
Abstract
Objective:
Owing to perceived additional costs, patients may avoid integrative health and medicine (IHM) treatments, while insurers may not cover IHM. We hypothesized that adult beneficiaries of a health system’s employee insurance plan with musculoskeletal (MSK) conditions receiving covered outpatient IHM would have reduced total allowed costs over the 1-year follow-up compared with matched controls, secondarily exploring medical and pharmaceutical cost subsets.
Methods:
We queried medical records and claims spanning 2018–2023 for beneficiaries aged 18–89 years with a new MSK episode. Patients were divided into cohorts: (1) IHM within 3 months after MSK diagnosis and (2) no IHM after initial primary care. After inflation adjustment and trimming, propensity score matching was used to balance cohorts on demographics, comorbidity, health care utilization, and prior 12-month spend. Least-squares mean total, medical, and pharmaceutical allowed costs (United States Dollar) over the 1-year follow-up were analyzed using a linear mixed model. Findings were compared with a generalized linear model without trimming.
Results:
There were 251 patients per matched cohort, with adequate covariate balance. There was no meaningful between-cohort difference (IHM minus No IHM) in least-squares mean total cost (+703 [95% CI: −314, 1720]). Secondary outcomes included medical cost (+878 [95% CI: 61, 1695]) and pharmaceutical cost (+6 [95% CI: −71, 83]). A generalized linear model revealed no meaningful difference in estimated mean total medical costs (−2561 [95% CI: −7346, +2224]).
Conclusions:
IHM use among adult health system beneficiaries with MSK conditions was not associated with meaningful differences in 1-year follow-up total health care costs compared with matched controls. Our study was underpowered for secondary outcomes, which should be interpreted with caution. Future research should include a larger sample of patients and examine longitudinal changes in patient-reported outcomes.
Introduction
Musculoskeletal (MSK) disorders are highly prevalent in the United States (US) and are associated with increased disability, health care utilization, and health care–related costs when compared with other conditions. 1 Integrative health and medicine (IHM), including acupuncture and chiropractic, offer foreseeable benefits for patients dealing with MSK disorders such as back or neck pain, with few adverse effects. 2 Despite its potential advantages, IHM adoption remains limited. Based on an analysis of the US 2019 National Health Interview Survey, merely 20% of adults experiencing low back or neck pain had engaged with IHM during the previous 12 months. 3 In a recent systematic review (2020) which examined factors influencing IHM use, nearly half of publications from Western populations cited “high cost” as a deterrent to using IHM. 4 These perceptions can be a barrier to care—hindering insurance coverage and potentially limiting accessibility. 5 –7
In addition, IHM coverage is inconsistent across health insurance carriers. 5 –7 For example, only 50% of US acupuncture visits were covered by a health insurance carrier in 2019. 5 While chiropractic is covered by most insurers, the coverage may be incomplete, especially for governmental plans. 6,7 As indicated by senior insurance executives, variable coverage of IHM can in part be attributed to apprehensions surrounding increased expenses. 6 Variable insurance coverage may also relate to a disparity in care access, whereby patients with lower income may be less likely to use IHM for chronic pain or arthritis. 8 –10
However, clarifying the cost implications of IHM has been a challenge, with limited research on the topic yielding conflicting results. 11,12 These divergent findings may be attributed to the heterogeneous impact of IHM on care pathways. For example, visiting a IHM clinician for a new MSK disorder is associated with a reduced likelihood of receiving prescription medications (i.e., opioids, benzodiazepines, or gabapentin), attending specialist visits, or undergoing procedures (i.e., epidural steroid injection or spinal surgery) for these conditions compared with usual medical care. 13 –19 Conversely, IHM treatments may require multiple visits, which could therefore increase total and medical health care costs when used in a complementary manner to usual medical care. 20,21 Adding to the complexity, prior studies have been confounded by an inability to account for out-of-pocket expenses due to inconsistent IHM coverage. 11,20 Our current study offers a unique opportunity to address these limitations by examining the cost of IHM services within an employee health plan in which IHM is covered.
Due to the limited understanding of the impact of IHM coverage on health care cost, this study compared costs between IHM users and nonusers among beneficiaries of a health system’s insurance plan that covered IHM modalities. Based on previous literature showing a reduction in health service utilization with IHM modalities, 13 –19 we suspected that such potential downstream changes could offset the cost of receiving IHM. Accordingly, we hypothesized that adults with a new MSK diagnosis receiving covered IHM would have reduced total, medical, and pharmaceutical costs for 1 year compared with those not receiving IHM after a primary care visit, after controlling for confounding variables.
Materials and Methods
Health economic analysis plan
The current retrospective cohort cost comparison study was determined to represent “Not Human Subjects Research” by the University Hospitals (UH) Institutional Review Board (Cleveland, OH, USA, STUDY20230408). Consent was not required for this study as it was retrospective and used administrative data. We adopted the financial perspective of the insurer (UH employee health plan) and focused on direct, allowed costs to assess the financial impact of including IHM within this plan. Data were extracted from January 1, 2018, to the query date on May 4, 2023, with the inclusion window ending 1 year and 4 months earlier to allow for sufficient ascertainment of cost during the follow-up period and any potential lag in claims data. Study reporting adhered to the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 22 and STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statements. 23
Setting and location
University Hospitals is a non-for-profit health system in Northeast Ohio serving the needs of more than 1.5 million unique patients annually. UH Connor Whole Health (UHCWH), a center for IHM embedded within the UH health system, partners with UH physicians, providers, and institutes to meet the growing demand for comprehensive treatment of chronic health conditions and overall well-being. In accordance with prior tenets of whole health, UHCWH seeks to empower and equip individuals to take charge of their health and well-being while emphasizing patients’ goals as the foundation for health care delivery. 24 At the time of accessing the data, there were five UHCWH locations, within and around the city of Cleveland, OH, USA.
The UH accountable care organization was established in 2010 with the objectives of facilitating care coordination, enhancing health care quality, and controlling health costs. 25 To care for the various accountable care organizations UH serves, the UH Population Health Division expanded to serve the employee health plan, akin to how the team serves accountable care organization members from various government and private payor partners. The employee health plan included more than 39,000 beneficiaries at the time of our query. UHCWH provides IHM services to beneficiaries within the UH employee health plan. The employee health plan covers chiropractic examination and treatments (e.g., evaluations, manual therapy, spinal and extraspinal manipulation, physiotherapy procedures), as well as acupuncture and integrative medicine consultations. Although massage therapy was also available through UHCWH, this service was not evaluated as it remains an out-of-pocket expense.
Data sources
The present study used a deidentified dataset extracted from the UH enterprise data warehouse using Alteryx Designer® (version 2021.4, Irvine, CA, USA), which includes data from outpatient and inpatient medical records, administrative claims, financial data, insurer member enrollment files, adjudicated claims, data regarding social determinants of health from the Social Vulnerability Index, as well as out-of-network data originating from the Ohio Health Information Exchange. We only included active and currently attributed employee health plan members for which a claims history and attribution period spanned the study’s time period (including the preceding and prospective 12 months).
Study population
This study included adult beneficiaries aged 18 to 89 years covered under the UH employee health insurance plan (including employees, their spouses, and dependents). Patients were required to have an International Classification of Diseases, 10th Edition (ICD-10), diagnosis within the MSK category (M00-M99) represented in any position within the diagnosis hierarchy. The MSK category includes several diagnoses spanning low back pain, neck pain, osteoarthritis, myalgia, and other soft tissue and joint disorders. This group of diagnoses was selected after a feasibility query in January 2023 by the Population Health Data Science team revealed that the most common conditions treated by IHM clinicians fell within the ICD-10 MSK category (81%). We used a 90-day washout period whereby patients had no recorded MSK diagnosis such that patients were seen for a new episode of an MSK diagnosis. Feasibility testing also demonstrated that patients receiving IHM in the employee health plan had a mean intermediate to high-risk score. Therefore, to maximize generalizability and sample size, we did not exclude patients with specific conditions.
We required patients to be continuously represented in the dataset for 1 year prior to enrollment. This helped ensure that data included in our propensity score matching model were accurate, complete, and not otherwise impacted by newly attributed members with a pent-up demand for health care services. In addition, we required patients to be represented for 1 year after enrollment, to ensure the accuracy of follow-up cost data.
Comparators
Patients were divided into two cohorts: (1) “IHM” defined as receiving any IHM service covered by the employee health plan within 3 months of first diagnosis of the MSK disorder and (2) “No IHM” defined as visiting a primary care provider at the first date of diagnosis of an MSK disorder and not engaging in IHM. The flexible window for the IHM cohort was instituted to allow for a lag period whereby patients could be referred for these services.
Analysis
All statistical analyses were performed using R (version 4.1.2) including functions from the matching, lme4, and emmeans packages. 26 –29 All currency was in United States Dollars (USD). We adjusted for inflation current to the year of the query (2023) using Bureau of Labor Statistics Data. 30 Based on an examination of the distribution of baseline characteristics (i.e., without knowing cost outcomes), we trimmed patients from both cohorts who had over 100,000 USD in prior year total spend to remove high-cost outliers and improve cohort comparability. 31
We used logistic regression to estimate propensity scores which we matched on to build cohorts more comparable with respect to variables that could affect cost. This included assessing matched variables over 1 year prior to and including the date of enrollment, except for comorbidities, which were ascertained from any available time point. Matched variables included those associated with health care cost: (1) demographics (age [continuous], sex [binary], race and ethnicity [categorical] 32 ), (2) comorbidity risk score [categorical], 33 (3) the log of both prior year medical and pharmaceutical spend [continuous], 34,35 (4) prior year health service utilization (emergency, inpatient visits, and office visits [continuous]), (5) prior year prescription count [continuous], (6) use of specialty medications [binary], (7) social vulnerability index (SVI) [continuous], (8) high versus low deductible health plan [binary], and (9) year of diagnosis [continuous]. The comorbidity risk score is a custom metric developed and validated by UH for use to appropriately risk stratify and serve accountable care organization members and those covered by the employee health plan. 36 The comorbidity score was modeled after the Minnesota Tiering model and factors in several weighted comorbidities to derive a unique score for each patient. 36
A 1:1 nearest-neighbor propensity score matching was conducted without replacement, using a caliper width of 0.2 standard deviation. Covariate balance was assessed using standardized mean difference (below 0.2), visualized in a Love plot, and the ratio of the variances of the residuals of the covariates (within a range of 0.5 to 2.0). 37 The final sample size was effectively determined after including all available patients per cohort in the propensity matching strategy.
Considering that cost data are typically skewed to the right rather than normally distributed, we compared the log-transformed cost between cohorts, analyzing least-squares mean (estimated marginal mean) total, medical, and pharmaceutical allowed costs over the 1-year follow-up using a linear mixed model. The model adjusted for the cohort type (i.e., IHM versus No IHM) as a fixed effect and included the matches as a random effect to estimate the differences in the mean log-transformed costs between the two cohorts.
We also conducted a sensitivity analysis using different statistical methods to determine whether our findings would differ. The sensitivity analysis was conducted without trimming based on prior cost and used a generalized linear model (GLM), which has advantages for analyzing skewed cost data. 1 Sensitivity analysis used the propensity matched sample, using emmeans with a log link to calculate estimated mean total, medical, and pharmaceutical costs.
Outcomes
The primary outcome was total cost, while secondary analyses included medical and pharmaceutical costs. Each outcome was assessed over 1 year of follow up. Total costs were considered the sum of all health care costs during the follow-up window, while medical and pharmaceutical costs were subsets of this outcome. We examined allowed costs, as compared to paid costs or out-of-pocket expenses, considering our goal of examining spending associated with covered IHM services from the perspective of the payor.
Results
Descriptive data
Our query identified 260 patients who received IHM and 4,953 who did not. Trimming high-cost outliers reduced the cohort sizes to 251 (IHM) and 4,900 (No IHM), respectively. This equated to a reduction in sample of 3.5% of the IHM cohort and 1.1% of the No IHM cohort. After propensity matching, a total of 251 patients comprised each cohort. Table 1 provides a summary of baseline characteristics before and after propensity matching. Prior to matching, patients in the IHM cohort were younger (42.4 vs. 48.4 years), had a greater proportion of female patients (78.9% vs. 66.9%), and had a different distribution of comorbidity risk index categories compared with the No IHM group. After propensity matching, there were no meaningful between-cohort differences with regards to matched variables (Fig. 1).

Love plot displaying standardized mean differences in baseline covariates before and after matching. PS, propensity score.
Baseline Characteristics Before and After Matching
Used for our primary outcome.
IHM, Integrative health and medicine; HDHP, high deductible health plan; SVI, Social Vulnerability Index; Rx, prescription; SM, specialty medication; SD, standard deviation.
Main results
Least squares mean costs for our primary outcome of total cost [95% CI] (IHM: 3935 [3210, 4824], No IHM: 3232 [2636, 3962]) and secondary outcomes of medical cost (IHM: 3008 [2410, 3754], No IHM: 2130 [1706, 2658]) and pharmaceutical cost (IHM: 177 [127, 245], No IHM: 171 [123, 237]) revealed overlapping 95% confidence intervals for each outcome. Analyzing the difference in least squares mean cost between cohorts (IHM minus No IHM) revealed no meaningful difference in least-squares mean total cost (+703 [95% CI: −314, 1720]) and no meaningful difference in our secondary outcome of pharmaceutical cost (+6 [95% CI: −71, 83]). The difference in least squares mean medical costs did not include zero (+878 [95% CI: 61, 1695]). Cost data are described in Supplemental Table S1, Table 1, and Figure 2.
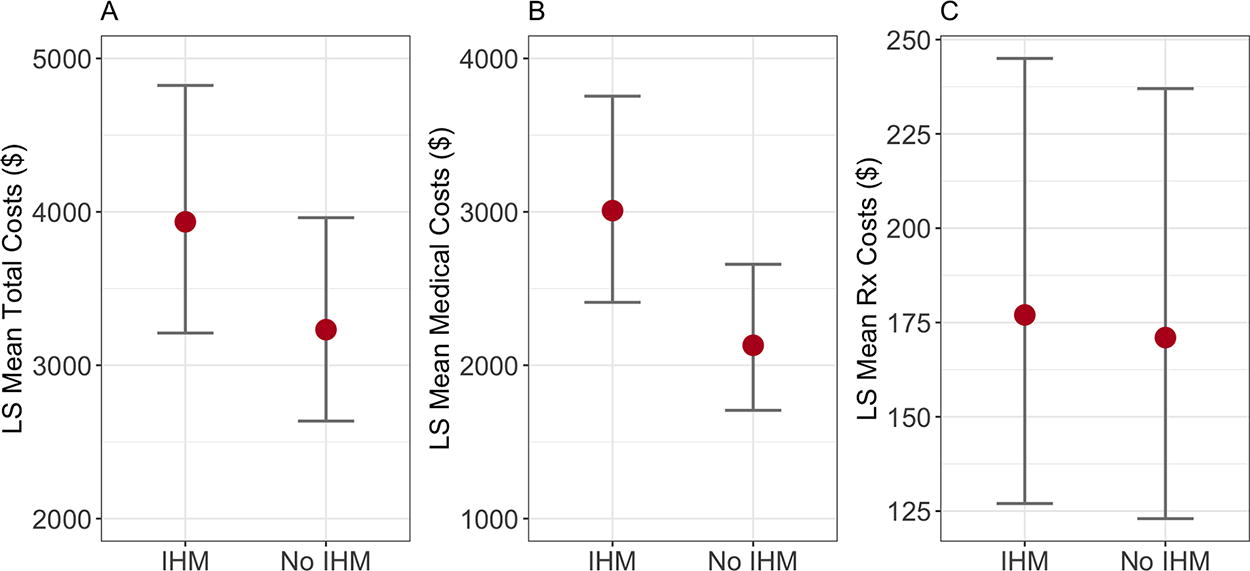
Least squares means cost. Point estimates (red dots) and 95% confidence intervals (brackets) are shown for total cost
Minimum cost values were consistently zero, while the maximum values varied and far surpassed the measures of central tendency and lower quartiles (Supplemental Table S1 and Table 1). Cost means consistently exceeded the median values, providing further evidence of an expected right skew. Least squares means were lower for each outcome compared with the conventional means, suggesting better control over cost variation in our analysis.
The sensitivity analysis using GLM revealed estimated mean costs for our primary outcome of total cost [95% CI] (IHM: 11578 [8911, 15044], No IHM: 14139 [10882, 18371]) and the secondary outcomes of medical cost (IHM: 7860 [5886, 10496], No IHM: 10629 [7959, 14194]) and pharmaceutical cost (IHM: 3718 [2369, 5836], No IHM: 3510 [2236, 5510]). Analyzing the difference in GLM cost between cohorts (IHM minus No IHM) revealed no meaningful difference in total cost (−2561 [95% CI: −7346, +2224]) and no meaningful difference in our secondary outcomes of pharmaceutical cost (+208 [95% CI: −2098, +2513]) and mean medical costs (−2769 [95% CI: −6592, +1055]). Additional results from our sensitivity analysis are shown in the supplementary files (Supplemental Figure S1: Love plot [Fig. 1], baseline characteristics [Table 1], and cost outcomes plot [Supplemental Figure S1]).
Discussion
To our knowledge, this is the first study to examine the cost implications of covering IHM services within an employee health plan. Contrary to our hypothesis, we found no meaningful difference in total health care cost over a 1-year follow-up period between adults receiving IHM and those not receiving IHM after visiting primary care for a new MSK diagnosis. Furthermore, there was no meaningful between-cohort difference in total cost or secondary outcomes in our sensitivity analysis using GLM without trimming.
Our secondary outcome of total cost subsets indicated no meaningful difference in pharmaceutical cost yet a potential increase in medical cost in the IHM cohort compared with the No IHM cohort. Our study was not powered to draw firm conclusions for these secondary outcomes, raising the possibility of type I error. Aside from a statistical interpretation, it remains possible that greater spending for IHM services would add to medical costs, though this increment might not be meaningful when considering total health care expenditures.
There are several possible reasons to explain our finding of no total cost difference between the cohorts. First, care delivered within the UH employee health plan model aims to avoid unnecessary tests and treatments, and this approach may have minimized costs in both cohorts. 38 Second, we were required to use a flexible inclusion window wherein IHM patients could have received other care within 3 months after their MSK diagnosis, to account for differences in scope of practice and portal-of-entry status among IHM clinician types. 15 Third, patients in the IHM cohort were equally eligible to have used other medical services (e.g., surgery, physical therapy, and injections) during the follow-up window.
By demonstrating a lack of total cost difference between IHM and No IHM, our findings do refute a belief that IHM is inherently more costly. 4 Accordingly, we encourage other researchers to replicate and build upon our findings to better determine whether IHM maintains cost-neutrality when added as a covered service for MSK disorders. Coverage of nonpharmacologic modalities such as IHM is complex, with cost only being one factor among many considered by stakeholders such as the available supporting evidence, appropriate use of treatments, administrative burden, and potential prior authorizations needed for care. 6 In addition, these results do not speak to the potential impact of IHM on other clinically meaningful outcomes including health-related quality of life, opioid utilization, health care utilization, and missed days of work. 39 Therefore, our insights may help inform insurance stakeholders’ decision to cover IHM, but these decisions should also consider the broader need for measurement of other outcomes (e.g., patient-reported outcomes) besides allowed costs.
Considering our finding of no increase in allowed total health cost with provision of IHM, we contend that IHM remains a viable treatment option for individuals with MSK conditions. IHM can provide several benefits, such as pain relief, improved function, and decreased disability, 2 and is generally well-tolerated. 2,40 In addition, patients may prefer to use IHM due to personal preference, concerns about side effects, or fear of pharmaceutical dependency and addiction. 41 In addition, IHM is recommended by major guidelines for pain and MSK disorders, including The Centers for Disease Control (CDC) Clinical Practice Guideline for Prescribing Opioids for Pain (2022), 41 the American College of Physicians, 42 and a white paper from The Academic Consortium for Integrative Medicine & Health (2018). 39
Strengths and limitations
The study strengths include having a multidisciplinary research team, coverage of IHM in the studied health plan, and inclusion of medical records data, which is not routinely available among economic evaluation studies. 43
A key limitation of this study is the lack of measures of changes in disability, health-related quality of life, pain, and other clinical outcomes, which would enable calculation of cost effectiveness or utility. Patient-reported outcome measures of pain, health-related quality of life, and disability are recorded inconsistently across the study sample and were not feasible to collect. Included IHM services are heterogeneous and may have variable effects on cost 15 ; however, an expected insufficient sample during initial feasibility testing precluded us from performing any subgroup analyses. While markers of health service utilization (e.g., emergency visits) and likelihood of receiving guideline-discordant medications (e.g., opioids) may differ between those receiving and not receiving IHM, 14,15 our study was underpowered to examine these outcomes.
Additional variables that we could not account for were patient or clinician preferences. Patient preferences to receive or not receive IHM may represent a form of selection bias in our study, although we aimed to mitigate the effects of this through propensity matching. For example, some patients who receive acupuncture or chiropractic care may prefer to avoid prescription medications. 44 However, we included two medication-related variables in our matching model. Furthermore, clinicians’ preferences to escalate patients’ care to include more costly services may have served as an unmeasured confounder. Individual clinicians’ practice characteristics vary depending on their background and tendency to adhere to clinical practice guidelines. 14
One limitation of our analysis is the use of log transformation to handle the skewness in cost data. The cost estimates and their confidence intervals obtained from log-transformed data are based on the geometric mean rather than the arithmetic mean. While this distinction can be relevant in certain contexts, our primary outcome showed no meaningful difference when using both linear mixed effects and GLM models and yielded wide confidence intervals which crossed the null in both analyses. This suggests that the potential bias from antilog transformation of the estimates back to the raw scale would be unlikely to alter our primary conclusions.
A recent systematic review suggested that IHM provided in outpatient clinics led to improvements in health-related quality of life, with more than half of included studies using a follow-up window of 6 months or less. 45 Accordingly, our 1-year follow-up window should have been sufficient to test for the presence of meaningful changes in health-related quality of life. Changes in health service utilization (medications, specialist visits, and procedures) are also often evaluated over a 1-year follow-up. 13 –17,19 Accordingly, the duration of follow-up in our study would have been adequate to examine potential changes in health service utilization and had our sample size been larger.
Future studies with a larger sample size should explore concurrent markers of emergency visits, surgery, and medications alongside cost. Our study did not include indirect costs such as missed days of work, yet given our perspective was from the payor, these fell outside the scope of our analysis. Finally, our study focused on a specific population of adults with MSK conditions within an employee health insurance plan, limiting the generalizability of the findings to broader health conditions (e.g., mental health or neurological disorders), populations, and health care settings.
Conclusions
Our retrospective cohort study found that among adult health system beneficiaries with MSK disorders, there was no meaningful difference in allowed total health care costs between those who received IHM and those who did not. These findings refute the notion that IHM is inherently more costly. Considering patients’ preferences, ethical considerations, the value of offering nonpharmacologic treatment options, and the evidence supporting IHM’s effectiveness, payers should consider covering IHM as a viable option for MSK disorders. Further research should corroborate and build upon our findings by including patient-reported outcomes, utilization measures, and occupational outcomes alongside measures of cost.
Footnotes
Acknowledgment
The authors thank the University Hospitals Population Health team members for their help with this study: Aravindh Anantharamakrishnan, James Muisyo, Susan Shea, and Yashashvi Raghuwanshi.
Authors’ Contributions
R.T., J.D., and F.A. conceived of study. R.T., J.D., M.N., T.D., S.R.M., S.S., and T.L. were involved in the design and development of the methods. M.N., T.D., and S.S. were responsible for the study software. S.S. and T.L. performed formal analysis, while M.N. and T.B. conducted the investigation. M.N., T.B., S.S., and T.L. provided the necessary resources for the study. S.S. curated the data for analysis. R.T. wrote the first draft of the article while all authors reviewed, edited, and approved of the article. S.R.M., S.S., and T.L. contributed to the data visualization. F.A., J.D., T.B., and T.L. supervised the research process. F.A. and J.D. were responsible for funding acquisition.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
The work conducted by employees of Connor Whole Health received support from the
Supplementary Material
Supplemental Table S1
Supplemental Table S2
Supplemental Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.