
Abstract




Introduction
Personalized medicine in cancer is an emerging approach to patient care in which certain individual characteristics are used to guide therapeutic decisions. 1 Ultimately, the goal is to execute the right intervention for the right patient at the right time. In this era of personalized medicine, how does one effectively tailor the mind–body medicine (MBM) prescription for individuals with varied needs and circumstances who are on their cancer journey? Here, we propose guiding concepts and a clinical model for personalized MBM in cancer care. Furthermore, we frame practical clinical aspects for effective application of MBM in integrative oncology (IO) with shared decision-making between patient/caregiver and provider.
An Overview of MBM in Caring for People on a Cancer Journey
MBM is a diverse system of practices that focus on the interactions between the mind, body, and behavior to promote health and well-being. It emphasizes the integration of emotional, mental, social, spiritual, and behavioral factors to directly affect health outcomes. 2 –8 MBM incorporates Eastern and Western models, traditional and modern approaches, psychological and physical components through an evidence-informed lens. 5 Among these are meditation (i.e., body/breath awareness, mindfulness, loving kindness and compassion-based training, transcendental, etc.), movement or energy-based therapies (i.e., qi gong, Tai Chi, and yoga), relaxation techniques (i.e., diaphragmatic breathing, progressive muscle relaxation, guided imagery, autogenic training, etc.), and expressive and other practices (i.e., nature, dance, art, writing, and music therapy). 2
Meditation can take many forms, and is a critical component of MBM that most generally refers to any practice that involves self-regulation of attention in a sustained fashion, potentially allowing deepening states of concentration, tranquility or insight, broadening the field of awareness, and developing altruistic tendencies. 4,6 There are numerous types of meditation across cultures and time. One meditation that has been widely studied in the modern cancer health care setting is “mindfulness meditation,” often in the context of mindfulness-based stress reduction (MBSR) or mindfulness-based cancer recovery (MBCR) training. 9 Mindfulness meditation generally aims to develop an awareness of thoughts, emotions, and physical sensations in a kind, observant, and nonjudgmental manner.
MBM has shown beneficial short- and long-term impact on physical, psychosocial-emotional, and interpersonal well-being in the care of people on a cancer journey. Systematic reviews of randomized trials and meta-analyses suggest that MBM practices are helpful for cancer-related symptoms, for treatment-related side effects, in survivorship, and in end-of-life care. 10 –16 These benefits are due to multiple reasons. Laboratory, imaging, and clinical data show its impact on chronic stress level and inflammatory markers, cortisol/hormone levels, the nervous system, cognitive and emotional factors, immune function, cardiovascular parameters, telomere health, and epigenetics. 9,17 –20
A Snapshot of Current Evidence and Guidelines for MBM in Cancer Care
National practice guidelines by the American Society of Clinical Oncology, Society for Integrative Oncology, and the National Comprehensive Cancer Network now include MBM for active cancer care and in survivorship. 3,10,21,22 Guidelines for supportive care during and after cancer treatment incorporate meditation, yoga, stress management, and music therapy with other integrative therapies, including acupuncture, massage therapy, exercise, and nutrition.
MBM practices are recommended options in patients with cancer for cancer pain, fatigue, sleep disorders, anxiety, depression, fear of recurrence, cognitive dysfunction, sexual dysfunction, stress reduction, and quality of life. 3,21 –24 Several large meta-analyses and systematic reviews summarize the benefits with yoga, Tai Chi, and qi gong on emotional health, improved sleep, and fatigue in patients with cancer and survivors. 3,11,13,15,21 –24 The research continues to evolve, as studies begin to compare different cancer MBM therapies and consider moderating factors to predict outcome. 25
In addition, MBM can be applied in the context of groups (i.e., MBSR, MBCR, Center for Mind–Body Medicine, and Stress Management and Resiliency Training). 9,14,26,27 Group-based settings provide a venue to learn skills, connect with others, and gain broader insight to support the healing journey. Of interest, randomized trial data in cancer survivors suggest lasting specific and unique benefits of MBCR and mind-body medicine practices, beyond the effects of group support and sharing. 14 Furthermore, virtual delivery of MBM through meditation/well-being mobile applications and online interventions holds new promise for equitable access and delivery. 28,29
Insights from Contemplative Science Models for Personalizing MBM
Given the vast array of MBM practices for patients with cancer, how does the IO provider tailor a prescription for an individual? It is complicated, since the interventions require the patient, and perhaps caregiver, to be active participants in a longitudinal learning process. This requires time, effort, resources, and sustained interest. While the complete answer remains elusive, thoughtful models in the contemplative and neurosciences literature may serve as guideposts in IO.
MBM models: attentional, constructive, deconstructive, and embodied
One theoretical model defines families of meditation styles as “attentional,” “constructive,” and “deconstructive” reflecting wisdoms and growth that may arise with various practices. 30 –33 Attentional practices can include focused attention (FA) and open monitoring (OM). 30 FA (sometimes termed “concentrative” or “single-pointed” meditation) may be a starting point. In FA training, one learns to place the focus of attention on a chosen object (e.g., breath, candle flame, sound, image, mantra). Once familiar, a meditator may progress to OM (sometimes termed “awareness meditation”), in which they attend to any experience that might arise in the moment, without selecting or judging. In OM, one may strengthen stability of attention, awareness, and nonreactivity, facilitating a healthier state for the person along the cancer journey.
Constructive styles of practice (“loving-kindness” and “compassion”) may incorporate elements of FA and OM to encourage self-kindness, build prosocial behavior, and facilitate positive reappraisal and compassionate action. For patients with cancer and their caregivers, constructive MBM practices can help deepen compassion and gratitude within, as well as extend it to others. 4,30 –33 The deconstructive family of MBM practices may elicit existential insight and generate knowledge through self-inquiry. These learnings may profoundly resonate with and support people on a cancer journey, often through nondual perspectives, and an acceptance of our impermanence and interconnectedness.
Additional other categories of common mind–body practices include “expressive” meditation (i.e., dance, art, writing, and music) and “movement” or energy-based meditation (yoga, Tai Chi, and qi gong). 26 In expressive/movement meditation one moves through an embodied experience to integrate physical movement, breathing, emotion, and somatic awareness. Such practices may be a way to increase accessibility to MBM in cancer care, especially if a seated/still practice is difficult due to pain, fatigue, traumatic re-experiencing, or rumination.
Different patients will have different world views. They may seek and gain different attentional, constructive and deconstructive insights from mind–body practices. Thus, it is helpful for the cancer clinician to elicit and understand the natural inclination, intentions, and ability of the patient. This, in turn, better guides the MBM prescription.
Developmental-stage model of meditation and mind–body practices
Building from prior models, Schoenberg and Vago introduced a developmental-stage model for meditation to reflect the complexity of the mind–body–brain dynamics. 30 In brief, the first stage is “neuro-visceral integration” in which the mind–body is stabilized for more rigorous mind-oriented meditative practice. It is conceptualized as a continuum from “relaxation” practices to “embodied” practices, reflecting body-oriented practices that were traditionally preparatory for sitting meditation.
The second stage is described as “concentration practices” characterized by training the mind using stable (FA) and/or flexible scope (OM). The next two stages of “insight” and “non-dual” practices serve to integrate more abstract contemplative practices for ordinary and extraordinary insight into the nature of self, mental habits, and self-transcendence. The final stage, termed “unified compassion practices,” describes a concrete understanding of ultimate reality where one's formal practice transforms into everyday living, integrating the preceding tiers and insights. This state is characterized by the direct experience of altruistic motivations for compassionate action, service-to-others, and unconditional love.
Developing a Clinical Model of Personalized MBM in IO
The framework of the contemplative models along with practical clinical experience serves as groundwork for personalizing MBM for an oncology patient or caregiver. Patient preference and shared decision-making must be at the foundation of any exploration, as the patient must endorse and implement changes for its clinical utility. 25
A clinical adaptation of the common MBM models, meditational families, and developmental stage model for personalized MBM in cancer care is shown in Figure 1. This adaptation is meant to spur thought on how we may continue to translate theoretical/research models to the IO practice. We describe hereunder a few key illustrative features.
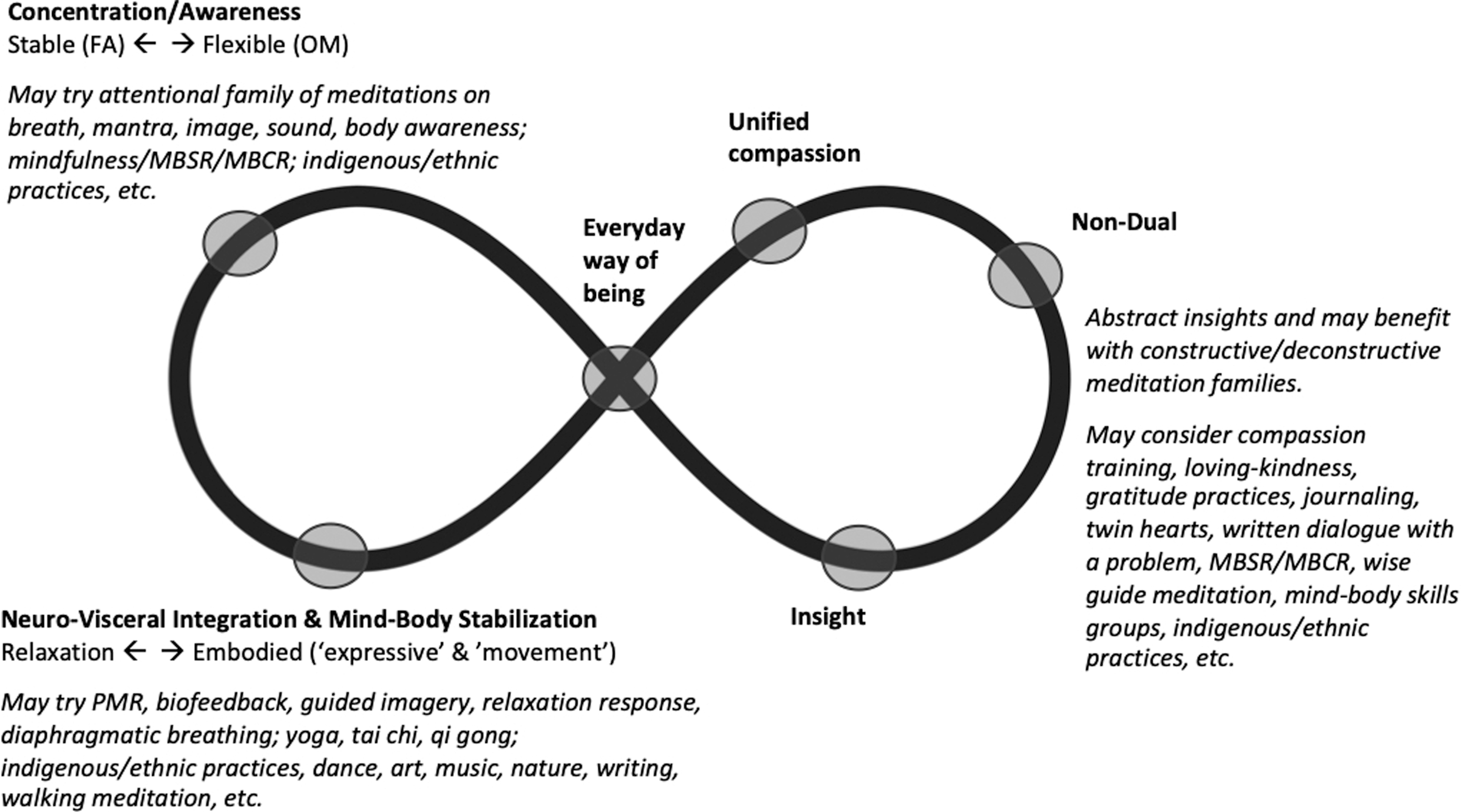
Adapting theory to a clinical model—informing personalized mind–body medicine for people on a cancer journey (clinical adaptation from the developmental-stage model, Schoenberg and Vago). 30
First, the personalized MBM model is imagined as an infinity sign. As an adaptation of the original developmental-stage model, we draw the stages along the path of this sign rather than a step-wise function. 30 Insights may not progress systematically in a staged manner for an individual patient or IO practitioner. Hence the infinity sign attempts to acknowledge learning through the steps as a fluid journey, which reflects also the personal experience for one of the authors and her patients (K.K.M.). Multiple concrete and abstract practices may be explored over time, and personal growth may develop in a flexible fashion due to variable contexts, MBM practices, and life events.
Second, the illustrative model shows the complex nature of prescribing and adapting MBM models for any individual patient on the cancer journey. For example, from a physical symptomology and psychosocial context point of view for a patient with cancer, relaxation-type of MBM practices or embodied practices may be helpful in the neuro-visceral integration and mind–body stabilization stages. Attentional family meditations may be effective for concentration/awareness stage of learning. The “insight” and “non-dual” practices serve as more abstract practices and may welcome insights from constructive and deconstructive families of MBM practices, such as meditation trainings in compassion, loving-kindness, gratitude, and other contemplative practices.
Indigenous and ethnic practices are a complicated aspect of our cultural responsiveness to the history of meditations across space and time. These have a critical place in the discussion as well. All MBM practices may provide insights into any of the developmental stages.
Third, this clinical personalized MBM model highlights the concept that this prescription is not temporary. Instead, the focus is to unify practice and daily living: to think, eat, breathe, love, act and live mindfully and heartfully. Hence the center of the infinity sign is drawn to serve this idea of an insightful, open, mindful, and meditative “everyday way of being.”
Framing the Clinical Prescription
A conceptual framework to apply the theory to practice is described in Table 1. The recommendations are drawn from the theoretical models alongside practical experience with patients in the cancer clinic. We describe critical elements of understanding the needs, barriers, patient and provider preferences, and psycho-sociocultural context in shaping an effective MBM prescription. The impact of group practices is important, with the growing understanding of social common therapeutic factors with instructor-led group-based practice, such as sense of belonging, validation, hopefulness, and alliance. 34 Interest and openness to trial and error are essential. What works for one patient, may not for another; what resonates on one day of practice, may not on the next.
Framing the Clinical Prescription and Practical Aspects for Personalized Mind–Body Medicine in Integrative Oncology
MBM, mind–body medicine; MBSR, mindfulness-based stress reduction; MBCR, mindfulness-based cancer recovery.
MBM for an oncology patient should be approached thoughtfully, especially in the context of trauma, mobility issues, energetic implications, childhood adversity, and psychological underpinnings. 35,36 Meditation-related adverse events (MRAE), such as anxiety, traumatic re-experiencing, and emotional sensitivity, have been noted. Interestingly, study participants with MRAE have reported being equally glad to have practiced meditation as those not reporting MRAE. 35 Risks can be reduced by identifying relevant factors, using trauma-informed care, and working with qualified experts. Applying personalized therapeutic approaches, MBM can provide a healthy model for experiencing and coping with adversity on the cancer journey. 37
Conclusion
“What you practice grows stronger.” 38
MBM for people on the cancer journey is an invitation to awareness, inner wisdom, and personal growth. It is an invitation to physical, psychological, social-emotional, and existential insight. It is an invitation to attentional, constructive, and deconstructive wisdoms. It is an invitation to strengthen the mind and body and promote healing. For IO providers, our goal is to help intuit a right intervention for a right patient at a right time, informed by the evidence base, for personalized MBM in cancer care.
Footnotes
Author Disclosure Statement
At the time of publication, Dr. Vago is also the research lead for the profit company, RoundGlass. For all others, no competing financial interests exist.
Funding Information
No funding supported the work associated with this article.