
Abstract
Objective:
The Non-Opioid Pain Alleviation Information Network (NOPAINMN) project was designed to identify, consolidate, and map evidence-based non-opioid and non-pharmacological pain management complementary and integrative health (CIH) modalities for chronic pain management across Minnesota into a searchable and informational website (www.nopainmn.org ).
Methods:
The Academic Consortium for Integrative Medicine & Health's Pain Task Force White Paper identifying evidence-based research of non-pharmacological pain practice (NPPC) was reviewed and referenced. National and state certifying boards and accrediting organizations for NPPC modalities were accessed to identify Minnesota-based NPPC providers' name, business/health-system affiliation, address, contact information, and credentials. The NOPAINMN website displays these data in a consumer-facing website with searchable fields such as NPPC modality type, and location with varying distances. The website was β-tested by practitioners and stakeholders for optimization. Eight main NPPC modalities and their respective subcategories were identified and mapped: Acupuncture; Integrative Medical Care (Functional medicine consultation and Integrative medicine consultation); Massage Therapy; Mind–Body Therapies (Biofeedback, Clinical Hypnosis, Mindfulness-Based Stress Reduction, and Music Therapy); Movement Therapies (Tai Chi, qigong, and Yoga Therapy); Psychology (Cognitive Behavioral Therapy); Rehabilitative Therapies (Physical and Occupational Therapy); and Spinal Manipulation.
Results:
All information compiled resulted in 17,155 providers/practitioners. Physical Therapy had the greatest number of reported providers (n = 5224), followed by Occupational Therapy (n = 3792), Psychology (n = 3324), Chiropractic (n = 3033), Acupuncture (n = 591), and Massage Therapy (n = 544). The Resource Map included 56 major health systems, 686 facilities, 2651 solo or private group practices, and 14 academic training schools. With web-based cross-referencing, providers and facilities were affiliated and linked with health systems to produce an interconnected mapping system. β-Testing with patients found that the website was reported as relatively easy to use and informative.
Conclusion:
The website was created to assist individuals, health care providers, insurance carriers, and health care facilities in finding evidence-based information and resources on NPPC to guide, support, and proactively manage and engage chronic pain patients across Minnesota.
Introduction
Chronic pain exerts an enormous personal and economic burden, affecting more than 30% of people worldwide according to some studies. 1 Chronic pain affects at least 116 million American adults—more than the total affected by heart disease, cancer, and diabetes combined. Pain also costs the United States up to $635 billion each year in medical treatment and lost productivity. 2 Even with treatment, chronic pain is a chronic disease with psychological implications. 1
Opioids are used to address chronic pain issues regardless of underlying cause or severity. While opioids may offer short-term pain relief, there is insufficient evidence to suggest that opioid treatment provides prolonged benefits to individuals with chronic pain. 3 In addition, opioids are associated with more harmful side effects when compared with other non-opioid treatment options and are highly addictive. 4 In addition, across the United States, deaths rose in the 2019 to 2021 timeframe, with more than 106,000 drug overdose deaths in 2021. 5
In the 1990s, the opioid epidemic was ignited with overprescribing opioids to treat pain. The inability to identify, engage, and treat patients with evidence-based opioid addiction treatment options further exacerbated the epidemic. The full impact of these changes was not fully recognized until the increase in deaths associated with opioid abuse emerged. 6 Minnesotans have suffered tremendously from the opioid epidemic, with preliminary data from 2021 indicating a 35% increase in the total number of overdose deaths involving opioids since 2020 (from 685 deaths in 2020 to 924 deaths in 2021). 7
Given the parallel crises of chronic pain and opioid misuse, there is a need to shift the approach toward pain management. Numerous studies and reviews highlight the growing evidence behind the efficacy and safety of non-pharmacological modalities in managing chronic pain and associated comorbidities. 8,9 Specifically, the Academic Consortium for Integrative Medicine & Health's Pain Task Force White Paper 8 was a comprehensive review of the impact of acupuncture, manipulation, massage therapy, relaxation techniques, and movement techniques (e.g., yoga and Tai Chi) toward reducing chronic pain related to osteoarthritis, back pain, neck pain, and migraines.
Furthermore, in a large systematic review and meta-analysis, mind–body therapies 10 were associated with moderate reductions in pain and small reductions in opioid doses. Recent large-scale epidemiologic studies have shown that chiropractic 11 and physical therapy 12 have positive effects in initiation and use of opioids.
This research is further supported by recommendations by the Centers for Disease Control and Prevention 13 the Joint Commission 14 and American College of Physicians 15 that emphasize the importance of increasing access to non-pharmacological modalities as the first-line treatment for chronic pain.
The utilization of these non-pharmacological modalities, also referred to as complementary and integrative health (CIH) services, is substantial. The 2012 National Health Interview Survey (NHIS) reports that ∼33% of U.S. adults used a CIH approach in their health care. 16 In 2017, there was a substantial increase in usage of yoga, meditation, and chiropractic care. 17 As a result, there is growing demand for patients to access information on CIH services, including locating and evaluating evidence-based non-pharmacological pain practice (NPPC) CIH services in health care.
CIH users often identify treatment options based on personal referrals from friends and family. 18,19 Factors such as cost, proximity to service location, and provider characteristics, including personality, gender, and race, are also included in decision-making about CIH utilization. 18 Chronic pain patients report hesitancy when speaking with their primary care providers about CIH options because of possible stigma, limited appointment time, and perceived lack of provider knowledge of different CIH treatment options for specific conditions. 18,19
Consequently, many patients turn to the internet as another resource to learn about and identify CIH resources. However, it can be challenging for patients to verify the accuracy of information and effectively evaluate the quality of resources listed online. 20
To assess the demand and effectiveness for CIH, in 2012, the BraveWell Collaborative organized a national mapping project to identify various health centers and academic institutions with CIH programs. 21 Since then, there have been no mapping studies and none that are specific for integrative pain management. As such, there is a clear need to provide both patients and providers with evidence-based NPPC CIH information. 22
In 2019, Minnesota passed opioid legislation HF 400, which required all funds received by the state through an opioid-related lawsuit or settlement to be used for opioid abatement. The law also created the Opioid Epidemic Response Advisory Council (OERAC), which oversees and distributes much of the money collected through the settlements.
In fiscal year 2020, $1.25 M was appropriated from the general fund to the commissioner of health, to provide funding for NPPC for a statewide mapping and assessment of community-based nonnarcotic pain management and wellness resources. This fund also supported up to five demonstration projects in different geographic areas of the state to provide community-based NPPC and wellness resources to patients and consumers. 23 Hennepin Healthcare received competitive funding for the mapping project titled the Non-Opioid Pain Alleviation Information Network (NOPAINMN) in Minnesota.
The objective of the project was to consolidate evidence-based NPPC CIH resources from both academically affiliated and nonacademic health organizations, and communities across the state into one interactive, searchable, and consumer-friendly online database. An accompanying article will also be published identifying the barriers and facilitators to CIH utilization from qualitative analysis of interviews with various stakeholders in Minnesota for chronic pain management.
Materials and Methods
Literature review of NPPC modalities
An online comprehensive literature review was conducted through PubMed and Google scholar to identify NPPC CIH modalities with the most evidence-based research. The consolidated research provided by The Academic Consortium of Integrative Medicine and Health Pain Task Force White Paper 8 was referenced to finalize the selection of NPPC CIH modalities to be mapped. This information was further cross-referenced with research published on the National Center for Complementary and Integrative Health (NCCIH) website. 24
Based on the literature review, inclusion and exclusion criteria for modalities were developed and disclaimers were included. However, two important clarifications are needed. First, the authors use the term for the modality (spinal manipulation) rather than the profession of chiropractic. 25 Second, while there is increasing evidence that integrative medicine physician consultations improve outcomes in general integrative medicine clinic patients, 26 integrative and functional medicine physicians may likely provide advice and referral, rather than a treatment, unless they have additional certifications or training in specific modalities.
Locating and mapping NPPC practitioners and locations
In planning the Resource Map, seven regions listed by the Minnesota Statewide Emergency Communications Board (MNECB) were referenced: central, metro, northeast, northwest, south central, southeast, and southwest (Fig. 1). The seven Minnesota regions were used to ensure comparable inclusion and accessibility of geographic locations and services from the entire State of Minnesota.
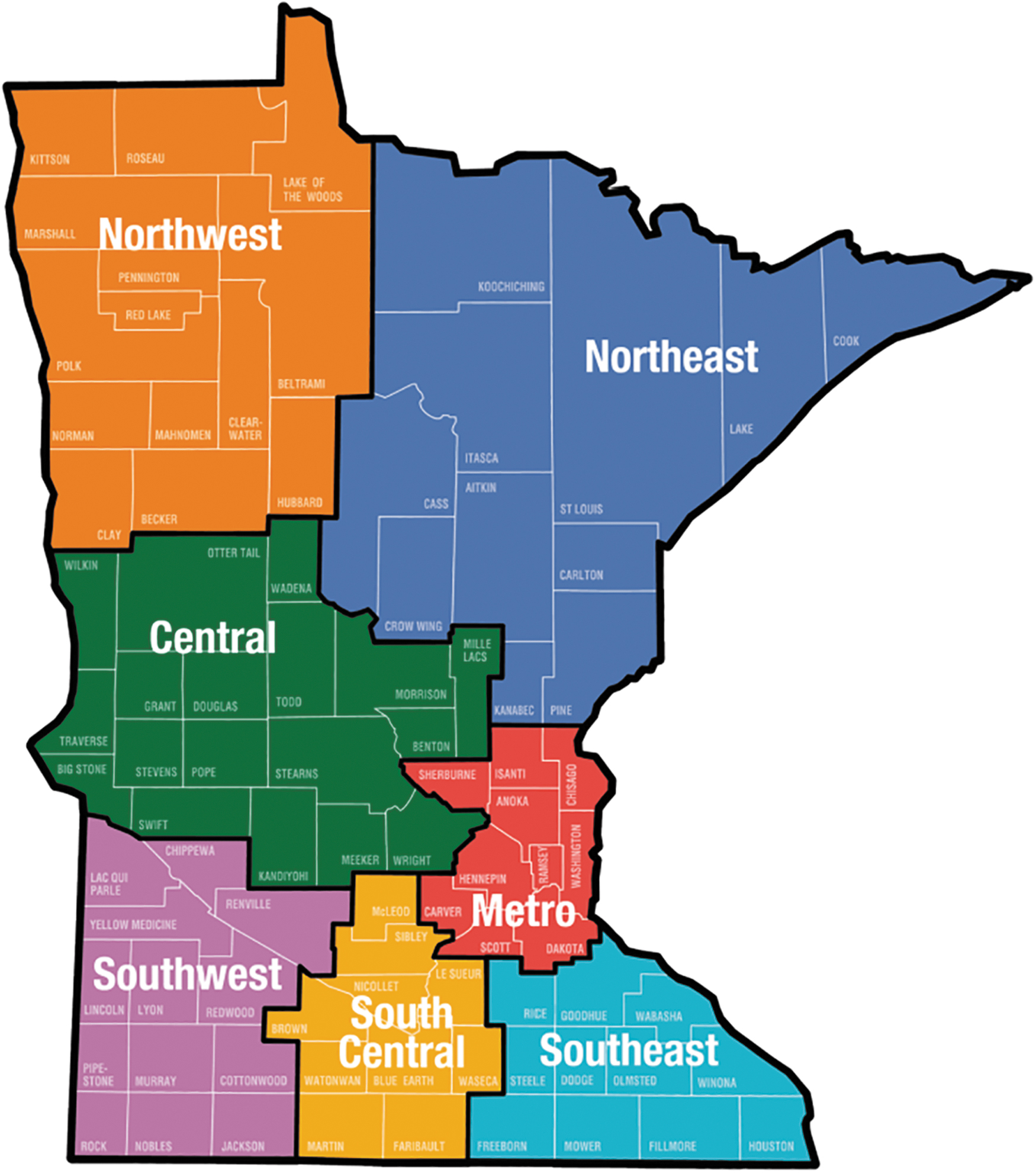
MNECB Map. MNECB, Minnesota Statewide Emergency Communications Board.
Publicly available databases provided by national and state certifying boards, accrediting organizations, and other data sources were accessed to locate licensed and credentialed NPPC providers across the state of Minnesota. Provider name, business or health system affiliation, address, contact information, and credentials were obtained and organized into master spreadsheets. Board and accrediting body information were complemented by internet search results of listed providers to verify current contact information and affiliation.
Providers were only included if they were listed by the identified certifying and accrediting organizations. Health systems and designated facilities affiliated with the Minnesota Hospital Association (MHA) offering NPPCs were additionally documented in the master spreadsheet for mapping. Accredited schools that train CIH practitioners and provide the respective non-pharmacological therapies were also mapped.
Website and map development
An experienced website design developer was contracted with expertise in both backend and frontend programming, and in programing and designing interactive digital maps. The developer provided frontend programming such as user interface design, website structure and layout, and backend programming regarding information architecture, programming mapping features, and provider information database.
Website content
Content such as treatment descriptions, evidence-based research articles, links, and resources were developed and gathered for the listed modalities. This information was reviewed by Content Expert Reviewers who were either practitioners or subject-matter-experts. The team engaged Hennepin Healthcare System's (HHS) division of Integrative Health faculty and providers in creating multimedia content of NPPC modalities with descriptive pictures and videos.
User experience and usability testing
Remote unmoderated qualitative usability testing was conducted between April and May 2022 to identify potential problems in the website design, uncover opportunities to improve, and to learn about user behavior and preferences. The usability testing was conducted with a targeted convenience sample consisting of individuals who participated in the qualitative interview portion of the project and those who participated in a chronic pain group medical visit program at HHS.
Administered through REDCap, the user experience and usability testing asked participants to complete a set of tasks using the website and then complete a survey about their experience within the domains of navigation, user satisfaction, website content evaluation, and visual evaluation of the website and map.
Ethics/IRB
This project was classified as a program assessment and as such was determined to be exempt by the HHS IRB.
Results
Inclusion and exclusion of NPPC modalities and information on website
Based on a literature review, eight main modalities and their respective subcategories were identified and included on the Resource Map. As shown in Figure 2, individuals who navigate to the landing page will see a rolling selection of NPPC modalities and pathway buttons to enter the website. Figure 3 is a screenshot of what an individual would see on the Resource Map if they selected “acupuncture,” zip code of 55404 and distance of 5 miles (8 kilometers). Separate tabs were created for treatment descriptions, evidence-based articles, links, and resources.

NOPAINMN website landing page with QR code. NOPAINMN, Non-Opioid Pain Alleviation Information Network.
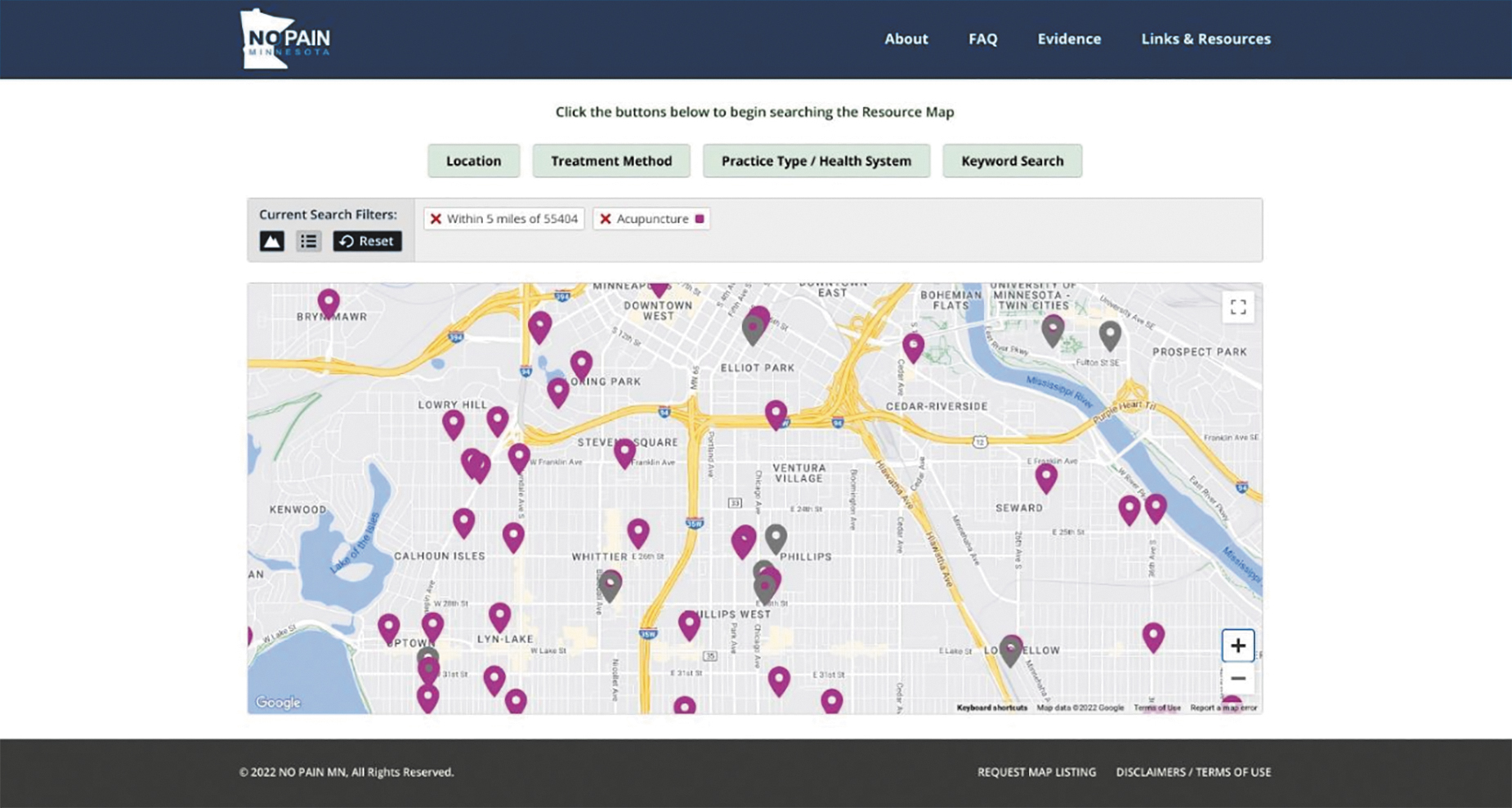
Screenshot of the Resource Map with search filters enabled.
These modalities are listed in Table 1 in alphabetical order: Acupuncture; Integrative Medical Care (Functional Medicine Consultation and Integrative Medicine Consultation); Massage Therapy; Mind–Body Therapies (Biofeedback, Clinical Hypnosis, Meditation/Mindfulness-Based Stress Reduction, and Music Therapy); Movement Therapies (Tai Chi, qigong, and Yoga Therapy); Psychology; Rehabilitative Therapies (Physical Therapy and Occupational Therapy); and Spinal Manipulation. Figure 4 is the list of these evidence-based treatment methods on the website.
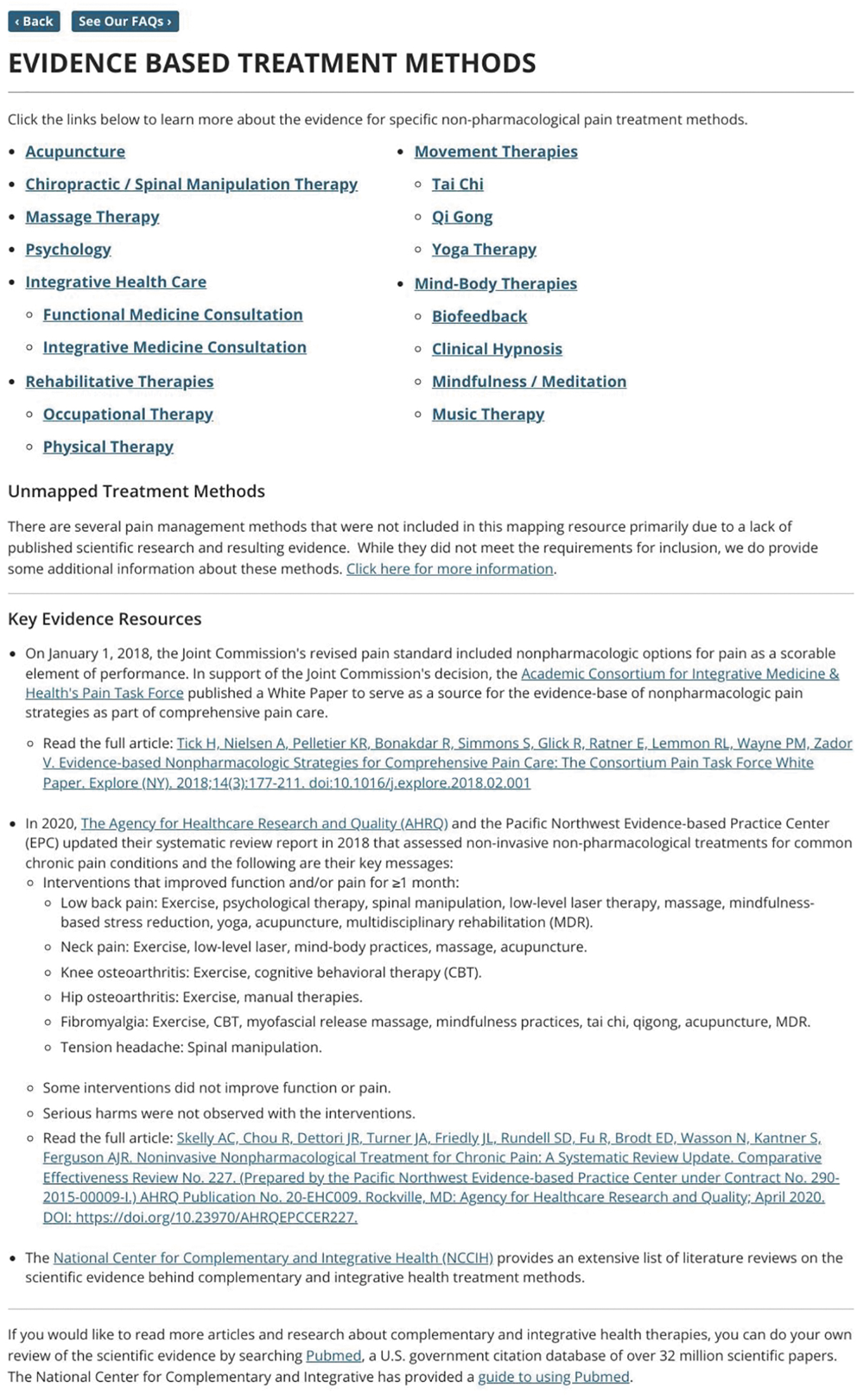
List of evidence-based treatment methods included on the NOPAINMN website.
Non-Opioid Pain Alleviation Information Network Mapped Modalities, Number of Providers, and Data Source
Total number does not include another 3205 practitioners that are missing latitude/longitude coordinates due to insufficient professional contact information from data source, particularly from Physical Therapy and Occupational Therapy.
AMTA, American Massage Therapy Association; ASCH, American Society of Clinical Hypnosis; BCIA, Biofeedback Certification International Alliance; CBMT, Certification Board for Music Therapists; IAYT, International Association of Yoga Therapists; IFM, Institute for Functional Medicine; NBCTMB, National Board Certification in Therapeutic Massage and Bodywork.
The literature review identified homeopathy, naturopathy, guided imagery, Pilates, Alexander technique, and Feldenkrais method as other non-pharmacological modalities. However, these therapies were not included in the Resource Map for reasons including limited evidence-based research related to chronic pain management, lack of a uniform certifying process, or lack of recognized training standards in the state of Minnesota.
When considering the spinal manipulation modality, it was determined not to list Doctors of Osteopathy (DO) as it was difficult to identify DO practitioners who continue to practice manipulation techniques. However, some DOs were listed in the Resource Map along with Medical Doctors (MD), Doctor of Pharmacy (PharmD), Physicians Assistants (PA-C), and Certified Nurse Practitioners (CNP) if they were certified in integrative or functional medicine.
NPPC practitioner and location database
All information complied, based on evidence and inclusion/exclusion criteria, resulted in 17,155 providers/practitioners. Table 1 also includes the respective number of providers per modality and the organization queried for information. Physical Therapy had the greatest number of reported providers (n = 5224), followed by Occupational Therapy (n = 3792), Psychology (n = 3324), Chiropractic (n = 3033), Acupuncture (n = 591), and Massage Therapy (n = 544). The Resource Map includes 56 major health systems, 686 facilities, 2651 solo or private group practices, and 14 academic training schools.
User experience and usability testing of the NOPAINMN website
A convenience sample of 50 participants were invited to pilot test the website and 30 were able to complete the usability testing (60% completion rate). Participants were chronic pain patients (n = 10), CIH providers (n = 10), non-CIH medical providers (n = 6), health insurance representatives (n = 3), and health care administrator (n = 1). Participants had a mean age of 47.83 (standard deviation 11.44), 60% were female, 80% were White/Caucasian, 10% were Black or African American, and the highest level of participants' education was a college degree (13.3%) or graduate or professional degree (67%).
Participants generally reported a positive experience pilot testing the website and Resource Map (Table 2). Participants rated all domains positively, including Navigation, User Satisfaction, website Content, and website and Map Visuals. In testing the website, most participants were satisfied, found it easy to navigate, found the content helpful, and rated the visuals positively. Out of 30 participants, 11 (36.7%) expressed facing some navigation challenges while using the website. These challenges were corrected from participants' feedback. Overall, many expressed excitement and hope about the website as a resourceful tool.
User Experience and Usability Testing Results of the Non-Opioid Pain Alleviation Information Network Website
Discussion
As a convenient resource for all stakeholders, this HHS-funded mapping project aimed to create an educational and interactive website of the location and availability of evidence-based NPPC services and providers in Minnesota. Qualitative interviews with stakeholders within chronic pain management that highlight facilitators and barriers to NPPC care will be published in a separate complementary article.
Based on the inclusion and exclusion criteria as described earlier, close to 17,000 providers of NPPC and their practice locations were mapped across Minnesota. The website/map includes evidence-based information and lists up-to-date research articles as of May 2022, for all the mapped modalities in a user-friendly searchable option. Pictures and videos are provided to make each integrative modality easily understandable to users.
To the team's knowledge, no other mapping study of any U.S. state with NPPC resources exists, making Minnesota the only state to have developed this resource to benefit multiple stakeholders. This project has discovered the richness and diversity of the network of NPPC CIH providers in certain parts of Minnesota such as the main Minneapolis/St. Paul metro region and identified the scarcity of NPPC providers and resources in the other four corners of the state. It was surprising that despite having several health care systems in less populated counties, there was a paucity of information identifying CIH providers and services. This information should greatly assist stakeholders, especially lawmakers, in resourcing the underserved areas.
One of the major limitations of the project was locating accurate or reliable information from specific NPPC provider listings. In addition, directories of certifying boards and organizations often list information in a nonstandardized format that is not readily amenable for inclusion in the map. Some organizations list insufficient information for consumers to contact providers by only listing providers' name, phone number, and physical address. These listed phone numbers and physical addresses are often ambiguous from a consumer perspective and do not indicate whether the provided contact information is professional or personal.
In addition, it was challenging to identify the NPPC providers who have not highlighted chronic pain management as part of their credentials. Unlike the Minnesota Board of Medical Practice, which keeps a record of all certified physicians in the state in a standardized format, there is no central body that lists accredited or certified CIH providers. Each of these NPPC modalities have their own credentialing or certifying board that is not integrated with the MN Board of Medical Practice. Some listings are membership based, for example, in Psychology Today magazine, where psychologists can list their business and services for a fee. This process reduces or eliminates the visibility of those practitioners who do not pay for listing and the yearly maintenance fees.
Another limitation is the use of convenience sample of chronic pain patients, CIH providers, non-CIH medical providers, and insurance industry representatives to evaluate the usability of the map and website. Indeed, since the average education of the usability participants (n = 30) was relatively high—further efforts will need to assess the usefulness of the map and website in a more representative sample.
Provider listings change frequently with influx or departures of providers and there is currently no process for the NOPAINMN website to keep up with the dynamic nature of credentialing NPPC practitioners throughout the state. Maintenance and updating of the website, database, and research is time-intensive work and requires a dedicated team.
Feedback from the user survey indicates a desire for more information on the website such as having more content or graphics/pictures. A need for more filter options to narrow searches on the Resource Map to years of provider experience, subspecialties, insurance information, provider or clinic days and hours of operation, and provider rating/availability was also mentioned. This was acknowledged to be of importance, but including this additional information was beyond the scope of the project due to funding constraints, the dynamic nature of insurance coverage for major insurance providers, and the resources needed to offer scheduling options for over 17,000 providers in the state.
The dissemination of this map and website to patients, providers, health systems, insurance carriers, and lawmakers is a major opportunity to improve patient resources as well as their knowledge about treatment options. Specifically, the authors sought to raise access of NPPC services by publishing the map and to also raise public awareness by including a brief description, an evidence summary, and a video demonstration of each of the mapped NPPC modalities.
The authors contend that combined access and increased public awareness is needed to highlight the recommendations from the American College of Physicians and The Joint Commission guidelines that NPPC practices should be implemented before opioid prescriptions. Additional study is needed to turn these recommendations into best practices for NPPC CIH utilization.
Overall, the NOPAINMN map has been received with great enthusiasm by Minnesota as it addresses an unmet need for NPPC, thus creating a successful model for other states to follow.
Conclusions
The NOPAINMN website and resource map is an innovative project with Minnesota as the only U.S. state that has created this important resource for practitioners, patients, health care administrators, insurance companies, and policymakers. Although this project has uncovered health disparities regarding access to services for chronic pain management in MN, it has empowered the stakeholders with knowledge of NPPC CIH resources.
The NOPAINMN website is a dynamic database that needs to be consistently updated to maintain accurate information. Provider, health facilities, and health systems' information will need to be intermittently reviewed to ensure updated and accurate contact information and services provided. Going forward, educational materials, including evidence-based articles, resources, and modality descriptions, will also need to be intermittently and systematically reviewed for updated and accurate information. Updating these materials is essential as the research and evidence in the field of NPPC is rapidly growing.
Despite the limitations of the project, NOPAINMN has provided a learning opportunity for the state and the lawmakers who provided the funding through the Minnesota Department of Health. Ongoing funding and legislative commitment are needed to not only sustain and expand the mapping study, but also to make policy changes regarding insurance coverage for chronic pain patients. Funding to sustain a technical support team and subject matter experts is needed to maintain the website so that usability remains at a high level for all stakeholders. Further dissemination of the project, website, and the identified barrier and facilitator themes is also needed to bring the mapping study to the next level.
There are ongoing challenges and barriers such as access to and cost for NPPC CIH services for chronic pain patients that need to be addressed. The opioid epidemic is a significant public health crisis and utilizing NPPC practices as the first line of defense to treat chronic pain is a way to reduce the economic burden on the State of Minnesota.
The NOPAINMN project can be replicated by other states to eventually have an integrated network across the United States, which can be leveraged for improving clinical care, quality, and access for patients, and driving policy work for coverage of NPPC services.
Footnotes
Acknowledgments
This study was presented at the International Congress on Integrative Medicine and Health, May 23–26, 2022; Phoenix, AZ, and was partially published as an oral abstract in Global Advances in Health and Medicine, Volume 11: 1–142, which can be accessed at ![]() ">https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9471381 The Hennepin Healthcare NOPAINMN team thanks the following individuals for their expertise, assistance, and contributions throughout all aspects of the project: Chris Hansen, interactive design developer at Insource Media, for creating the website; Julie Watt at the Hennepin Health Foundation for their help in grant writing, and the Minnesota Department of Health program and grant staff: Dana Farley, Shelly Dieu, Liz Corey, and Mark Kinde.
">https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9471381 The Hennepin Healthcare NOPAINMN team thanks the following individuals for their expertise, assistance, and contributions throughout all aspects of the project: Chris Hansen, interactive design developer at Insource Media, for creating the website; Julie Watt at the Hennepin Health Foundation for their help in grant writing, and the Minnesota Department of Health program and grant staff: Dana Farley, Shelly Dieu, Liz Corey, and Mark Kinde.
Authors' Contributions
All the authors have accepted responsibility for the entire content of this article and approved submission. Conceptualization, methodology, writing, reviewing, editing, supervision, and funding by A.P. Methodology, reviewing, and editing by R.P. Original draft preparation, data curation, visualization, and editing by M.V. Original draft preparation and methodology by S.K. Methodology, writing, reviewing, editing, and supervision by J.A.D.
Author Disclosure Statement
Authors state no conflict of interest.
Funding Information
This project was funded by the Minnesota Department of Health (Grant number 178835).