
Abstract
Unaddressed grief and trauma may precipitate and maintain problematic substance use, criminal behavior, and resultant incarceration. We detail the implementation and evaluation of an evidence-based grief support group model conducted in seven groups in the two substance-use disorder treatment programs within a state correctional facility. The three aims of this project were to (1) train Department of Corrections mental health clinicians in the grief support group model, (2) conduct seven grief support groups facilitated by trained clinical social workers in two substance-use disorder treatment programs within the prison, and (3) evaluate impact of the grief support group model on participant grief. This is a pragmatic intervention feasibility evaluation of 69 incarcerated people in seven grief support groups facilitated by prison mental health clinicians trained in the grief support group model. The investigation resulted in high satisfaction and self-efficacy among clinician trainees, research feasibility being established, the intervention being found acceptable and practical, and client participants reporting clinically significant reductions in grief severity and grief improvement. The grief support group model holds promise as a complementary modality within a well-designed therapeutic program at the proper time for clients with severe grief.
Introduction
Death is the most natural and inevitable of human events, yet few are prepared for the loss of someone close. Grief is understood to be a normal reaction to loss and an essential part of dealing with loss—especially loss by death. When we discuss grief, it is important to understand that grief is universal in that every person will experience it at some time and also unique in that every person will experience grief in their own way.
Many factors contribute to constructive processing of a death toward integrated grief, that is, the permanent adaptation to the loss in which function is restored and satisfaction with the ongoing life is possible (Shear et al., 2013). Many factors can derail this normative process, including the nature of the death, traumatic exposure to the death, multiple losses close together, loss of one’s most important person, lack of supportive people, health and mental health comorbidities, and disenfranchisement of the loss (Shear et al., 2017). Unaddressed grief can result in prolonged grief disorder, impaired social and occupational function, isolation, negative health and mental health outcomes, and increased risk of suicidal ideation/suicidality and substance misuse (Supiano & Luptak, 2014).
Decades of research on adverse childhood experiences (ACEs) have provided substantive evidence that “exposures to adverse childhood experiences converge dose dependently to potently increase the risk for a wide array of causally inter-linked mental illnesses, addictions, and multi-organ diseases” (Zarse et al., 2019, p. 2). In addition to increased risk of mental illness and addiction disorders, people with four or more ACEs demonstrate higher levels of risky behaviors than those with fewer ACEs (Campbell et al., 2016).
Furthermore, evidence from a study conducted by Jackson et al. in the United Kingdom suggested that “child property delinquency, substance use, low self-control, unstructured socializing, and parent-child attachment at age 11 all significantly mediate the relationship between early ACEs and delinquency in adolescence, with early delinquency and low self-control emerging as the most robust mediators” (Jackson et al., 2023, p. 1). The impact of ACEs appears to persist into adulthood in the form of increased risk for criminality. Reavis and associates evaluated 151 people from four different “offender groups” referred for treatment following conviction in a criminal court. In comparison with a normative sample of males, the offender groups reported four times as many ACEs, leading researchers to conclude that “childhood adversity is associated with adult criminality” (Reavis et al., 2013, p. 44).
In one of the earliest investigations of the impact of traumatic grief on criminality, Leach, Burgess, and Holmwood (2008) noted that unresolved loss and grief issues in incarcerated people manifest as trauma, which is further exacerbated by incarceration. In their theoretical framework, incarceration results in poor emotional processing skills and suppression of healthy/effective mourning leading to recidivism, defined as a relapse into criminal activity after release from prison. Similarly, Maschi et al. (2011) reported significant residual trauma secondary to accumulated losses and deaths that occurred over the life course in older incarcerated people.
Other investigations have reported on the deaths of those close to the incarcerated person during their time in prison. Fahmy et al. (2024) reported that 41% of incarcerated people experienced the death of a family member or friend on the outside during their final year of incarceration—and that the magnitude of this grief could be somewhat buffered by external social support and in-prison social cohesion. Harner, Hentz, and Evangelista (2011) identified four negative outcomes of unaddressed grief that occurred in incarcerated females: a sense of being frozen in time since the loss, having no space/place to grieve, burying emotions, and feeling lonely while “never being alone.” Each of these studies called for further research into the grief of incarcerated people as well as clinical approaches to address unaddressed loss and grief.
More recently, Wilson (2023) proposed a theoretical model to address the “far-reaching effects” of multiple losses that may contribute to illegal activity (p. 1). Wilson suggests that “grief overload,” that is, the intensity of the unprocessed cumulative grief experiences, may contribute to an individual’s propensity for maladaptive coping and criminal behavior. Wilson articulates the following seven key risk indicators in the prisoners’ grief overload theory:
(1) Death is experienced as high in intensity. (2) Underlying factors negatively affect resistance and heighten susceptibility to maladaptive coping. (3) The griever’s sense of self-worth becomes diminished. (4) The grief response is disproportionate according to wider societal norms, that is, its influence exceeds the ability to adhere to the law, resulting in imprisonment and harm to society. Or, during incarceration, coping with ubiquitous grief and other stressors causes harm to the bereaved prisoner (i.e., through extreme maladaptive coping) and may negatively impact the prison community. (5) The overwhelming majority of stressors/strains are perceived by the griever as negative in nature, as distinct from the ability to recognize and confront positive grief stressors. (6) Effective oscillation between loss-oriented and restoration-oriented coping responses and taking time out for rest and recuperation—particularly in prison—become unattainable. (7) There is an absence of meaningful social support (Wilson, 2023, pp. 17–18).
This theoretical framework and the research literature suggest that unaddressed trauma that occurs at any point in the life course may precipitate and maintain problematic substance use, criminal behavior, and resultant incarceration. Furthermore, in a comprehensive, trauma-informed model of care, grief due to multiple deaths, deaths in proximity, and traumatic/violent deaths needs to be addressed in incarcerated people.
The complex intersection of life trauma, problematic substance use, criminal behavior, and grief is poorly understood. Henry (2020) noted that a history of adverse life events is linked to rules violations within correctional facilities and that mental health and substance-use disorders appear to mediate this relationship. Even if that is a known effect, it does not suggest pre-incarceration causality.
Support groups can be the ideal approach to addressing long-standing trauma and sorrow. Yalom and Leszcz (2005) have described several therapeutic advantages of group work that distinguish it from other treatment modalities. Specifically, group therapy instills hope, acknowledges universality to the psychological experience, imparts information, generates altruism, permits corrective recapitulation of the family group, provides opportunities for socialization, fosters appropriate imitative behavior, promotes interpersonal learning, creates group cohesiveness, provides safe catharsis, and attends to existential factors in the human experience.
As we have demonstrated in our earlier research with groups serving clients with a history of trauma (Supiano & Luptak, 2014), the importance of establishing safety, trust, and security, being with others having similar traumas, providing psychoeducation to reduce isolation, and having specific interventions for trauma are essential. With respect to the unique needs of grieving people, group treatment can provide emotional support in the face of loss, bring grieving people together in a comfortable setting to reduce isolation, foster relationships, and create common bonds. Groups also provide a forum for sharing experiences, listening and learning, the development of effective coping skills, and provide an opportunity for suffering people to not only gain support but also provide help and support to others.
Group work is particularly suitable in mental health and substance-use treatment within correctional settings as it also incorporates social skill building, permits practice in vulnerability and trust building in a supportive context, and is cost-effective.
In this article, we detail the prison-based implementation and evaluation of an evidence-based grief support group model. This implementation was conducted in seven groups in the two substance-use disorder treatment programs within the Utah State Correctional Facility. We report findings of a pragmatic feasibility and intervention impact evaluation of the training of mental health clinicians, research and intervention feasibility, and change in grief in 69 incarcerated client-participants in a grief group. This study was approved by the University of Utah Institutional Review Board (irb_00118341), the State of Utah Department of Health and Human Services Institutional Review Board (#0677), and the Department of Corrections Research Review Board.
Method
Project Background
Since 1997, our Caring Connections: A Hope and Comfort in Grief Model grief support program at the University of Utah has been conducting loss-specific grief support groups (loss of a spouse, a child, a family member or friend, loss to suicide) for people across the state of Utah. We provide grief support groups virtually and in person and serve approximately 300 grieving people per year.
In 2020 we received a grant from the Utah Division of Substance Use and Mental Health to develop a grief support group model for the unique experience of the grief of overdose death, modeled on our established group support intervention for the grief of suicide death. Subsequently, we developed a broader group support intervention for the grief of sudden death. Under that grant, we have trained 989 clinicians across the state. We continue to support and evaluate the implementation of this model in varied mental health agencies, substance-use disorder treatment programs, and other social service agencies using clinicians in those agencies trained in this grief support group model.
The Grief Support Group Model
The grief support group model is a manualized eight-session group support intervention conducted as a closed (vs. drop-in) group in 90-minute weekly sessions and is designed for six to 12 participants per group. These grief support groups use a topic-based, incremental curriculum to increase grief normalization and understanding, enhance effective coping skills, foster remembrance apart from the circumstances of the death, and address meaning-making (see Table 1).
Grief Group Session Themes
Setting
The Utah State Correctional Facility is a 3,600-bed facility presently housing 3,059 people. The facility opened in 2022 and is organized as seven secure units: (1) a male maximum security building; (2) a building for males who qualify for work, programming, and education; (3) a geriatric and mental health treatment unit; (4) a female general population building; (5) a female maximum-security building; (6) a building housing people convicted of sex crimes; and (7) an intake unit.
The grief support program was implemented in two prison substance-use disorder treatment programs in earnest, after COVID restrictions were lifted in 2021. ConQuest is the men’s substance-use treatment program at the Utah State Correctional Facility (building 2). It currently serves 128 clients in residential, intensive outpatient, and pretreatment. Each level of care is determined by a clinical assessment, with residential treatment being the largest and most robust treatment offered. Clients within the program live in the highest privilege level within the general population, an area where clients have access to more frequent time in the yard, the gymnasium, and extracurricular activities. To live in this housing unit, clients must meet higher standards of behavior enforced by both security and therapy staff.
The Elevate program is the women’s substance-use treatment program at the correctional facility (building 5). It serves 56 clients and has also offered grief support groups to its clients since 2021.
Clinical Education in the Grief Support Group Model
Clinical training consists of single-day events with a total of 6 hours of content, including identification of those grieving overdose/suicide/traumatic death; assessment skills including loss inventory, adverse life events, risk for suicide, and risk of substance misuse/abuse of griever/of associated family; training in the grief support group model intervention components; clinician self-care guidance; and team-building skills. Training content includes video interviews with people bereaved by traumatic death and a 2-hour video portrayal of the key treatment components of the eight sessions using actors. The training was highly interactive, with trainees discussing various clients and situations with trainers. Clinician trainees receive six continuing education credits for the course.
Clinician Trainees
In an incremental manner, we have trained all the substance-use/mental health clinicians in the state correctional system. We initially trained three clinicians in 2020 who, due to pandemic precautions, were not able to implement the groups. In this project, we report on the training of 11 mental health clinicians in the prison, three of whom conducted the seven reported groups.
Sample
Potential grief group participants were identified by clinical social workers in the ConQuest and Elevate programs as having a reported death of a family member or friend. Essentially, all clients in these units qualified by privilege status, yielding a convenience sample. We had no exclusion criteria, as our exclusion criterion in the community population, active suicidality with plan, was not present in this closely monitored client group (clients with active suicidality would be transferred to an acute mental health unit). Clients were scheduled for information/consenting/enrollment interviews with study staff based on work schedules and time available before final parole hearings. Separate groups were conducted for male and female clients.
Informed Consent Procedures
As incarcerated people represent a potentially vulnerable population, care was taken to adhere closely to the U.S. Department of Health and Human Services’ guidance for prisoner involvement in research (2003), as well as the University of Utah and State of Utah guidelines on research protection of vulnerable human subjects. Adherence to these principles was evaluated at each of the three supervising institutional review board reviews.
Because participation in therapeutic activities is a condition of parole and attendance counts toward parole, our research team was especially sensitive to avoid coercion in any form. Clients who participated in the program were already well known by the social workers who made referrals and conducted the groups, as they coordinate all mental health services for this population. Potential participants met with one of the study team members in semiprivate rooms (door partially open) for interviews that included sharing the study goals, answering any questions, obtaining witnessed signatures on consent documents, and completing intake interviews and initial grief assessments. The same study team collected all posttest data. Pretest data were obtained 1 to 2 weeks before each eight-session group, and posttest data were obtained in the week following the groups.
Measures
Trainee participant satisfaction with training assessed content relevance, satisfaction with curriculum materials, and willingness to “recommend to my agency/other clinicians.” Participant satisfaction was measured with a mean score from four items on a scale from 1 (not relevant) to 3 (very relevant). Self-efficacy of clinicians in the program was assessed on a 16-item scale adapted according to Bandura’s (1977) framework for assessing self-efficacy in clinical skills. Participant self-efficacy was measured with a mean score from 16 items on a scale from 1 (not at all) to 5 (very). There were two recommendation items with yes or no responses.
With respect to grief group participants, the primary outcome was treatment response, measured as self-reported change in scores on the Inventory of Complicated Grief-revised (ICG-r), the Brief Grief Questionnaire (BGQ), and the weekly, facilitator-generated Clinical Global Impressions (CGI) scale. The BGQ (Shear & Essock, 2002) is a 5-item Likert scale for self-reporting the presence of grief symptoms ranging from “not at all” to “a lot.” Possible scores range from 0 to 10; a total score of 5 or more is positive for complicated grief. The BGQ has a high reported reliability (Cronbach’s α = 0.75) and a high discriminant validity. The clinical cut score for problematic grief is ≥4.
The ICG-r (Prigerson et al., 1995) is a 19-item measure assessing severity of prolonged grief disorder symptoms. The ICG-r has excellent internal consistency (Cronbach’s α = 0.94) and good convergent validity with other grief symptom measures. The typical score threshold for inclusion in prolonged grief disorder research has been an ICG-r score of ≥30; however, the recommended clinical cutoff is scores ≥25, reflecting a grief with significant functional impairments.
The CGI scales (Guy, 1976) were used to determine individual participant baseline status and weekly change. The CGI scales have demonstrated high levels of validity, 0.86 to standard measures, and are strongly associated with both self-report (Cronbach’s α = 0.62) and clinician-administered measures (Cronbach’s α = 0.72) of specific symptomatology and impairment across multiple conditions.
The CGI-Severity subscale was used to establish the baseline performance of participants and was rated by facilitators on the following 5-point scale: 1 (normal, not at all ill), 2 (borderline mentally ill), 3 (mildly ill), 4 (moderately ill), and 5 (markedly ill). The CGI-Improvement subscale was used by facilitators to assess weekly change and is a single Likert-type rating from 1 to 7 where 1 through 3 indicate very much, much, and minimally improved, respectively; 4 indicates no change; and 5 through 7 indicate minimally, much, and very much worse, respectively. While all selected outcomes and measures are reliable and valid and have been widely used with a variety of populations, we have no evidence of additional validation studies in the setting of corrections, yet no reason to doubt their suitability.
All outcomes (ICG, BGQ, and CGI ratings, including the Severity and Improvement subscales) were analyzed using generalized mixed modeling using the R software package. A fixed factor of time (baseline vs. postgroup, or Week 1, Week 2, etc.) was included in the model as well as a random factor of participant. Generalized mixed modeling allows for the correlated data structure due to participants having multiple data points (longitudinal/repeated measures).
We sought to triangulate data from three sources as follows: clinician identification and referral of appropriate potential participants, use of the two self-reported measures, and use of one clinician evaluation tool. As this was a pragmatic evaluation, we also examined the research feasibility measures of participant recruitment, demand, and participant retention, as well as the intervention feasibility measurements of acceptability by clinicians, acceptability by clients, and user practicality (see Table 2).
Feasibility a and Outcome Measures
After Bowen et al., 2009.
BGQ, Brief Grief Questionnaire; CGI, Clinical Global Impressions; GSM, Grief Support Model; ICG-r, Inventory of Complicated Grief-revised.
Results
Clinician Training
Trainee-Participant Satisfaction and Self-efficacy
There were 11 registered trainees. Participant satisfaction scores were high with a mean of 2.95 (standard deviation or SD = 0.10). Participant self-efficacy was also high with a mean of 4.74 (SD = 0.22). Most trainees (9, 82%) answered yes to the item, “I would recommend this training for my agency administrative personnel in the future.” All 11 trainees answered yes (11, 100%) to the item, “I would recommend this training for my agency clinical personnel in the future.”
Feasibility Outcomes
With respect to training feasibility, all appropriate mental health clinicians in the Utah Department of Corrections were eager to receive the training, and the majority found it very relevant and helpful. Self-efficacy was very satisfactory.
Research feasibility was also positive, with reported high demand for the program by both clinicians and potential participants. Most clients in the program were appropriate for inclusion; only one potential client had no reported losses due to death in their personal history and was not enrolled. Retention was uniformly held with exceptions being when there was a time conflict with work assignments (with these participants typically shifting to a future group) or a loss of privileges (n = 2).
With respect to intervention feasibility, in brief exit posttest assessments, most participants spontaneously expressed gratitude for the opportunity to participate. Similarly, the program proved practical, as clinicians and clients incorporated it into the larger treatment program as adjunctive to existing evidence-based therapies yet addressing an identified gap in current treatment.
Clinical Change in Grief Group Participants
A total of 69 participants were analyzed. The average age in years of the participants was 40.68 (SD = 10.84). Of the 69 participants, 44 (64%) were male, and 25 (36%) were female. Most were White (41, 59%). Our intake interviews revealed that most participants had multiple deaths and most had experience with a death they described as traumatic—both by the nature of death and by the trauma sequelae in the individual participant. Due to the scope of the study and the desire to gain client trust with the study team, we limited our inquiries into the details of the deaths.
Results indicate there was a reduction in mean ICG-r sum scores from baseline to postgroup (36.53 vs. 14.10), standard error of mean or SEM = 1.44, p < .001 (see Fig. 1). Analyses showed that BGQ scores also decreased from baseline to postgroup (5.10 vs. 1.97), SEM = 0.30, p < .001 (see Fig. 2). CGI scores for participant mental illness severity showed a statistically significant drop starting at Week 3, p < .05 (see Fig. 3). CGI ratings for participant improvement showed significant improvement starting at Week 3, p < .05 (see Fig. 4).
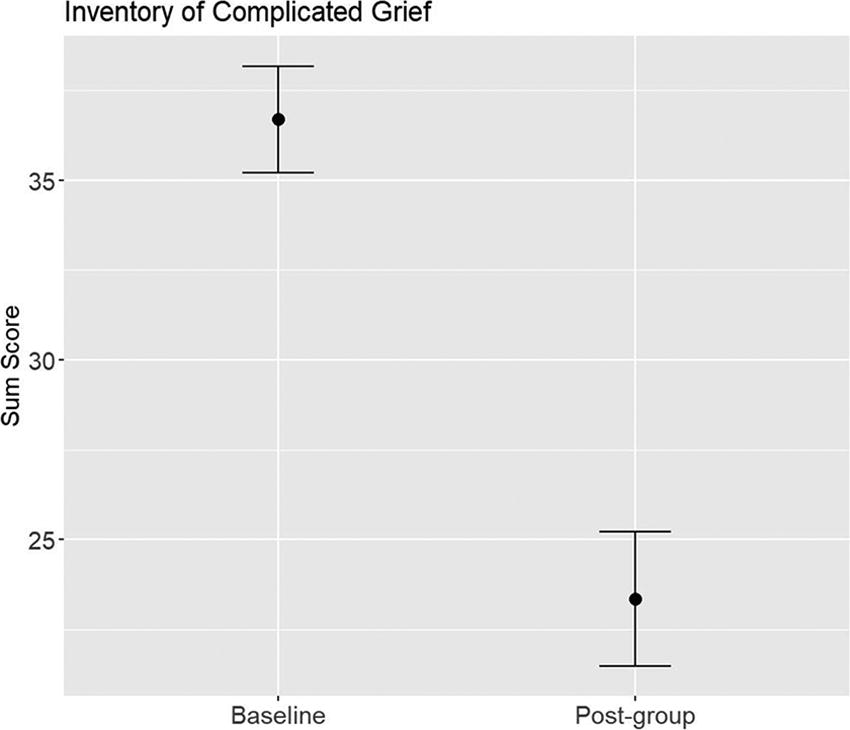
Change in self-reported grief on the Inventory of Complicated Grief-revised.
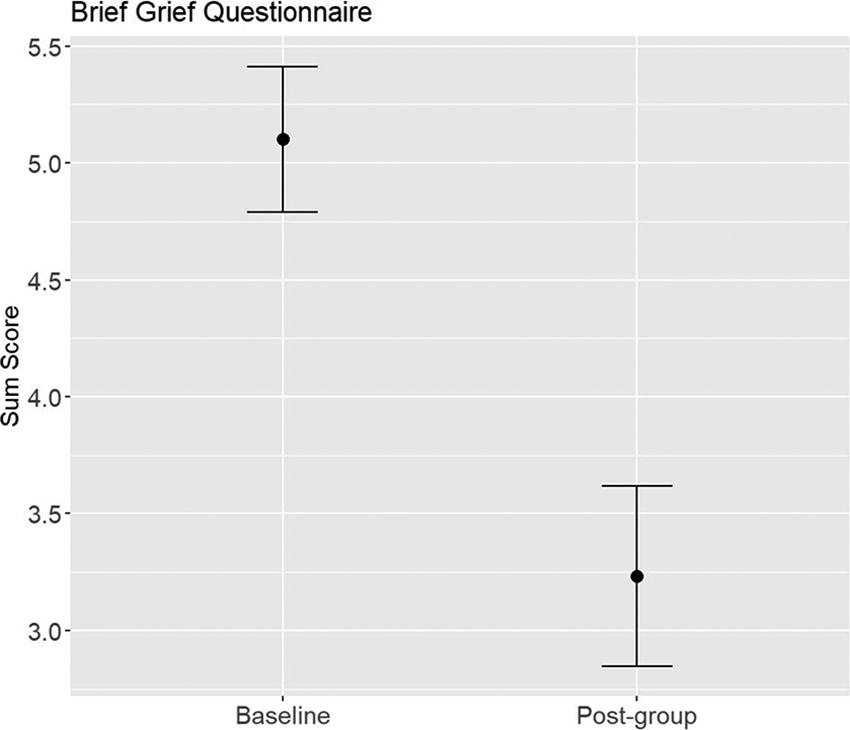
Change in self-reported grief on the Brief Grief Questionnaire.
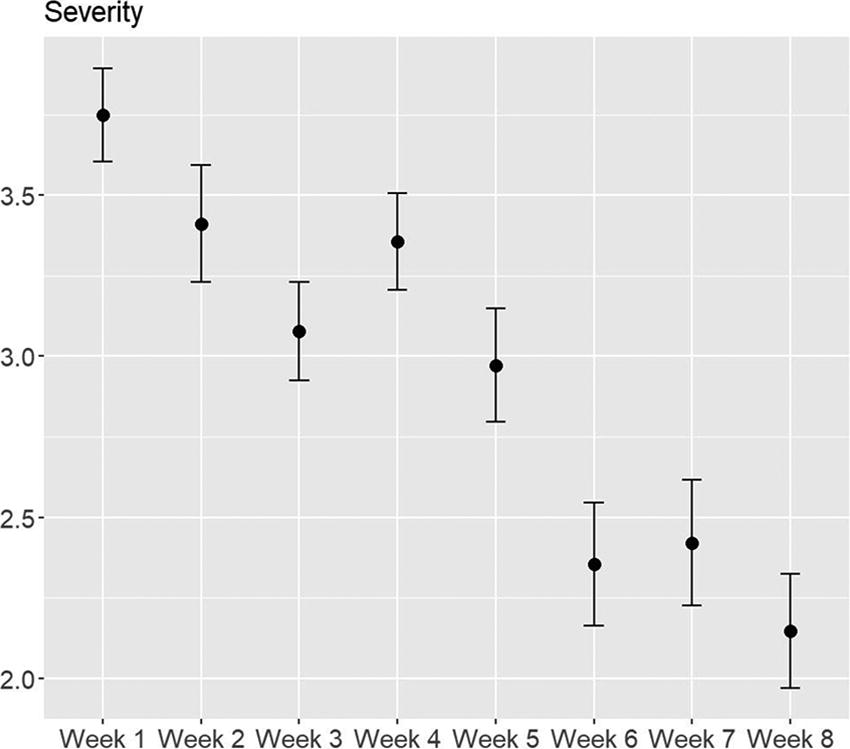
Change in clinician-reported grief on the Clinical Global Impressions-Severity subscale.
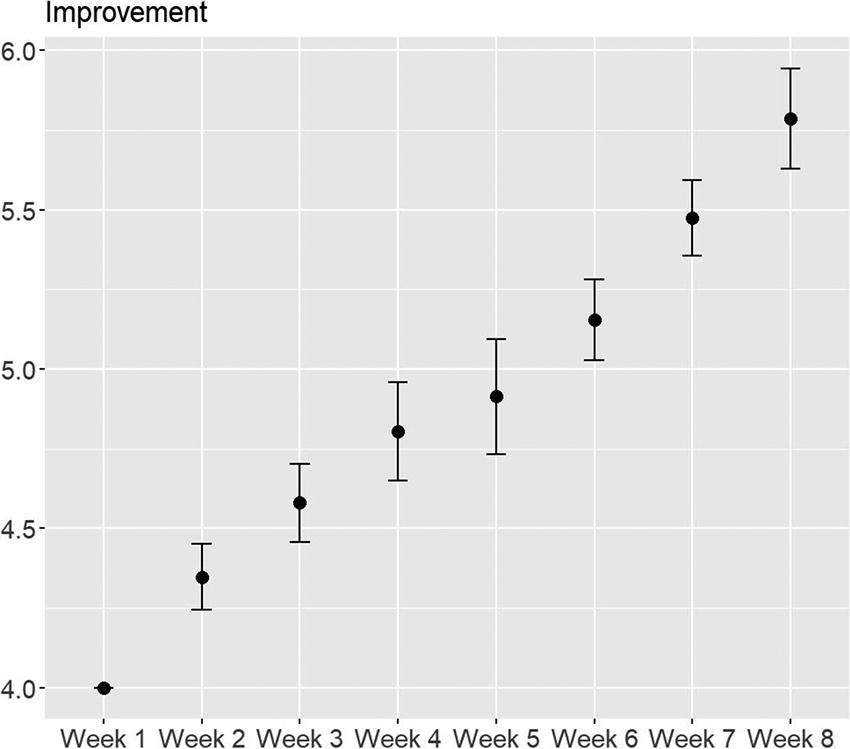
Change in clinician-reported grief on the Clinical Global Impressions-Improvement subscale.
Discussion
This pragmatic evaluation of the implementation of the grief support group model in prison substance-use treatment programs demonstrated promising outcomes for further translation and dissemination. Clinicians trained in the intervention were engaged, satisfied, and reported high levels of self-efficacy. Notably, they collectively expressed that therapeutic attention to traumatic grief addressed a gap in their existing trauma-informed approach to late-stage incarceration.
Implementation proved feasible in both the research approach and in clinical application of the intervention. With well-trained and committed clinicians reviewing caseloads, appropriate potential participants were identified, enrolled, and retained. Participants demonstrated that there is a demand for grief support in their overall mental health care.
Findings from the three instruments used in this study yielded evidence of significant positive change in grief across all measures. Scores on both of the self-reported measures, the BGQ and the ICG-r, indicated significance at p < .001. Notably, this reflects not only statistical significance but also clinical significance, in that the change in scores on each measure began with mean scores at the high-risk cutoff levels and ended with grief scores in the range of normal grief. This suggests that participants were processing their grief in constructive, productive ways. Clinician evaluations also support this conclusion, as participants demonstrated markedly decreased grief severity and significant grief improvement. This change gained momentum in Week 3 as, at that point, participants had “shared their stories” in a nonjudgmental and safe environment and could utilize the treatment content.
It is essential to state here that, even with marked improvement, the participants’ grief is not “finished,” as grieving is a lifelong process and painful grief episodes will likely recur. Participants attained a level of understanding of problematic and healthy grief and of productive processing and coping skills in a supportive setting that will contribute to future effective grieving.
Participants in this study reported multiple losses experienced across the life course and frequently of a traumatic or violent nature. The observed grief change indicates that these incarcerated people brought a magnitude of loss not typically seen in the general population, affirming the potential role that ACEs play in unaddressed grief. Yet this particular participant population, now in the final phase of incarceration, most likely brought a readiness to address long-held sorrow. The grief support groups were, therefore, ideal for this setting as one component of a comprehensive substance-use/mental health treatment and life skills therapeutic environment within the correctional system.
Strengths and Limitations
This study, while suitable for a pragmatic trial, was limited by its size. Further fully powered efficacy studies are warranted. The intervention evaluation within a specific subpopulation—substance-use treatment program clients within one prison—limits generalizability to other correctional populations. The strengths of the study include the contribution of a feasibility evaluation that targeted people with high levels of traumatic grief and evaluated the grief support group model in incarcerated people—an underrepresented mental health population.
Conclusion
This study contributes scientific evidence to the prisoner’s grief overload theory articulated by Wilson, as it is evident that the incarcerated people who participated in these seven grief support groups were experiencing grief overload. Yet, we demonstrate that this pregroup grief overload, as evidenced by grief severity, can be successfully reduced with the grief support group model. We further established that the impact of grief can be buffered by properly executed group cohesion (Fahmy et al., 2024) and existing negative grief sequelae (e.g., having no space/place to grieve, burying emotions, and feeling lonely while never being alone; Harner et al., 2011).
The key finding of the success of this pragmatic study is that this intervention was effectively implemented using existing clinicians as a complementary modality within a well-designed therapeutic program at the proper time for suitable clients. The grief support group model and its manual and training components can be readily utilized in mental health and substance-use treatment programs with the U.S. correctional system.
Footnotes
Acknowledgments
The authors appreciate the support of the Utah State Department of Health and Human Services—Substance Use and Mental Health Services leadership—VaRonica Little and Megan West. They are grateful for their colleagues in the Utah Department of Corrections and Marcie Remington, LCSW, whose vision brought this project to fruition.
Authors’ Contributions
K.P.S. was responsible for the conceptualization, funding acquisition, method design, conducting the investigation, and administration of this project, as well as the writing and editing of this manuscript. M.E.: Project conceptualization and administration, writing-original draft. A.F. and K.P.G.: Data collection, management and curation, writing-original draft. L.B.: Data collection, management and curation, writing-original draft, review and editing. A.B.: Funding management, writing-original draft. B.W.: Software, Data Curation, Data analysis, writing-original draft.
Author Disclosure Statement
The authors have no potential or actual conflicts of interest to declare.
Funding Information
This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding, in part, from the National Center for Research Resources and the National Center for Advancing Translational Sciences, the National Institutes of Health, through grant UM1TR004409 (formerly UL1TR002538).