
Abstract
Background:
Currently, no systematic evidence synthesis of the mechanism of action of mindfulness-based approaches exists for pain conditions.
Aim:
To identify and synthesize experimental and clinical studies examining aspects of the mechanism of action of mindfulness for pain relief.
Methods:
The following databases and search interfaces were searched: Embase (via Embase.com) and Medline (via PubMed). Additional references were identified via bibliographies of included studies. The following were the inclusion criteria applied: (1) original studies published in peer-reviewed journals, (2) in adult populations that (3) examined the mechanism of action of mindfulness meditation on pain outcomes or (4) provided conclusions regarding the potential mechanism of action of mindfulness meditation. The studies were selected by two independent reviewers. Discrepancies were resolved by discussion.
Results:
A total of 21 studies published in English met the inclusion criteria, of which 5 studies were clinical studies, which included patients with chronic pain, and 16 studies used experimental pain induction. The investigation into brain mechanisms through functional magnetic resonance imaging and diffusion tensor imaging revealed mindfulness meditation’s ability to modulate brain activity, particularly in the anterior cingulate cortex, anterior insula, and orbitofrontal cortex, and to enhance structural and functional connectivity in regions associated with pain perception. Regarding the role of opioids, findings across five studies indicated that the analgesic effects of mindfulness are maintained even when opioid receptors are blocked, suggesting a nonopioidergic pathway for pain modulation. Pain perception studies highlighted that mindfulness practices foster pain acceptance and modify pain control beliefs, serving as key mediators in improving pain outcomes. For experienced versus novice mindfulness practitioners, results demonstrated that long-term practice enhances pain threshold and reduces pain unpleasantness through increased activity in salience and attentional control regions.
Conclusion:
This systematic review highlights mindfulness meditation as a multifaceted approach to pain management, utilizing mechanisms such as cognitive and emotional reappraisal, nonopioidergic pathways, and enhanced attention in control regions. It emphasizes the role of mindfulness in fostering pain acceptance and altering pain control perceptions, showcasing its broad impact on the neurological and experiential dimensions of pain. However, the predominance of studies on healthy subjects and methodological variations across experiments necessitates careful interpretation of the findings. The review calls for further research to explore the mechanisms of mindfulness in chronic pain populations more deeply, distinguishing the specific effects of mindfulness from nonspecific effects and expanding its applicability in clinical settings for chronic pain management.
Introduction
Mindfulness-based therapies are defined as self-regulated attention strategies based on nonjudgmental awareness of the present moment. 1 Mindfulness can be cultivated through a variety of meditation programmes and even untrained meditation activities. Within each of these strategies, there are numerous variations. Mindfulness-based stress reduction (MBSR) has been linked to a number of positive health outcomes. 2 Different styles of meditation, such as sitting and moving meditation, are paired with behavioral therapy, daily assignment work, and a silent 1-day retreat in the MBSR program. 3 Other mindfulness-based interventions grew out of MBSR, including mindfulness-based cognitive therapy (MBCT) for treating depression, 4,5 mindfulness-oriented recovery enhancement for combating opioid abuse and chronic pain, 6 and mindfulness-based relapse prevention, which has been shown to be effective for addiction treatment. 7
Because mindfulness increases cognitive control 8 and emotion regulation, 9 it may have the ability to address several avenues in this complex network of brain systems which cause pain. 10 Across clinical and experimental contexts, evidence shows that mindfulness meditation may be a promising alternative to reduce pain. The health-promoting effects of meditation are most prominent for pain and pain-related comorbidities, such as fibromyalgia 11 and chronic low back pain, 12 stress, depression, and anxiety. 13 –15
Previous narrative reviews propose that mindfulness alters the meaning, interpretation, and appraisal of nociceptive information, which are important considerations for stabilizing and long-term improvements in chronic pain symptomology, and which can potentially serve as a mechanism against the development of pain over time. 10,16
Currently, no systematic evidence synthesis of the mechanism of action of mindfulness-based approaches exists for pain conditions. Therefore, the objective of this systematic review is to identify and synthesize experimental and clinical studies examining aspects of the mechanism of action of mindfulness for pain relief.
Methods
English language articles were searched from database start up to January 2022 in MEDLINE (via Pubmed.com) and Embase (via Embase.com). To minimize the risk of selection bias, English abstracts of articles in other languages were screened to determine suitability for translation and inclusion into the review. Reference lists of reviews and obtained articles were screened for further studies to include. To obtain additional study information, authors of publications were contacted when necessary. So-called “gray literature” (i.e., Doctoral and Master dissertations) was searched through google scholar. Search terms included “mindfulness AND pain.”
The following were the inclusion criteria used during the screening process: (1) original studies published in peer-reviewed journals, (2) in adult populations that (3) examined the mechanism of action of mindfulness meditation on pain outcomes or (4) provided conclusions regarding the potential mechanism of action of mindfulness meditation. The criteria for exclusion were as follows: (1) articles that did not contain original research (i.e., reviews and meta-analyses, guidelines and/or protocols), (2) clinical trials focusing on treatment gains or efficacy for pain reduction, and (3) studies in languages other than English. The studies were selected by two independent reviewers. Data extraction was also performed by two independent reviewers. Discrepancies were resolved by discussion. All relevant data were synthesized in the table.
The protocol for this systematic review has not been published, and the review is not registered with a systematic review database.
Results
Figure 1 shows a flowchart for the selection of eligible studies. The search strategy initially identified 3957 studies through database searching and 16 additional studies through bibliographic searching. After removing duplicates (n = 958), 3015 articles were screened according to the inclusion criteria. If these were met, the full-text article was retrieved and screened in full for the analysis. A total of 21 studies published in English met the inclusion criteria and were selected for review.
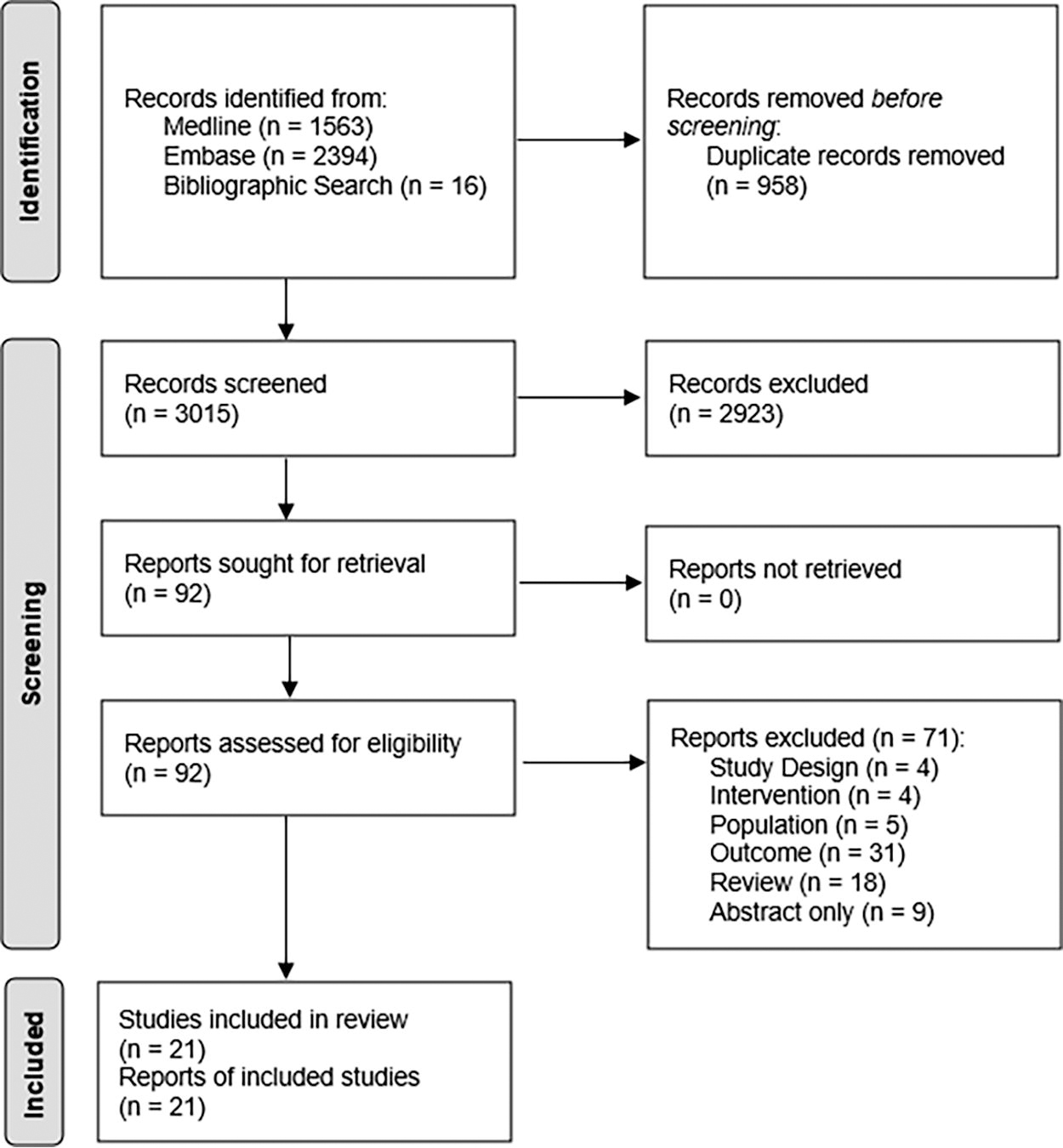
PRISMA flow diagram.
The studies were classified into three broad categories, according to outcomes as follows: (1) neurological outcomes, (2) outcomes comparing experienced versus novice mindfulness practice, and (3) pain perception outcomes, including studies on the role of opioids and other. A summary of the main characteristics of each study, including participants, study designs, sample size, control conditions, outcomes, and conclusions can be obtained from Table 1.
Study Characteristics and Outcomes
ACC, anterior cingulate cortex; AI, anterior insula; AIC, anterior insular cortex; aMCC, anterior midcingulate cortex; CI, confidence interval; daMCC, dorsal anterior midcingulate cortex; DMN, default mode network; DPQ, Dallas Pain Questionnaire; FC, functional connectivity; HF, high frequency; HIT-6, headache impact test; HR, heart rate; HRV, heart rate variability; KIMS, Kentucky Inventory of Mindfulness Skills; MBSR, mindfulness-based stress reduction; MBCT, mindfulness-based cognitive therapy; MRI, magnetic resonance imaging; N/A, not applicable; NNT, number needed to treat; NPS, neural pain signature; OFC, orbitofrontal cortex; PCC, posterior cingulate cortex; PFC, prefrontal cortex; SFMPQ, Short Form McGill Pain Questionnaire; sgACC, subgenual anterior cingulate cortex; SMH, stress management for headache.
Based on the selected articles, seven studies reported on neurological outcomes, 17 –23 two studies examined the difference in pain outcomes with experienced versus novice mindfulness practitioners, 24,25 six studies investigated pain outcomes and the role of opioids, 26 –31 and six studies reported on outcomes related to general perceptions of pain (Table 1). 32 –37
Out of the 21 studies included, 5 studies were clinical studies which included patients with chronic pain, such as low back pain, 34 headache, 19,33 and chronic neuropathic pain. 18,20 Of the 16 studies which used pain induction, 13 were randomized studies 17,22,23,26 –32,35 –37 and 3 were pretest-posttest studies. 21,24,25 Sample sizes ranged from n = 119 36 to n = 15, 29 of which 15 studies had a study population of <100 (Table 1).
Studies on neurological outcomes of pain management with mindfulness
A total of seven studies examined the mechanism of action of mindfulness based on neurological outcomes. 17 –23
Out of these, six studies used functional magnetic resonance imaging (MRI) and one study conducted the test by diffusion tensor imaging. 18 Results indicate that meditation appears to engage multiple brain mechanisms that alter the construction of the subjectively available pain experience (Table 1).
Clinical studies, like those conducted by Mioduszewski et al. (2020), Seminowicz et al. (2019), and Smith et al. (2020), 18 –20 have demonstrated through diffusion tensor imaging and functional MRI that mindfulness meditation enhances structural and functional connectivity (FC) in the brain, particularly increasing fractional anisotropy in the uncinate fasciculus, amygdala, hippocampus, and improving connectivity between the posterior cingulate and medial prefrontal regions. These changes correlate with reductions in pain perception and severity in conditions like episodic migraine and chronic neuropathic pain (Table 1).
In contrast, experimental studies by Kober et al. (2019), Su et al. (2016), Zeidan et al. (2011), and Zeidan et al. (2015), 17,21 –23 utilizing functional MRI in healthy subjects, have identified mindfulness meditation’s activation of the anterior cingulate cortex (ACC), anterior insula (AI), and orbitofrontal cortex (OFC), alongside reduced activation in the primary somatosensory cortex and amygdala, outlining a detailed map of neural mechanisms that mediate the pain-relieving effects of mindfulness (Table 1). For example, the experimental studies by Zeidan et al. (2011, 2015) demonstrated that mindfulness meditation significantly reduced both pain intensity and unpleasantness ratings, linking these effects to changes in brain activity (Table 1). 22,23
Studies examining experienced versus novice mindfulness practice
In comparing experienced mindfulness practitioners with meditation-naïve individuals, Lutz et al. (2013) and Perlman et al. (2010) found that although pain intensity remained consistent across groups, experienced meditators reported significantly less pain unpleasantness (Table 1). 24,25
Studies investigating the role of opioids in pain outcomes
Out of the six studies investigating the role of opioids in pain outcomes with mindfulness, five reported findings indicative of a nonopioidergic pathway facilitating the pain-relieving effects of mindfulness meditation. 26 –28,30,31 Specifically, these studies found that mindfulness meditation reduced pain intensity and unpleasantness in participants, even when opioid receptors were blocked by naloxone, highlighting a mechanism independent of the body’s endogenous opioid system. For instance, May et al. (2018) observed enhanced meditation analgesia under naloxone blockade, suggesting that long-term meditation practice strengthens nonopioidergic pain modulation. 28 Similarly, Zeidan et al. (2016) reported that mindfulness meditation activated brain regions associated with cognitive modulation of pain, such as the OFC and ACC, without the involvement of opioidergic pathways (Table 1). 31
Studies on general pain perception
Mindfulness meditation was found to enhance pain management through mechanisms such as increased pain acceptance, changes in pain control beliefs, and reductions in pain catastrophizing across both clinical 33,34 and experimental studies, 32,35 –37 with one experimental study (Adler-Neal et al., 2020) demonstrating that mindfulness also led to physiological changes, such as increased heart rate variability (HRV), associated with reduced pain unpleasantness (Table 1). 32
Discussion
According to this review of the existing literature, mindfulness meditation for pain relief appears to have favorable effects via multiple modes of action; however, the major mechanism via which the therapeutic effect is supplied could not be clearly identified from the current research.
The results of this review show that mindfulness meditation-based pain alleviation engages a variety of mechanisms that are representative of reappraisal processes that are not relying on a single brain mechanism to alleviate pain. These pathways elucidate how mindfulness meditation influences pain perception and management through a combination of neurological, cognitive, and experiential changes, distinct from opioid-based mechanisms. The included brain studies have shown that mindfulness meditation affects pain perception by regulating emotional intensity and altering brain activity, reducing negative affect and pain by modulating activity in the amygdala and other pain-related brain regions, leading to a significant decrease in the neural pain signature. This suggests that mindfulness regulates pain through cognitive and emotional reappraisal mechanisms. However, the majority of these studies presented clear hypotheses but generally lacked clear primary outcome parameters and did not conduct sample size calculations. This suggests a methodological weakness in these studies, potentially affecting the clarity of their objectives and the statistical power to detect meaningful effects. 17,18,20 –23
The results of the studies investigating the role of opioids in pain relief indicate that the pain-relieving effects of mindfulness meditation do not rely on endogenous opioids. The majority of studies using naloxone, an opioid antagonist, have shown that mindfulness meditation’s analgesic effects are maintained even when opioid receptors are blocked, pointing to a nonopioidergic pain modulatory pathway. 26 –31
The clinical studies examining general pain perception reveal that pain acceptance and changing pain perception and control beliefs are key mediators in MBCT for improving outcomes in patients with headache and chronic low back pain. 33,34 Meanwhile, experimental investigations highlight distinct mechanisms of mindfulness meditation in pain modulation, including increased HRV, enhanced pain threshold, more complex cognitive and affective pathways beyond physiological changes, and the pivotal role of acceptance in pain management. 32,35 –37
Additionally, the accumulated experience of meditation practice significantly affects the perception and modulation of pain. Experienced meditators show reduced pain unpleasantness and enhanced activity in brain regions associated with salience and attentional control, indicating that long-term practice cultivates an experiential awareness that downregulates anticipatory anxiety and recruits attentional resources more efficiently during pain processing. 24,25
Pain is a complex and subjective conscious experience that is shaped and modulated by a variety of sensory, cognitive, and affective factors, such as mood, psychological disposition, learning, expectations and prepain cognitive states (e.g., expectations; anxiety). 9,10,38 –42 Additionally, the setting in which pain arises continues to have a significant impact on the subjective experience of pain. Previous experiences, expectations, attitude, training, desires, sensitization/habituation, and other cognitive factors can all drastically increase or decrease pain. 10,42 –47 Peripheral primary afferents register nociceptive sensory events at the site of injury/tissue destruction, and subsequently convey this information to the dorsal horn of the spinal cord. Nociceptive information travels from the spinal cord to the brain contralateral to the site of pain, primarily via the spinothalamic pathway. Feedback connections between lower-level sensory regions, such as the parabrachial nucleus, periaqueductal gray matter (PAG), thalamus, and main and secondary somatosensory (SI) cortices, are used to process nociceptive input, 9,10,38 –42 with the ascending nociceptive information then being sent to the posterior and anterior insular cortices (AICs), where it aids with pain appraisal. 48 The activation of higher-order brain areas such as the ACC, dorsal ACC (dACC), and prefrontal cortex (PFC) facilitates the contextual meaning of pain. 10,48,49
Previous research has shown that mindfulness may be a promising intervention at reducing pain, 50 –53 and the results of the present systematic review concur with previous reviews that it does so via involving processes that reflect changes in one’s relationship with pain. 3,10,16 The identified studies on the comparison of novice (short-term) versus experienced (long-term) mindfulness practice 24,25 indicate that with more experience, the mechanisms enabling mindfulness-based pain treatment will grow more impactful, in contrast to standard pain medicines, which show rising tolerance and efficacy plateaus. 54 –56
These results are in agreement with other authors, implicating that the brain processes that underpin mindfulness-induced pain reduction alter depending on the level of meditation, where mindfulness-based pain relief is associated with higher order (OFC and rostral ACC) regulation of low-level nociceptive neural targets (thalamus and primary somatosensory cortex) after brief mindfulness-based mental training, suggesting an engagement of unique reappraisal mechanisms. 3,10,16 Mindfulness-based pain alleviation, on the other hand, is associated with prefrontal deactivation and increased activation of somatosensory cortical regions after extensive training, suggesting an ability to minimize evaluations of emerging sensory stimuli. 3,10,16
Zeidan et al. (2016) 10 postulates that activation of the OFC may help the thalamic reticular nuclei generate inhibitory connections, reducing nociceptive information throughout the cortex (evidenced by reductions in thalamic, PAG, and SI activation). Neuroimaging data adds to the understanding of these events. Through alterations in executive attention, novice meditators use higher-order brain areas (OFC, subgenual ACC [sgACC], AI) to downregulate ascending nociceptive input at the thalamus level. As a result, following a short period of mental training, meditation has an effect on sensory and affective pain responses. 10 Long-term meditation practice, on the contrary, is associated with much increased activation in sensorimotor areas and inactivation of appraisal-related brain regions. Long-term meditation practitioners’ decoupling between sensory experience and meaning and/or contextualization of what pain means to them provides evidence that meditation’s analgesic effects can be developed and enhanced with more practice, which is important for those seeking long-term narcotic-free pain relief. 24,25
The results of this present systematic review show that meditation was observed to significantly lower pain intensity and unpleasantness ratings when compared with rest and control groups, regardless of naloxone or placebo-saline delivery. The endogenous opioidergic system includes cannabinoid, serotonergic, dopaminergic, cholecystokinin, adrenergic, and other neurochemical systems (i.e., vasopressin). Endogenous opioidergic systems have been shown to mediate analgesia induced by placebo, 57,58 conditioned pain modulation, 59 acupuncture, 60 and hypnosis 61 on several occasions. Significant reductions in pain-related brain activation (i.e., SI, posterior insula, parietal operculum) and activation in higher-order brain regions, such as the ACC, PFC, and insula, are associated with pain alleviation provided by these cognitive approaches. 62 –67 The PFC, insula, and ACC all have significant levels of opioid receptors and are linked to the production of analgesia via descending inhibitory networks. 68 –71 Meditation appears to decrease pain via involving brain regions with high concentrations of opioid receptors (sgACC, OFC, AI). 58,68,72 In addition, mindfulness meditation lowers activation in the PAG, a brain area involved in opioid-mediated descending pain suppression. 73,74 The findings of the present systematic review add to the growing body of data that mindfulness meditation reduces pain through mechanisms other than opioid dependent pathways, which is significant for chronic pain patients looking for a fast-acting nonopioid pain treatment.
Some of the identified studies in this review indicate that although the processes to promote mindfulness-based pain management may not directly correspond to reducing pain intensity, they do imply that mindfulness modifies the contextual appraisal of both pleasant and unpleasant sensory stimuli, and mindfulness meditation had a greater impact on the affective dimension of pain than on the sensory dimension, with the unpleasantness dimension of pain being considerably reduced with respect to pain intensity across some of the identified mindfulness/pain-focused experiments, 23 –25,31 which is a relevant impact when contemplating the use of meditation for clinical pain.
The research identified in this review, which were mostly conducted on healthy, pain-free people, have elucidated distinct pain-relieving mechanisms, such as cognitive and emotional reappraisal mechanisms, nonopioidergic pain modulatory pathways, acceptance in pain management, or enhanced activity in attentional control regions, which may now allow for the development of more effective mindfulness-based therapies to treat certain chronic pain problems. However, while the results from the majority of studies included in this systematic review have indeed provided valuable insights into the potential mechanisms through which mindfulness practices may influence pain perception, there are important limitations in generalizing these findings to patients with chronic pain conditions. First, it is crucial to acknowledge that pain experiences in healthy individuals and chronic pain patients are fundamentally different. In healthy subjects, pain typically serves as a protective mechanism, warning the body about potential or actual tissue damage. It is usually acute and short-lived, subsiding as the body heals. On the contrary, chronic pain persists or recurs over long periods, often beyond the normal healing period, and can be out of proportion to any observable injury or disease. 75 It can also be associated with conditions where the nociceptive (pain sensing) system itself may be damaged, such as in neuropathic pain. 76 Therefore, the neural mechanisms underlying acute pain in healthy individuals may differ significantly from those underlying chronic pain. Second, chronic pain is often associated with significant psychological distress and comorbid mental health conditions such as depression and anxiety. 77 These can significantly modulate pain perception and response to pain management interventions, including mindfulness. 78,79 The interplay of these psychological factors in the context of chronic pain is complex and may not be adequately reflected in studies involving healthy participants. Additionally, people living with chronic pain may have altered baseline brain structures and function due to the persistent pain experience. This includes changes in brain regions associated with pain modulation, such as the PFC and the ACC. These alterations could potentially affect the response to mindfulness interventions, as mindfulness practices are known to engage these areas and promote their FC. 10,48,49 Pain experiences and coping strategies also can vary widely among individuals with chronic pain, depending on factors like the specific nature of their condition, its duration, their personal and social resources, and their previous experiences with pain management interventions. 80 These variations add another layer of complexity to the generalizability of findings from healthy subjects to chronic pain patients.
Although the neuroscience of mindfulness-based pain management is still in its early stages, it has already demonstrated its ability to expand the known brain modulatory pain pathways and shed light on the complex affective and psychological aspects of pain management. The vast number of people suffering from chronic pain around the world highlight the potential value of developing validated self-administrable mind–body therapies that target pain in multiple ways via several distinct neuromodulatory pathways. However, due to the wide range of mindfulness meditation techniques and the biopsychosocial complexity of chronic pain conditions, future research should continue to use the highest experimental standards to investigate the clinically relevant treatment protocols to achieve long-term improvements in chronic pain management. Mindfulness-based techniques may play a role in changing the meaning, interpretation, and assessment of nociceptive information on its path to creating the subjective experience of pain.
Because the majority of the identified studies were conducted in healthy participants, more brain imaging and neurophysiological research is needed to delineate the processes through which mindfulness affects chronic pain. Hence, the results of these studies may not be transferable to the chronic pain population. In particular for chronic pain populations, there needs to be a better understanding of the brain pathways that promote mindfulness-based pain treatment. The brain processes that promote pain alleviation in chronic headache, for example, may differ from those that have been demonstrated to be beneficial in treating back pain.
Additionally, mindfulness meditation may be prone to nonspecific effects, i.e., slow breathing, demand characteristics, beliefs related to practicing meditation, conditioning, or posture, hence, placebo/sham-based comparisons are strongly recommended to better separate real mindfulness mechanisms. 16 In the current review, only three studies 23,30,32 using a placebo/sham control as a replacement for mindfulness meditation were identified, which highlights the scarcity of these approaches and the need for more rigorous future research in this area. Because three of the studies lacked a matched and active control group, 21,24,25 it was difficult to determine if mindfulness lowers pain through brain pathways similar to placebo analgesia or other nonspecific influences.
Furthermore, the vast range of potential between-study and between-group variations (e.g., demographics, study characteristics, and meditation protocols) across the identified studies limits their generalizability to specific populations or treatment protocols.
Conclusion
The research reviewed herein underscores mindfulness meditation as a multifaceted approach to pain management, revealing its efficacy through cognitive and emotional reappraisal mechanisms, nonopioidergic pain modulatory pathways, and enhanced activity in attentional control regions. Notably, mindfulness practices foster pain acceptance and alter perceptions of control over pain, indicating a comprehensive influence on both neurological and experiential aspects of pain. Despite these promising findings, the studies’ methodological limitations, including a focus on healthy individuals and varying experimental designs, call for cautious interpretation. This review highlights the need for future research to delve deeper into understanding mindfulness’s impact on chronic pain and exploring the mechanisms in populations with chronic pain conditions. Future studies should also differentiate the specific contributions of mindfulness techniques from nonspecific effects and extend investigations to clinical populations to confirm mindfulness-based interventions’ applicability and efficacy in managing chronic pain.
Footnotes
Authors’ Contributions
M.P. was responsible for conceptualization, data curation, formal analysis, methodology, and writing—original draft. D.M. was responsible for conceptualization, supervision, validation, and writing—review and editing.
Data Availability
The data of this systematic review can be provided by the corresponding author on reasonable request.
Author Disclosure Statement
The authors of this publication declare no conflict of interest.
Funding Statement
This work did not receive any funding.