach statistical significance despite reported improvement. High levels of participant engagement and perceived improvements in blood pressure control indicate the positive impact of HWC for hypertension.
Cholesterol
The 2017 Compendium and 2019 Addendum featured 21 articles, including 11 RCTs addressing cholesterol management and HWC. The 2023 Addendum adds only three original data-based (investigational) quantitative research studies solely focused on cholesterol management and other cardiovascular disease risk factors. These three quantitative studies included two pre–post pilot studies and one retrospective cohort study. Sample sizes ranged from 81 to 326 participants, with coaching interventions lasting 6–12 months and comprising 3–12 sessions. Two studies were conducted in person, while one used a phone-based format. Across these studies, reductions in low-density lipoprotein cholesterol, total cholesterol, and blood pressure were reported, alongside increased participant satisfaction. Higher engagement levels were also associated with improved lipid profiles, underscoring HWC’s value in cholesterol management.
Cancer
The 2017 Compendium and 2019 Addendum featured 10 original data-based (investigational) research articles, including 8 RCTs related to HWC and cancer. The 2023 Addendum adds 19 articles, including 17 original research articles (6 RCTs, 5 pre–post pilot trials, 3 cohort studies, and 3 qualitative studies).
The sample sizes ranged from 13 to 786 participants. The duration of coaching interventions varied, ranging from 1 to 6 months with 3 to 12 sessions. Delivery methods were diverse, with both in-person and remote approaches used. The studies reported numerous benefits, including improvements in physical activity, quality of life, and dietary habits. Many participants, particularly those with breast cancer, noted enhanced well-being and reduced distress, and one study reported a positive impact on return-to-work rates postcancer treatment. These findings suggest that HWC can provide meaningful support to cancer patients by improving quality of life and promoting healthy lifestyle choices.
Wellness
The 2017 Compendium and 2019 Addendum featured 58 original data-based (investigational) research articles related to HWC and wellness, including 21 RCTs. The 2023 Addendum adds 22 wellness-focused articles, including 21 original research studies and 1 scholarly article. Of the 21 data-based studies, 14 were quantitative and 7 used mixed methods. Notably, the 21 studies included 12 RCTs, 2 pre–post pilot studies, 6 cohort studies, and 1 qualitative study.
Studies ranged in sample size from 50 to 1264 participants. Participants were primarily middle-aged, educated, and female. The duration of coaching programs varied from 3 to 12 months, with 4 to 24 sessions. Studies reported positive perceptions of HWC, with some studies showing a significant association with cost reduction, particularly in minority-focused programs. Participants commonly reported improvements in physical activity, dietary habits, and psychological well-being, although some studies showed mixed results. Overall, the 2023 Addendum broadens the scope of wellness studies and highlights HWC’s feasibility and effectiveness in promoting behavior change and well-being.
Miscellaneous
The 2019 Addendum featured 9 original data-based (investigational) research articles, including 5 RCTs related to miscellaneous categories. The 2023 Addendum adds 31 original research articles that do not fit singularly into other categories. Of these, 18 were quantitative studies, 7 used mixed methods, and 3 were qualitative. Of the original studies, 20 were RCTs, 5 were cohort studies, 2 were case series, and 1 was a qualitative study. Coaching interventions lasted from 2 to 12 months and varied in delivery methods, including online, mobile health, telephonic, and in-person sessions. These studies addressed diverse health outcomes, such as stroke, kidney disease, chronic disease management, quality of work life, resilience, preventive care, periconception, and pregnancy.
Examples of findings include improved health care activation among rural Zuni participants with chronic kidney disease, enhanced quality of work life for administrators, increased resilience among sixth-grade students, and better lifestyle behaviors to reduce stroke risk. Gestational-related studies highlighted the feasibility, efficacy, and satisfaction with HWC during periconception and pregnancy, leading to improved nutritional habits and postpartum weight loss. Although some studies did not show significant effects on morbidity/mortality or hospitalizations, a 9-month disease prevention program significantly improved health biomarkers and reduced chronic disease risk among employees. Overall, studies in the “Miscellaneous” section report positive outcomes for HWC interventions across diverse conditions and populations.
Emerging categories
Two specific conditions were previously addressed as part of the miscellaneous section: respiratory diseases and chronic pain. There has been substantial growth in research focusing on these conditions; therefore, we report these emerging conditions in their own categories.
Respiratory disease
The 2023 Addendum introduces 10 original data-based (investigational) research studies on the efficacy of HWC for managing respiratory conditions, specifically chronic obstructive pulmonary disease (COPD). Of these studies, seven employed mixed methods, and three were quantitative, with designs including five RCTs, two cohort studies, two case–control studies, and one cross-sectional study. Across the studies, a total of 1556 patients with COPD were recruited.
Coaching interventions generally showed positive outcomes, particularly in long-term COPD management by enhancing self-management behaviors and inhaler adherence. Several studies indicated a reduction in COPD-related hospitalizations, suggesting HWC’s potential in minimizing disease exacerbations and lowering health care utilization. The effect on quality of life varied across studies, yet improvements in mental health outcomes, such as depression, were consistently noted.
Notably, home-based HWC programs proved to be feasible and highly acceptable, with high adherence levels reported among COPD patients, underscoring their suitability for diverse patient demographics. Specific findings include greater medication adherence and inhaler use, 26 enhanced self-management skills in home-based programs, 27 and increased physical activity, as evidenced by step counts in a goal-setting cohort. 28 HWC improved quality of care scores and reductions in depression symptoms, with a trend toward fewer hospitalizations, 29 but a study found no significant difference in health-related quality of life, though it noted an increase in self-management engagement among coached patients. 30 Integrating specialist coaching significantly improved guideline-concordant care and patient-reported quality of care, with evidence on the benefits of subspecialized training for coaches. 31
Together, these findings underscore HWC’s multifaceted impact on respiratory disease management. While improvements in clinical metrics such as medication adherence and self-management were frequently observed, HWC’s broader influence extended to enhanced patient engagement and perceived quality of care, reflecting its value in holistic COPD management.
Chronic pain management
The 2023 Addendum includes 8 original data-based (investigational) research studies examining the efficacy of HWC interventions in managing chronic pain conditions, mainly knee osteoarthritis, low back pain, and nonspecific low back pain, across 1279 participants, with intervention periods ranging from 8 weeks to 24 months. Multimodal interventions—included health education, exercise programs, physiotherapy sessions, and/or self-management techniques in addition to HWC—were delivered through individualized sessions, telephone coaching, face-to-face consultations, and/or home-based programs.
Three studies focused on knee osteoarthritis. Gilbert et al. 32 used motivational interviewing, leading to increased physical activity levels. Williams et al. 33 implemented a self-determination theory-based intervention, significantly increasing physical activity among patients. O’Brien et al. 34 targeted weight loss and physical activity, increasing physical activity despite minimal changes in pain and disability.
Three studies focused on low back pain/nonspecific low back pain. Gardner et al. 35 showed significant reductions in pain and disability scores over 12 months, improving overall well-being and functional abilities. Thanawat and Nualnetr 36 used health education and exercises for low back pain management, resulting in significant pain and function improvements over 8 months. Iles et al. 37 integrated HWC into physiotherapy, significantly improving functional status over 12 weeks. Two other studies where one focused on general pain management and one on fibromyalgia management. Hinman et al. 38 implemented a physiotherapist-led intervention, resulting in pain reductions and physical function improvements at 6 months, sustaining active lifestyles at 12 months. Hackshaw et al. 39 evaluated an HWC intervention for fibromyalgia, demonstrating significant enhancements in health and quality of life, reduced pain severity, and notable reductions in health care utilization.
HWC interventions for chronic pain showed benefits such as reduced pain, improved physical activity, and enhanced functional abilities. Quality-of-life improvements were notable, particularly in fibromyalgia and knee osteoarthritis. The studies supported the feasibility of integrating HWC into multimodal approaches but highlighted the need for further research to address variability and optimize long-term outcomes.
Discussion
Integrated summary of findings
The 2023 Addendum builds on the foundational work of its 2017 and 2019 predecessors, providing a comprehensive understanding of HWC’s effectiveness in eight established health conditions and two emerging categories across various health care and wellness settings. The summarized knowledge from 212 articles, including 108 RCTs, indicates that HWC interventions are impactful in managing chronic health conditions and improving lifestyle behaviors. For all previously reported conditions (diabetes, obesity, heart disease, hypertension, obesity, cancer, and wellness) as well as two emerging conditions (respiratory diseases and chronic pain management), studies integrating HWC generally demonstrated positive effects on patient-centered and patient-reported outcomes, including self-efficacy, quality of life, disease management, and medication adherence. HWC also supported improvements in health biomarkers, including blood glucose, blood pressure, cholesterol levels, physical activity, and dietary habits. Despite some inconsistencies and limitations, including variable study designs and small sample sizes in interventional studies, these findings suggest that HWC is an acceptable, feasible, and effective intervention for improving clinical, surrogate, self-care outcomes, and quality of life-related outcomes. Further research is needed to optimize coaching methodology (dosing and framework), understand long-term effects, and explore cost-effectiveness to enhance HWC delivery and impact across diverse health care settings and populations.
Comparative analysis of HWC effectiveness
This addendum compiles HWC publications through March 2022, comparing findings to seminal studies and recent reviews through March 2024. 3,9,11,40 –43 By doing so, it provides a nuanced, comprehensive view of HWC’s growth, utilization, adaptability, efficacy, challenges, and opportunities. 3,6,7,9 –12,15,40,42 –47 The differential effectiveness of in-person versus digital HWC delivery methods remains an area of exploration. Mills et al. demonstrated significant reductions in blood pressure through multilevel, multicomponent interventions that included in-person HWC. 3 These effects may be attributed as much to the program’s complexity as to the coaching modality. Conversely, Bevilacqua et al. found digital HWC effective for weight loss and waist circumference but noted challenges in sustaining long-term behavior change, particularly for clinical outcomes such as blood pressure. 42 Chew et al. emphasized the potential of hybrid models integrating digital tools with personalized coaching to improve engagement and adherence. 45 Caution is warranted when interpreting digital HWC findings due to variations in program design, outcomes measured, and participant characteristics, underscoring the need for rigorous comparative studies. 42,43,46
Several studies explored the effectiveness of HWC as a standalone intervention versus as part of a broader, multimodal approach. Sieczkowska et al. evaluated HWC for weight loss, reporting positive effects despite limitations in methodology and risk of bias. 43 Conversely, interventions incorporating HWC alongside self-monitoring tools, medication adherence strategies, or lifestyle programs demonstrated broader impacts. For example, Racey et al. highlighted the short-term benefits of HWC for diabetes management while emphasizing the need for booster doses to sustain outcomes. 10 These findings align with earlier research emphasizing the critical need for well-designed studies that can isolate the effects of HWC within multicomponent programs. 40,42,47
Despite progress, significant opportunities remain to improve diversity and representation in HWC research. Over 20 studies in this review examined ethnoracially and resource-diverse populations, providing valuable insights. 48 However, challenges persist in ensuring generalizability across diverse demographic and socioeconomic contexts. To address this, future research must prioritize equitable representation and compare outcomes among varying populations, thereby enriching the evidence base and ensuring HWC’s accessibility and relevance.
While these studies show consistent evidence of the acceptability and feasibility of HWC, they also reveal heterogeneity in design and outcomes, complicating cross-study comparisons. For example, Boehmer et al. reported improvements in self-management among patients with COPD, 40 while Prior et al. noted significant reductions in pain and disability in chronic pain populations. 47 These findings, along with insights from systematic reviews, 3,6,7,9 –12,15,40 ,42 –45,47,49 –51 highlight the promise of HWC as a critical tool in chronic disease management. However, sustaining behavior change through HWC remains complex, requiring innovative approaches and rigorous research to optimize delivery frameworks and maximize impact. 10,52 –54
Supplementary Table SA2 in Supplementary Appendix summarizes recent comparative effectiveness reviews across health conditions from selected systematic reviews with or without meta-analysis. 3,6,7,9 –12,15,40,42 –45,47,49 –51
The evolving landscape of HWC and its implications
The past 5 years have seen considerable advancements in HWC, supported by national advocacy and technological innovations. 1,20,24 The integration of in-person and telehealth methods and remote health applications has made HWC more feasible and acceptable, enabling real-time health monitoring and improved communication between coaches and clients. This digital shift has expanded HWC’s accessibility and allowed for more personalized, data-driven strategies. 46 HWC has also been integrated into various health care settings, addressing conditions such as respiratory disease, chronic pain, and musculoskeletal issues. 7,11,40,47 HWC is recognized as a valuable tool in primary care for preventive health and chronic disease management. Mental health services have started incorporating wellness coaching, particularly for anxiety and depression, although rigorous studies are scarce. Employers are adopting HWC in wellness programs to enhance employee well-being and productivity, yet studies on HWC services delivered by health insurance sectors are notably lacking. 55 –58 These developments highlight the growing impact of HWC in promoting whole-person health. 59,60
Limitations, opportunities, and the future of HWC
In summarizing this addendum, we compile our findings from a search date inclusion through March 2022 while also comparing findings from more recent evidence-based systematic reviews published through March 2024 (i.e., beyond the cutoff search point for the compendium). This approach aims to bridge gaps, identify consistent trends, and highlight areas needing further exploration, enhancing the evolving application of HWC in practice and research. The field of HWC has experienced substantial growth, supported by its role in promoting patient-centered outcomes across diverse health conditions. Challenges such as variability in HWC interventions, including duration (ranging from 1 to 48 months), frequency (3 to 48 sessions), and methodologies, continue to limit the ease of summarization and interpretation. 1,52 Standardized protocols and guidelines are essential to ensure consistency and quality in HWC practices. Combining HWC with other interventions, such as education or counseling, or as part of an integrated team structure presents opportunities for improved outcomes, but also complicates the interpretation of individual intervention efficacy. Precision in study designs and analysis can help clarify these effects where applicable. 52
The emergence of the COVID-19 pandemic posed unique limitations, especially in its early stages, as it universally impacted research endeavors. The pandemic’s effect on global health and economic systems introduced variables that added complexity to interpreting HWC outcomes, underscoring the need for carefully designed studies. 61 Researchers faced challenges such as adapting to remote delivery methods, maintaining participant engagement and retention in virtual settings, and addressing the escalating complexity of mental health issues. Nonetheless, the pandemic accelerated the adoption of telehealth and digital platforms, offering new opportunities to study the accessibility, effectiveness, and equity of different HWC delivery modalities. 42,46 Research suggests promising outcomes with digital HWC, with several studies reporting comparable or improved accessibility and reach compared to in-person interventions. Additionally, the shift toward stress management in the wake of heightened societal stressors reflects the growing role of HWC in addressing social determinants of health. 62,63
Evolving and emerging opportunities
As HWC continues to evolve, several emerging areas of impact merit attention, including digital health interventions, neuroscientific insights, cultural competency, and a whole-person approach to well-being. Condition-based subspecialty training as well as dissemination and implementation frameworks (e.g., methods, dosing) are needed to support HWC’s integration into clinical practice. 1,31,49,52 Sustainable reimbursement will require robust clinical evidence for different conditions, particularly through CPT-coded hybrid service-delivery models. 64 Expanding research on demographic diversity, 65 the long-term (>1 year) maintenance of impact across diverse conditions, 49 and the integration of digital health tools, particularly AI, could further enhance its effectiveness. Additionally, broadening HWC’s role in global health, community outreach, and crisis response is essential for increased applicability and impact. 61 We summarize some of these key areas in Table 2.
Comparative Effectiveness Evidence Across Health Conditions from Selected Systematic Reviews with or Without Meta-Analysis
AMA, American Medical Association; CMS, Center for Medicare and Medicaid Service; CPT, Current Procedural Terminology; HWC, health and wellness coaching; NBC-HWC, National Board Certified Health & Wellness Coach.
The future of the HWC compendium
The establishment of a national board (NBHWC) offering certification and the recognition of reimbursement CPT codes by the AMA are clear indications of HWC’s emergence as a vital health care profession. The HWC Compendium has played a supportive role in these developments and has advocated for systematic reviews and meta-analyses to delve deeper into HWC effectiveness. Since the inception of the HWC Compendium in 2016, the field of HWC has matured considerably. Notably, the 2023 Addendum alone witnessed the publication of over 10 systematic reviews with or without meta-analysis, 6,7,10,11,15,40,42 –47,59 reflecting the field’s evolution and remarkable growth, albeit without clear implementation of the adapted HWC definition by Wolever et al. 2 With the increasing publication of evidence-based reviews as well as current advancements in technology (e.g., artificial intelligence) and search engines, we envision the future compendium to become a living compendium (i.e., direct online study repository updates) as a more efficient and appropriate to field’s mission.
Conclusions
The 2023 Addendum highlights the recognizable growth in the body of literature and the extent of HWC applications, achieved since its 2017 and 2019 predecessors, with over 480 articles and 160 RCTs included from all versions. This cumulative evidence across the past two decades underscores the growing role of HWC, particularly in chronic conditions management and in improving patient-centered and -reported outcomes. As the field of HWC continues to evolve through standardized methodologies of education, training, research, and practice supported by advancing technologies, it is poised to expand further in health care settings and beyond, reinforcing its role in comprehensive well-being, preventive health, and tertiary care management.
Footnotes
Acknowledgment
The Scientific Publications staff at Mayo Clinic provided copyediting, proofreading, administrative, and clerical support.
The staff at the National Board for Health & Wellness Coaching, specially Ms. Cindy Romero, for facilitating the administrative work.
Authors’ Contributions
Conceptualization: A.M.A.D., J.M.W., M.M., and G.A.S. Data curation: A.M.A.D., J.M.W., B.M., R.G., A.B.M., A.R., S.N.P., T.J.B., and G.A.S. Formal analysis: A.M.A.D., J.M.W., B.M., M.P.K., K.S., E.S., S.H., R.G., A.B.M., A.R., S.N.P., B.M.B., and G.A.S. Investigation: A.M.A.D., J.M.W., and G.A.S. Methodology: A.M.A.D., J.M.W., B.M.B., M.M., T.J.B., and G.A.S. Project administration: A.M.A.D., J.M.W., A.B.M., and G.A.S. Resources: A.M.A.D., J.M.W., A.B.M., M.M., and G.A.S. Supervision: A.M.A.D., J.M.W., and G.A.S. Validation: A.M.A.D., J.M.W., M.M., and G.A.S. Visualization: A.M.A.D., J.M.W., M.M., and G.A.S. Writing: A.M.A.D., J.M.W., B.M., M.P.K., K.S., E.S., S.H., B.M.B., and G.A.S. Critical review: A.M.A.D., J.M.W., A.B.M., M.M., T.J.B., and G.A.S.
Author Disclosure Statement
A.M.A.D. is a board member (volunteer) at the National Board for Health & Wellness Coaching. J.M.W. is a board member (volunteer) at the National Board for Health & Wellness Coaching. B.M.B. is a member of the National Board for Health & Wellness Coaching and the UH Integrative Health and Well-Being Coaching Program. G.A.S. is a member of the National Board for Health & Wellness Coaching Research Commission and a research advisor to Wellcoaches. The other authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.
Supplementary Materials
Supplementary Appendix
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.