
Abstract
Introduction:
Complementary and integrative health (CIH) modalities promote overall health and well-being and can be beneficial for individuals with a range of conditions. Traditionally, CIH has been delivered in person. COVID-19 created a need to identify sustainable remote delivery options to assure access to CIH while practicing public health recommendations. This scoping review maps the opportunities and challenges to remotely delivered CIH.
Materials and methods:
A scoping review was conducted between June 2020 and October 2020 using the following search engines: PubMed, Academic Search Premier, PsycINFO, CINAHL, Cochrane Reviews, and the Cochrane Clinical Trial Collections. Search results investigating remote CIH delivery were restricted to articles written in English, published after 1990.
Results:
Of the 10,884 articles identified, after review for content and methods, 330 articles were included. Most articles were randomized controlled trials (n = 170), applied mindfulness (n = 203), and targeted mental and behavioral health conditions (n = 182). Interventions were primarily delivered through mobile applications (n = 151) and web-based platforms (n = 86). Most commonly reported barriers were adherence (n = 24), resource requirements (e.g., time and space) (n = 23), and technology-related issues (n = 21). Although most studies did not report facilitators (n = 217), most commonly reported facilitators were social and technologic supports, accessibility, usability, perceptions, and rewards. Participant outcomes measured were broad and included movement (n = 88), stress (n = 68), and pain (n = 54). Intervention characteristic outcomes most often measured were satisfaction and usability (n = 5).
Conclusions:
This scoping literature review identified many articles addressing remote delivery of CIH, but few reporting on the implementation of remotely delivered CIH. Findings suggest remotely delivered CIH, specifically mindfulness and meditation-based modalities, is a viable treatment option for a diverse range of health conditions. Feasibility studies and larger sample sizes are recommended to strengthen the scientific evidence.
Introduction
Complementary and integrative health (CIH) modalities promote overall health and well-being and can be beneficial for individuals with a range of conditions. 1 –5 Where “conventional” refers to mainstream Western approaches to medicine, nonmainstream approaches used in conjunction with conventional medicine are considered “complementary.” 6 Complementary modalities include acupuncture; meditation and mindfulness activities; hypnosis; chiropractic; massage and other body work-based techniques; yoga; Tai Chi; qigong; and biofeedback. “Integrative health” brings conventional and complementary approaches together in a coordinated way.
Traditionally, CIH modalities were delivered in-person, often with “hands-on” approaches and there is a vast knowledge of CIH outcomes based on in-person delivery. 7,8 The COVID-19 pandemic created a priority to identify sustainable means of remotely delivering care to ensure patient access to services while reducing contact. The priority to remotely deliver care poses unique challenges and opportunities for delivering CIH modalities. 9 The unique contribution of this article to the literature is the focus on the virtual delivery of CIH, given the need for remote access in the current pandemic climate.
CIH represents many heterogeneous modalities. 7 To further complicate matters, these modalities have demonstrated the capacity for remote delivery using a multitude of approaches. Research on CIH has been proliferating for the last 30 years, including the conduct of randomized controlled trials and systematic reviews in a variety of populations of video and audio resources, including telephones, telehealth, and mobile applications, making comparison of findings across studies difficult.
There is a gap in the literature on the identification of best practices, barriers and facilitators, and relevant outcomes in remotely delivering CIH—as this is an emergent approach to delivering CIH. Adding to this body of knowledge can inform efforts to ensure CIH modalities are accessible to patients, particularly in a climate where remote delivery might be a necessity (i.e., pandemic).
Heterogeneity among CIH remotely delivered interventions, coupled with the lack of adequate reporting, made conducting a systematic literature review of the effectiveness of remotely delivered CIH interventions not feasible, as such, the authors opted to use a scoping literature review. 10 The goal of this scoping review is to map the current literature on the use of virtual health resources (VHR) to remotely deliver CIH, and the opportunities and challenges. This article does not attempt to address the efficacy or effectiveness because they did not limit their search to a scoped body of literature with comparable outcomes.
The authors performed a broad review of this literature to be able to characterize the scope of remote delivery of CIH modalities, including the health status of populations under study, the technologies and methods used, feasibility of remote delivery of CIH, and the facilitators and barriers of the different approaches. The comprehensive breadth of the review, including asynchronous and synchronous approaches and projects including both remote and in-person delivery components, was intended to fully assess the opportunity for leveraging use of VHR to make CIH more accessible. From this review, the authors identified the best practices and promising policies in remote delivery of CIH. Information from this scoping review will inform the development of future research intervention protocols that build on the findings to address the current gaps in the literature.
Materials and Methods
Study design
The authors conducted a scoping review 10 to map the scope, feasibility, relevant patient and delivery outcome measures, and recommendations for remote delivery of CIH programs using VHR. To establish a broad net for their scoping review, they included a broad definition of CIH and multiple methods for delivery with no limitations on the study design, condition, or health status under investigation, as the intent was to gather information that could benefit future implementation of remotely delivered CIH programs. This scoping review was part of a larger program evaluation that was determined by the local VA Research and Development Service to be a quality improvement project, and thus not subject to the institutional review board review for research.
Search engines and terms
Searches were conducted using the following search engines: PubMed, Academic Search Premier, PsycINFO, CINAHL, Cochrane Reviews, and the Cochrane Clinical Trial Collections. Search terms were refined by investigator discussion, initial search results, and keyword review from relevant articles. Multiple searches were conducted using combinations of search terms to obtain as broad a review of the literature as possible. Search terms included the following for CIH modalities: “acupressure,” “acupuncture,” “meditation,” “transcendental meditation,” “mindfulness,” “repeated mantras,” “mantras,” “hypnosis,” “hypnotherapy,” “guided imagery,” “imagery, psychotherapy,” “relaxation therapy,” “chiropractic,” “massage,” “healing touch,” “therapeutic touch,” “yoga,” “tai chi,” “qi gong,” “Pilates,” “movement therapy,” “breathing exercise,” “progressive muscle relaxation,” “autogenic training,” “biofeedback,” “Feldenkrais,” “alexander technique,” “rolfing,” “trager,” “whole health,” “holistic health,” “complementary therapies,” “integrated medicine,” “integrated health,” “mindbody therapies,” or “complementary integrative health.”
Search terms for remote or virtual delivery included the following: “virtual,” “telehealth,” “remote,” “self-directed,” “electronic delivery,” “information technology,” “applications,” “apps,” “mobile,” “mobile health,” “e-health,” or “m-health.” Generic or specific terms for CIH modalities were always used in combination with terms describing a remote or virtual delivery. Reference lists from relevant systematic reviews and meta-analyses on CIH were searched for articles not previously identified in the database searches. In addition, a publication list maintained by a VA-affiliated CIH evaluation center was also searched for relevant articles. Searches were conducted between June 2020 and October of 2020.
Search and screening procedure
Each search was conducted by a single reviewer, with two authors (A.C.A. and E.J.B.) and a VA librarian conducting separate searches. Search results were uploaded to a digital platform to facilitate systematic reviews 11 to assist with deduplication, screening, and full-text review. Screening of articles for inclusion and exclusion criteria was conducted by five reviewers. For each article, the title and abstract were screened by one reviewer to determine whether they met the inclusion criteria for the review. For articles where the reviewer was uncertain whether they met the criteria, the articles were discussed by all reviewers and inclusion/exclusion was determined by consensus.
Inclusion/exclusion criteria
After duplicates were removed, titles, abstracts, and methods were searched to confirm the virtual or remote delivery of one or more of the CIH modalities included in the search terms described above. This included programs that combined in-person and remote delivery, if the remote delivery involved some VHR (e.g., video, mobile app, website). Search results were restricted to peer-reviewed articles published in English after 1990 and involving only human populations. No age restrictions of the studied population were applied, as the goal was to perform an expansive review including any potential remotely delivered modality, regardless of whether it was in children or adults. There were also no restrictions on the study design or the condition or health status of the population under study.
Studies were not limited to fully synchronous or asynchronous delivery and could include aspects of both. In addition, studies could include multiple CIH interventions as well as both CIH and non-CIH interventions. Full-text articles that were not available through subscriptions at either the facility VA library or the affiliated university libraries or were not available through interlibrary loan were excluded (n = 8) (Fig. 1).

PRISMA. This diagram shows the systematic process the authors followed to include articles captured by this search.
Data collection
A custom data extraction sheet was developed and used by all reviewers for full-text reviews. Data extraction included the title, first author, publication year, journal, study population, the condition(s) under study, study design, CIH modality, type of remote delivery (i.e., website, mobile app, video), intervention details, any noted barriers or facilitators, and outcomes. While the authors extracted data on outcomes, this was not to evaluate efficacy, but to obtain information that could be useful for future implementation efforts. Since comparison of synchronous versus asynchronous delivery or fully virtual versus hybrid studies with some in-person components was not a specific objective of this study, they did not extract data specifically to be able to compare outcomes of these delivery types.
Data analysis
Once data extraction was complete, results were organized in a Microsoft Excel spreadsheet for review. Results were grouped by the type of remote delivery and summarized according to the CIH modality, publication year, conditions, and outcomes.
As there were no inclusion criteria for the conditions, there were a wide variety of conditions or patient populations included in the articles. The authors used the International Classification of Diseases, 10th Revision (ICD-10) codes to categorize conditions. A full list of the articles included in the review is given in Supplementary Appendix A.
Results
Of the 10,884 articles identified, after review for content and methods, 326 articles were included. Table 1 shows the frequency of study designs in the included articles. The majority (51.8%) of the articles reported results of a randomized controlled trial, followed by before-after (20.6%) studies looking at change pre- and post-intervention, and formative (16.0%) studies that examined the development, feasibility, and acceptability of a CIH intervention.
Study Design of Articles Included in Scoping Review
Mental, behavioral, and neurodevelopmental conditions were the most common (54.9%) conditions addressed by the interventions in the included articles. Cognition and emotional state (29.4%), and conditions of the nervous system (21.5%) were the next two most common conditions (Table 2).
Types of Conditions or Health Topics Included in Articles
Frequencies represent the number of articles that examined the condition. Percentages do not add to 100% since articles could include multiple conditions.
Table 3 displays the technologies used for the intervention or content delivery by the CIH modality. For mindfulness, meditation, biofeedback, guided imagery, and acupressure/acupuncture, mobile applications were the most common VHR used. Compact discs (CDs) or digital video discs (DVDs) used to deliver audio or video files were the most common VHR used for yoga, hypnosis, massage, Tai Chi, qigong, and Pilates. For progressive muscle relaxation, telephone and CD/DVD were tied as the most common technologies used. Another common VHR used across the CIH modalities was a website.
Virtual Health Resource Used for Intervention or Content Delivery by Complementary and Integrative Health Modality
Frequencies in parentheses after the complementary and integrative health modality name represents the number of articles that utilized that modality. Modality frequencies do not add to the total number of included articles (n = 329) since articles could include more than one complementary and integrative health approach.
Frequencies for each virtual health resource may not add to the modality frequency since multiple virtual health resources could be utilized in a single study. Percentages are calculated per modality using the modality frequency as the denominator.
CD, compact disc; DVD, digital video disc.
Outcomes measured in each study that were identified by the authors and collated during data extraction are shown in Figures 2 and 3. Not all articles identified outcome measures (e.g., protocol publications). Outcome measures and results varied across publications. Outcome measures were categorized into participant outcome measures and intervention characteristic outcome measures. The most common participant outcome constructs measured included movement (n = 88), stress (n = 68), and pain (n = 54).

Participant outcome measures. This graph shows the number of articles reporting each of the participant outcome measure constructs listed on the left of the graph (y-axis).
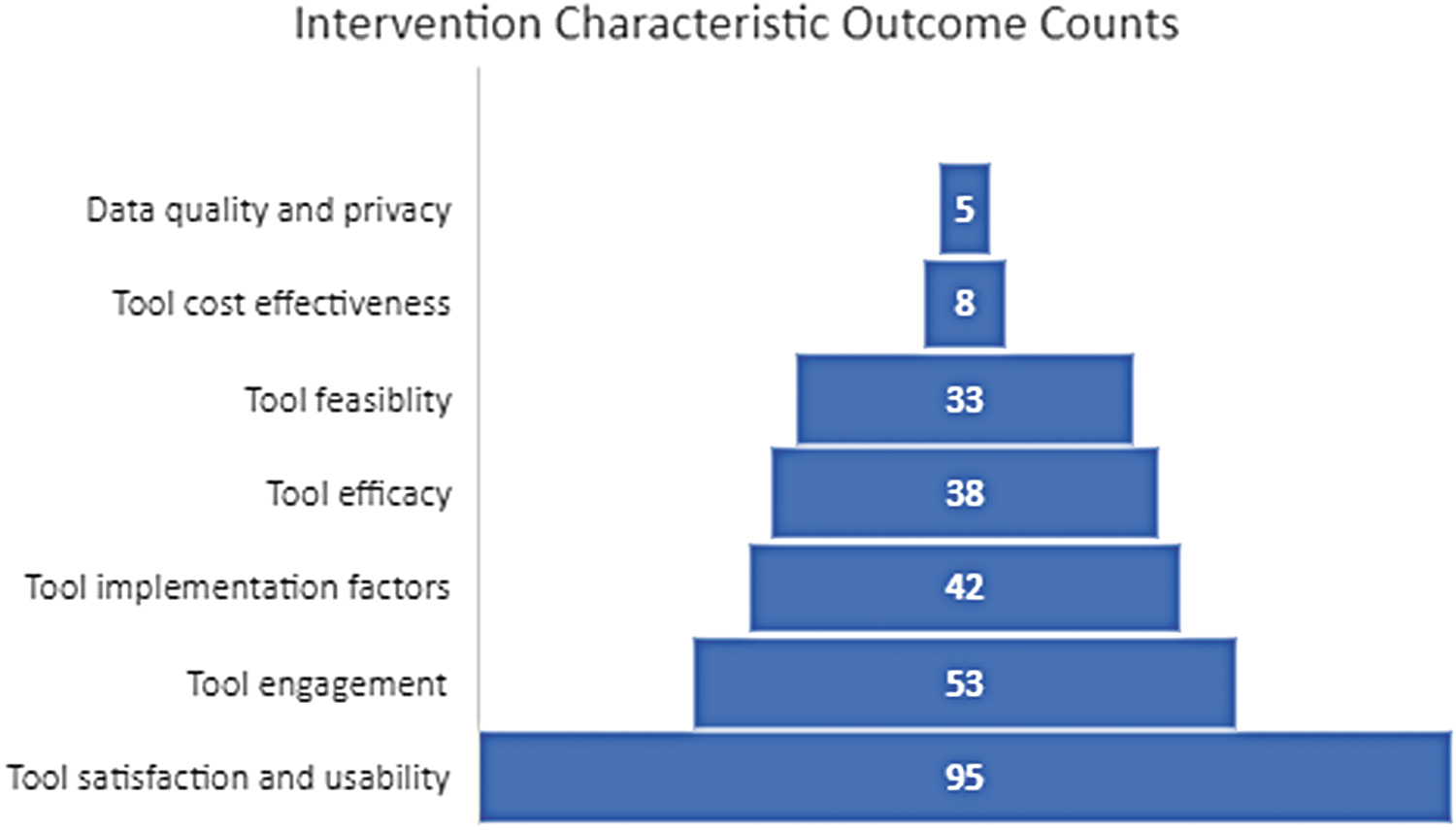
Intervention characteristic measures. This graph shows the number of articles reporting each of the intervention characteristic measure constructs listed on the left of the graph (y-axis).
Each construct collates several subconstructs (e.g., balance, stress awareness, pain interference). The construct of movement included a variety of subconstructs including activity tolerance, 12 balance, 13 and physical function. 5 The construct of stress included measures of stress, 14 burnout, 15 and relaxation. 16 Of the publications measuring pain, only one 17 measured more than two subconstructs (e.g., pain intensity, pain catastrophizing, and pain interference with activities) of this complex construct. Outcomes were assessed in a variety of ways and may have been assessed quantitatively with validated measures or qualitatively, capturing participant experience.
Intervention characteristic outcomes were less often assessed. The most common characteristic measured was satisfaction and usability (n = 95). This characteristic included reported usefulness, user friendliness, and experience while engaging with the tool. Intervention engagement was often measured as time spent with the intervention (e.g., minutes per day), retention through study protocol, and sessions attended. Few publications reported on the feasibility, cost effectiveness, or data quality. Four publications did stand out as assessing a range of intervention characteristics such as satisfaction and usability, feasibility, and cost effectiveness. 18 –21
A primary aim of the scoping review was to synthesize the findings relevant to the facilitators of the implementation of remotely delivered CIH. Considering most included studies did not assess implementation feasibility, there were times when facilitators were not specifically author identified. In these instances, reviewers then identified facilitators of virtual implementation of CIH modalities.
Of the articles selected for this scoping review, the majority did not provide insight into facilitators of the virtual implementation of CIH modalities (n = 217; 66.3%). Synthesis of the remaining articles resulted in the identification of facilitators across five categorizations, which include social and technologic supports, accessibility, usability, perceptions, and rewards.
The categorization with the most identified facilitators in the article synthesis was categorized as supports. Facilitators within the support category varied, with the most common form of support abstracted being social support, which comprised in-person 22 or online group meetings 23 as well as one-on-one interaction with a CIH implementor. 24 Supports also included technologic reminders to encourage engagement in the remote CIH modality such as automated and live text messages, 25 e-mails, 26 phone calls, 27 and notifications. 28 Although reported less often, the use of tracking features that include daily logs 29 and employer initiatives 30 that support the use of remotely delivered CIH were also included.
The second-most frequently identified facilitators were categorized as factors related to accessibility. Studies cited the availability of content 24-h a day 31 or access to the intervention after the study, 32 which afforded study participants the opportunity to engage in their CIH at a time of their convenience. In addition to content availability, the delivery method 31 of the CIH was also cited as a facilitator since mobile applications and online formats are now ubiquitous and thus accessible for most individuals. Another factor related to accessibility was no or low cost of the remotely delivered CIH. 33
The third category was usability, and article synthesis revealed CIH modalities deemed easy to use, 34 simple, 35 and usable for diverse populations 36 while a gamified nature 37 facilitated the remote utilization of CIH among participants. Perceptions of the CIH users also served as facilitators. Although less commonly abstracted from the included studies, perceiving the remote CIH as secure, 38 permitting self-direction, 39 satisfaction, 28,40 and acceptable 41 facilitated the implementation and utilization of the remote CIH. The least commonly reported facilitator was the provision of incentives in the form of money, gift cards, or even extra credit college courses facilitated the implementation of remote CIH.
Barriers to successful implementation that were identified by the article authors or by the reviewers during data extraction are shown in Table 4. Not all articles had an identified barrier, as most of the articles were not specifically designed to address feasibility. Of the barriers identified, the most common were low adherence or participation (26.4%), 40 synchronous and/or in-person components that added additional constraints, such as travel, time, and space (25.3%), 42 technical difficulties with the VHR used to deliver the intervention (23.1%), 43 technical requirements that limited adoption (such as broadband internet or requiring a particular smartphone operating system; 14.3%), 44 and condition-specific barriers, such as fatigue or embarrassment, that contributed to dissatisfaction or inability to complete the intervention (11.0%). 35
Barriers to Implementation
Frequencies represent the number of articles among those where at least one barrier was reported. Percentages do not add to 100% since articles could contain multiple barriers.
For some studies where participant feedback was obtained, participants reported that there were aspects of the intervention that they did not like, such as the voice used during content delivery, or the background music chosen (11.0%). 45 Additional barriers identified for remote synchronous delivery included instructor time and scheduling conflicts (5.5%). 46
Table 5 shows the most frequent limitations of the included studies that were noted during review. The most frequently identified study limitations were small sample size (46.1%), lacking generalizability (20.6%), high attrition (17.2%), possible selection bias (15.6%), and lack of or unsuitable control group for comparison (15.0%). Other common limitations included a short duration of follow-up (6.1%), self-reported outcomes or compliance with the intervention (5.6%), a lack of assessment of adherence by the study investigators (5.0%), and a short duration of the intervention (4.4%).
Most Frequently Identified Study Limitations
Frequencies represent the number of articles among those where at least one limitation was identified. Percentages do not add to 100% since articles could contain multiple limitations.
Discussion
This article presents the findings of a scoping review to identify the current state of implementation of remotely delivered CIH programs including implementation facilitators, barriers, and study outcomes. Although beyond the scope of this review, findings reflect the literature of in-person delivery of CIH with studies evaluating CIH as a treatment for diverse populations. A summary of data findings suggests that most articles were randomized controlled trials, applied mindfulness-based CIH modalities, and targeted mental and behavioral health conditions. Interventions were primarily delivered through mobile and web-based applications; outcomes measured were broad and included movement, stress, and pain; and intervention characteristic outcomes most often measured were satisfaction and usability.
Most reported barriers were adherence, resource requirements (e.g., time and space) and technology-related issues. Although most studies did not report facilitators, most reported facilitators were supports, accessibility, usability, perceptions, and rewards. Findings suggest that remotely delivered CIH, specifically mindfulness- and meditation-based modalities, is a viable treatment option for a diverse range of health conditions. Data findings inform recommendations to advance the state of the science of delivering CIH with VHR.
These scoping review data findings present evidence of both variety and rigor of study designs. Although randomized control trials are the gold standard for evidence, 47 when building the science of a particular intervention (i.e., remotely delivered CIH), formative evaluations are warranted before conducting randomized control trials. 48 Increasing the number of formative evaluations will help to improve the quality and effectiveness of remotely delivered CIH programs and could help to identify and alleviate potential barriers. Many of the studies in this scoping review reported small sample size as a limitation to their design.
Mental and behavioral health conditions are well known to be amenable to CIH programming. 49 –52 These findings reflect this in that more than 50% of the studies focused on these important health conditions. Beyond mental and behavioral health, studies focused on the gamut of conditions from every ICD-10 category from cancer to pregnancy. This finding suggests that remotely delivered CIH is a viable treatment option for diverse health conditions. While the scope of this review was limited to virtual delivery of CIH, it should be noted that this finding mirrors the literature of in-person delivery of CIH with studies evaluating CIH as a treatment for a wide variety of conditions and populations. 7,8,53 –57
Most studies were focused on mindfulness and meditation. This is likely due to the availability of mindfulness- and meditation-based programs and the ease of program implementation. For example, the ready availability of commercial mindfulness apps that can be easily downloaded from an app store provides an accessible, portable, and efficient means of testing mindfulness as a therapy for a variety of conditions. 58 –63 The emphasis on the use of VHR to deliver mindfulness and meditation is interesting considering that the most reported measured outcome was movement.
VHR used for delivering the CIH programs varied by CIH modality, most often using the efficient and portable mobile application. Mobile applications are readily developed and can provide accurate data to track participant engagement and progress, but more formal testing is needed. 64 Surprisingly, the majority of remotely delivered movement CIH (i.e., yoga, qigong, Pilates, Tai Chi, massage, hypnosis) used CD/DVDs as opposed to the more adaptable mobile application. CD/DVDs may be the VHR of choice for these CIH as they may be played on a television screen that is largely visible even when in varied positions required for a movement practice. In addition, this may also reflect the historical availability of exercise videos that could be applied to CIH movement-base interventions. Similarly, progressive muscle relaxation was most often delivered via CD/DVD and telephone.
Many of these programs used more than one VHR. For example, participants may receive a CD/DVD with video education for their desired CIH modality and a weekly telephone call to assess program engagement and answer questions. Mobile, web, and CD/DVD tend to be more commonly used, but telehealth, virtual reality, and wearable devices are gaining popularity and have been more accessible in recent years. One notable finding was the relative lack of web conferencing, although this option could be feasible for increasing accessibility. The use of virtual tools to deliver CIH improved access to CIH; however, some touch-based modalities such as acupuncture, acupressure, chiropractic, professionally delivered massage, and professionally facilitated hypnosis did not emerge as feasibly delivered CIH modalities.
Reported outcomes measured in this data set were varied. Movement was the most common type of reported outcome. Movement included balance, range of motion, stress incontinence, and others. Many CIH programs aim to improve movement, and so, this finding was not surprising. Studies took care to measure pain and all its permutations such as pain intensity, pain catastrophizing, pain interference, daily pain, and average pain. The authors found the limited number of studies reporting measure of “breathing and breathing signals” and “attention and focus” to be interesting given the importance of both breath work and focus in many CIH programs, including mediation, mindfulness, Tai Chi, qigong, and yoga. Breathing and breath are important aspects of several modalities (e.g., meditation, yoga) and were rarely measured. This may be due to the difficulty in measuring such things remotely.
More research is needed to assess the efficacy of a given VHR with a given modality. Due to the number of modalities used and the number of VHR, it is beyond the scope to conclusively synthesize outcome results.
The relatively recent increase of remotely delivered CIH programs has led to many studies and publications, and more are to be expected with the onset of COVID-19. However, although the application of formative evaluations remains critical, the current literature is lacking in this evaluative approach. Although some studies looked at these qualities, few (n = 33) reported assessing feasibility, a first step to successful implementation. Even fewer reported assessing cost effectiveness or data quality of the varied CIH programs. Cost effectiveness is key in garnering fiscal support for new programming. Quality data are imperative in being able to accurately investigate programming outcomes. Additional work would benefit from including these outcomes in remotely delivered CIH programming studies and publications.
Barriers to successful implementation of remotely delivered CIH programs were most often reported as low adherence or participation (i.e., engagement), resources, and technology-related issues. Research has shown that reminders, prompting, and accountability all improve engagement in remotely delivered interventions and is consistent with the scoping review finding supports, which, include reminders, act as a facilitator in CIH engagement. Formative evaluation of new programs may be able to discern which type of intervention or program component will improve engagement for a given implementation.
Future efforts to employ the VHR to deliver CIH should employ facilitators, including supports, accessibility, usability, perceptions, and rewards. Although not a main finding, another facilitator identified in the review included the gamification of interventions. Gaming components have also been noted as key in improving engagement. Including any of these components will likely increase the successful implementation of new programs. As the intent of this review was to better understand the broad scope of remote delivery of CIH, there was a wide degree of heterogeneity in the methods and approaches used by the studies included in this review, including synchronous and asynchronous delivery, and studies with hybrid in-person and remote delivery. The effects of these differences in delivery should be objectively compared in future research.
The scope of this article is limited to the delivery of CIH using VHR. The authors recommend that in-person delivery of CIH be addressed in subsequent scoping reviews. To strengthen the scientific evidence on remotely delivered CIH, future research should also address feasibility, include larger samples, and standardize outcome measures.
Limitations should be considered when inferring results. First, since their review did not limit to specific conditions, CIH or VHR, the authors are not able to comment on the effectiveness or efficacy of virtual delivery of CIH. The volume and heterogeneity of these works precluded the ability to synthesize specific outcomes. What they did review and synthesize were the measures of outcomes. Second, the authors limited the review to English-language articles and therefore do not have a representation of all literature published in other languages. The authors also did not include gray literature. Third, although they included a broad time range (January 1990 to October 6, 2020), due to the pandemic there is very likely a surge of literature that will come from the COVID onset. However, this body of work provides a foundation for continuing these efforts.
Conclusions
This scoping literature review identified literature reporting on the implementation of remotely delivered CIH. Findings suggest that remotely delivered CIH, specifically mindfulness- and meditation-based modalities, is a viable treatment option for a diverse range of health conditions. Although mobile applications, CD/DVDs, and websites were most commonly used for remote delivery of CIH, the recent explosion of use of web conferencing applications during the COVID-19 pandemic for remote meetings is another viable option for further evaluation—although, since much of the literature the authors evaluated predated the COVID-19 pandemic, they did not find this used frequently. Formative evaluation and feasibility studies are needed to discern the value of attempting implementation on a larger scale. Larger sample sizes are needed to account for small differences and demonstrate statistical significance in findings.
In addition, the authors recommend standardization of outcome measures, including all collected outcomes in publications to include “negative” findings, to inform the strength of evidence for remotely delivered CIH. There are several means for delivering CIH remotely, each warrants consideration when addressing implementation of remotely delivered CIH. The type of VHR that works best is the CIH modality itself, and a combination of different technologies can be used to best implement the program successfully. The body of knowledge clearly indicates the feasibility of delivery of CIH remotely using VHR, which presents itself as a necessity in the current global pandemic climate, and an opportunity to expand accessibility of CIH to remote populations.
Footnotes
Acknowledgment
The authors express their gratitude to Rachel Benzinger and Marilyn Teolis for their contributions in bringing this article to fruition.
Authors' Contributions
J.N.H. made substantial contributions to the conception and design of the work as well as the writing of the article. A.C.A. led data collection and analysis and contributed to writing of the article. E.J.B. and J.M.G. made substantial contributions to data collection and analysis and contributed to writing of the article. C.M. contributed to the data collection and analysis and the writing, editing, and submission of the article. J.M.P. contributed to the conceptualization of the work. All authors have approved the submitted version of this article. All authors have agreed both to be personally accountable for the author's own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for this project was provided by Whole Health Service, James A. Haley Veterans' Hospital.
Supplementary Material
Supplementary Appendix A
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.