
Abstract
Purpose:
Childhood cancer survivors have increased risk of cardiac late effects that can be potentially mitigated by physical activity and fitness. We aimed to (1) compare cardiovascular disease (CVD) risk between survivors and controls, and (2) examine whether the associations of moderate-to-vigorous physical activity (MVPA), cardiorespiratory fitness (CRF), and musculoskeletal fitness (MSF) with CVD risk factors differed between survivors and controls.
Methods:
Within the Physical Activity in Childhood Cancer Survivors (PACCS) study, we assessed CVD risk factors (android fat mass, systolic blood pressure [SBP], total cholesterol/high-density lipoprotein [HDL]-cholesterol, and glycosylated hemoglobin) in 157 childhood cancer survivors and 113 age- and sex-matched controls aged 9–18 years. We used multivariable mixed linear regression models to compare CVD risk factors between survivors and controls, and assess associations of MVPA, CRF, and MSF with CVD risk factors.
Results:
Compared with controls, survivors had more android fat mass (861 vs. 648 g, p = 0.001) and lower SBP (114 vs. 118 mmHg, p = 0.002). MVPA, CRF, and MSF were associated with lower levels of android fat mass and total cholesterol/HDL-cholesterol, and higher SBP in survivors. Associations of MVPA, CRF, and MSF with CVD risk factors were similar in survivors and controls (Pinteraction > 0.05), except the associations of CRF and MSF with android fat mass, which were stronger in survivors than in controls (Pinteraction ≤ 0.001).
Conclusion:
Owing to higher levels of android fat mass and its stronger association with physical fitness in childhood cancer survivors compared with controls, survivors should get targeted interventions to increase fitness to reduce future risk of CVD.
Introduction
At present, there are an estimated half a million childhood cancer survivors (further referred to as survivors) in Europe, and the population is growing. 1 Despite good survival prognosis, survivors are at risk of treatment-related late effects, including cardiac conditions, abnormal pulmonary function, musculoskeletal deficits, and fatigue2,3; all conditions that can lower physical activity and fitness.
Cardiovascular disease (CVD) is highlighted as one of the most serious late effects among survivors, associated with premature mortality. 4 The literature on adult survivors of childhood cancer reports a sevenfold increased risk of dying from CVD compared with the general population. 5 Moreover, unfavorable levels of CVD risk factors are found in adult survivors compared with references.6–10 Whether increased CVD risk is present already in adolescent survivors is not well studied.
In adolescents with no history of cancer, high levels of moderate-to-vigorous physical activity (MVPA) and fitness are associated with reduced CVD risk factors, such as less adiposity, lower risk of hypertension and hyperlipidemia, and improved glycemic control.11–15 In adolescents who have survived cancer, the literature shows that they have lower levels of physical activity and fitness compared with controls,16–18 persisting many years after treatment completion, which potentially exacerbates their risk of late effects. The literature on the associations of physical activity and fitness with CVD risk factors in these adolescent survivors is scarce. One sole study, looking at physical activity and CVD risk factors in adolescent survivors and controls, showed less adiposity with high levels of physical activity in both groups; however, the association was stronger in survivors compared with controls. 19 The authors found no association between physical activity and measures of blood pressure, lipids, or glucose/insulin. We are not aware of any study looking at physical fitness and CVD risk factors in adolescent survivors.
Cardiorespiratory fitness (CRF) and musculoskeletal fitness (MSF) are physiological characteristics dependent on both modifiable factors (i.e., MVPA) and nonmodifiable factors (i.e., genetic factors).20,21 Because of cancer treatment, survivors may reap the rewards from physical activity differently compared with the general population. 22 Exposures to anthracyclines and radiation to the heart can lead to abnormal hypertrophic response to exercise and interfere with cardiac and vascular adaptive mechanisms. 22 In line with this, our previous publication showed that the positive associations between moderate and vigorous physical activity with CRF were moderated when adjusting for cancer-related variables. 23 Knowing whether adolescent survivors of childhood cancer already have unfavorable CVD risk factors and how they relate to physical activity and fitness, can help to develop targeted interventions at the right time point. In this study, we have a unique opportunity to examine CVD risk factors in association to MVPA, CRF, and MSF.
The aims of this study were thus to:
compare CVD risk factors in adolescent survivors with age- and sex-matched controls, and examine whether the associations of device-measured MVPA, directly measured CRF, and isometric MSF with CVD risk factors differ between survivors and controls.
Methods
Study design and participants
This study is part of the international, multicenter study Physical Activity in Childhood Cancer Survivors (PACCS). Recruitment procedures and methodology are described in detail elsewhere. 24 We describe the methods relevant for this cross-sectional substudy hereunder.
We recruited survivors at their pediatric outpatient clinics when visiting for scheduled follow-up care, from three study sites (Oslo, Norway; Bergen, Norway; and Basel, Switzerland). Age- and sex-matched controls were recruited via the participating survivor (friend or sibling, Norway), or through the hospital staff (Basel). Because not all survivors had a sibling or were comfortable asking a friend to participate in the study, the sample includes fewer controls than survivors from Norway.
Inclusion criteria were age between 9 and 18 years, ability to perform a cardiopulmonary exercise test; and for survivors, any previous cancer disease, cancer treatment completed ≥1 year before recruitment, and participation in the previous part of the PACCS study. Participants were excluded if they had language or cognitive difficulties, or cardiopulmonary exercise testing was considered not possible because of physical or cognitive impairments. Participant recruitment and data collection were performed between January 2019 and January 2021. The last participants were recruited during the coronavirus disease 2019 (COVID-19) pandemic and some study visits were postponed based on the national regulations and recommendations.
Measures
Outcomes: CVD risk factors
We measured body composition by dual-energy X-ray absorptiometry and estimated android fat mass (g). Android fat mass is shown to be more closely correlated with the unhealthy visceral adipose tissue than more traditional measures, such as body mass index and waist circumference. 25 Participants came nonfasted and in light clothing. We scanned participants from head to toe in a supine position by Lunar iDXA (GE Healthcare) using the enCORE Software Version 14 and 18 (Norway), or by Horizon A (Hologic, Inc.) using the InnerCORE Software Version 13 (Basel).
After at least a 30-minute lunch break, participants entered the fitness testing lab for preparation, including resting blood pressure measurements. We attached electrocardiogram electrodes and wires before situating an appropriate-sized blood pressure cuff on the participant's right arm. Participants were seated in a back-supported chair with feet flat on the floor and their arms relaxed in their lap for a 5-minute rest before the blood pressure measurements. 26 No talking was allowed during or between measurements. At least two measurements were performed using an automated oscillographic blood pressure device (Suntech Tango+) in Oslo and in Basel (Suntech Medical Instruments); and Suntech Tango M2 in Bergen (Suntech Medical Instruments), and the lowest value of systolic blood pressure (SBP; mmHg) was used in the current analysis.
We collected nonfasted blood by venous sample in Norway, and by venous or capillary sample in Basel. Blood samples were collected from survivors from all three study sites, and from controls in Oslo (n = 52) and in Bergen (n = 6). We measured lipid metabolism as the ratio between total cholesterol and high-density lipoprotein (Total/HDL-cholesterol), and glucose metabolism as glycosylated hemoglobin (HbA1c; mmol/mol), which are unaffected by fasted state.27,28 Analyses were performed at medical laboratories by photometric methods and high-performance liquid chromatography to analyze cholesterol measures and HbA1c, respectively.
Exposures: physical activity, CRF, and MSF
Detailed information on equipment and procedures are provided in the Supplementary File S1.
We equipped participants with a hip-worn accelerometer (ActiGraph GT3X-BT) to assess MVPA (minutes/day) defined as ≥2000 counts per minute, 11 sampled in 10-second epochs. Participants were instructed to wear the monitor for eight consecutive days and to remove the monitor only for sleep and water-based activities. The accelerometers were initialized at a sampling rate of 30 Hertz, and accelerometer files were processed using the KineSoft analytical software version 3.3.80, restricted to hours between 06:00 and 23:59. Nonwear time was defined as periods of ≥20 consecutive minutes of zero counts. Minimum 8 hours/day of wear was defined as a valid day, and more than or equal to three valid days were required to be included in the analyses (Figure A in Supplementary File S1).
Participants performed cardiopulmonary exercise testing to assess CRF. In Norway, the test was performed by walking and running on a stationary treadmill, whereas in Basel, the test was performed on an electronically braked ergometer cycle (Supplementary File S1). Gas exchange was determined by breath-by-breath sampling, averaged over 30-second intervals, through a breathing mask. Participants performed a continuous incremental task to volitional fatigue, and VO2-peak was defined as the highest oxygen uptake during the test and was standardized for kilogram of fat-free mass (mL∙fat-free mass−1∙min−1). We estimated fat-free mass by subtracting fat mass from body weight derived from dual-energy X-ray absorptiometry.
After a 7- to 10-minute warm-up on a treadmill/ergometer cycle, we estimated MSF by maximal isometric knee extension (kg) and chest press (kg) where force curves were registered (Supplementary File S1). The participants performed a minimum of three attempts with 5-second maximal effort, with 60-second breaks, in each isometric exercise until maximum force was achieved. The criterion for a valid attempt was flattening of the force curve at the highest force achieved, without systematic fluctuations. The highest value for each exercise was registered, summarized, and standardized to body weight as a proxy of whole-body MSF.
Covariates: age, sex, puberty stage, and cancer-related characteristics
We determined puberty stage by the self-reported Pubertal Development Stages questionnaire. 29 Participants were categorized as prepubertal if they reported the lowest category for all indices, postpubertal if they reported the highest category for all indices, whereas the remaining participants were categorized as pubertal.
We extracted cancer diagnosis and a limited number of available key factors concerning cancer treatment from the survivors' medical records: age at diagnosis, cumulative anthracycline dose (doxorubicin isotoxic equivalent dose, mg/m2), 30 cumulative radiation dose (gray [Gy]), radiation site (central nervous system [CNS], thoracic, abdominal, total body, other), high-dose steroids as part of cancer treatment protocol [prednisolone equivalent dose of 60 mg/(m2·day) or more; yes/no], and relapse (yes/no).
Statistical analyses
Characteristics are expressed as frequencies (percentages) or means ± standard deviations for survivors and controls.
To compare CVD risk factors between survivors and controls (aim 1) we calculated marginal means with 95% confidence intervals (CIs) and p-values from mixed effects linear regression models, with study site and survivor–control pair as random intercepts to account for clusters in the data, in addition to the fixed factors age, sex, and puberty stage.
To assess whether the associations of MVPA/CRF/MSF with CVD risk factors differ between survivors and controls (aim 2), we performed mixed-effects linear regression models including an interaction term between the exposure (MVPA/CRF/MSF) and participant status (survivor/control). In model 1, we adjusted only for study site and survivor–control pair as random intercepts. In model 2, we additionally adjusted for age, sex, and puberty stage as fixed effects (Figure B in Supplementary File S1). We defined missing information on puberty stage as own category to avoid losing participants in the analyses. We compared the fully adjusted models including either a two-way or three-way interaction term using likelihood ratio tests. Models with a two-way interaction term yielded in general the best model fit and were thus selected for analyses.
We used the delta method (by STATA's margins command) to extract marginal means and 95% CIs for survivors and controls from the mixed model. All p-values were two-sided, and we considered p ≤ 0.05 as statistically significant. Analyses and graphics were conducted using Stata statistical software (version 17.0; Stata Corp.).
Results
Study population
Of the 267 eligible invited survivors, 157 (59%) agreed to participate (Fig. 1), together with 113 controls (unknown participation rate owing to the recruitment procedure).
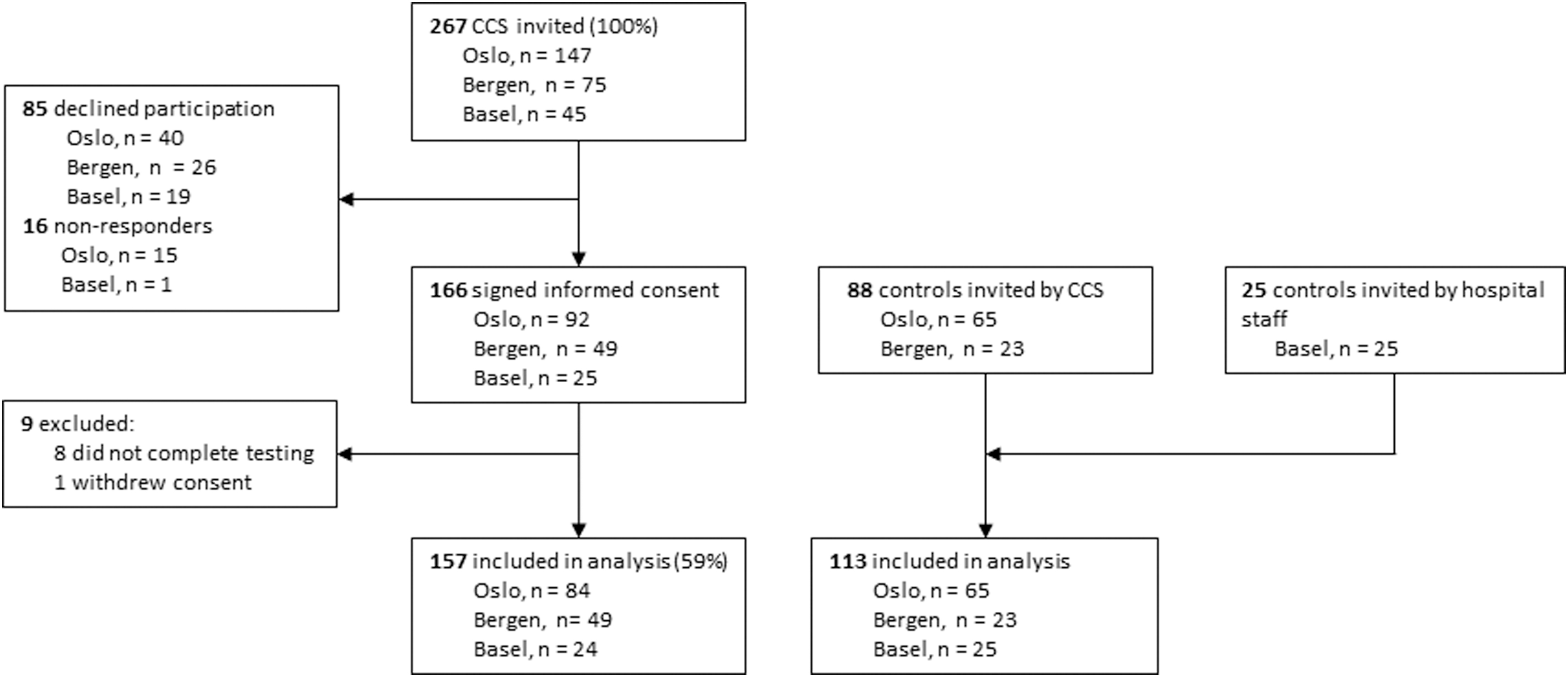
Flowchart of the inclusion process. CCS, childhood cancer survivors (referred to as survivors).
Demographics were similar between survivors and controls (Table 1) but survivors had higher body mass, body mass index, and fat mass than controls. On average, survivors were ∼5 years old at diagnosis and ∼8 years from diagnosis. Half were diagnosed with leukemia; 78% had received anthracyclines; 29% radiotherapy; and 57% high-dose steroids as part of their cancer treatment protocol.
Characteristics of Childhood Cancer Survivors and Controls
Numbers are means with standard deviations if not stated otherwise.
Missing value on puberty stage in five controls.
Missing value on fat mass and fat-free mass in three survivors and one control.
Includes neuroblastoma (n = 9), eye cancer (n = 2), kidney cancer (n = 14), liver cancer (n = 2), bone tumor (n = 6), soft-tissue sarcoma (n = 10), others (n = 2).
Missing info on anthracyclines in two survivors and anthracycline dose in nine survivors.
Missing radiotherapy dose in one survivor.
Multiple radiation locations possible.
As part of cancer treatment protocol [prednisolone equivalent dose of 60 mg/(m2·day) or more].
CNS, central nervous system; Gy, gray; ICCC-3, International Classification of Childhood Cancer—Third Edition; NA, not applicable.
CVD risk factors
Compared with controls, survivors had more android fat mass (Table 2; marginal mean 861 vs. 648 g, p = 0.001) and lower SBP (marginal mean 114 vs. 118 mmHg, p = 0.002). Total/HDL and HbA1c were similar between survivors and controls. Our post hoc explanatory analysis showed that CNS-irradiated survivors had more android fat mass compared with non-CNS–irradiated survivors (1009 ± 537 g vs. 853 ± 718 g).
Marginal Means of Cardiovascular Disease Risk Factors with 95% Confidence Intervals in Survivors Versus Controls
Blood samples were drawn from controls mainly from Oslo, hence the large number of missing Total/HDL and HbA1c values in this group.
Marginal means with 95% CIs and p-values from mixed-effects linear model with study site and survivor–control pair as random intercepts and age, sex, and puberty stage as fixed effects.
Missing value for android fat mass in three survivors and one control.
Missing value for SBP in seven survivors and four controls.
Missing value for Total/HDL in 7 survivors and 55 controls.
Missing values for HbA1c in 7 survivors and 56 controls.
CI, confidence interval; CVD, cardiovascular disease; HbA1c, glycosylated hemoglobin; SBP, systolic blood pressure; Total/HDL, total cholesterol/high-density lipoprotein.
Associations of physical activity, CRF, and MSF with CVD risk factors
Figure 2 provides the associations of MVPA, CRF, and MSF with CVD risk factors in survivors and controls, respectively, with p-value for the interaction between participant status (survivor/control) and the respective exposure. The results in Figure 2 are based on increases of 10 minutes of MVPA, 5 mL∙fat-free mass−1∙min−1 of VO2-peak (CRF), and 0.25 total kg pushed∙kg bodyweight−1 of MSF (Tables A–C in Supplementary File S2). Background information on accelerometer data quality and distribution of the exposure variables MVPA, CRF, and MSF in survivors and controls is provided in Supplementary Table D in Supplementary File S2.

Associations of MVPA, CRF, and MSF with
Android fat mass
There was no significant interaction between survivors and controls on the association between MVPA and android fat mass (Pinteraction = 0.15; Fig. 2A). However, higher levels of MVPA among survivors were associated with significantly less android fat mass, compared with no significant association in controls (−52 g [95% CI: −85 to −19] vs. −15 g [95% CI: −57 to 27]). The association between CRF and android fat mass was significantly different between survivors and controls (Pinteraction = 0.001), with a significant association in survivors, but not in controls (−145 g [95% CI: −193 to −97] vs. −28 g [95% CI: −87 to 31]). MSF was associated with significantly less android fat mass in both survivors and controls (−302 g [95% CI: −361 to −243] and −143 g [95% CI: −212 to −74], respectively); however, the association was stronger in survivors than in controls (Pinteraction < 0.001).
Systolic blood pressure
Associations of MVPA, CRF, and MSF with SBP were similar for survivors and controls (all Pinteractions > 0.05). CRF was positively associated with SBP in both survivors and controls, whereas MVPA and MSF were positively associated with SBP in survivors only. In survivors, higher MVPA, CRF, and MSF were associated with 0.7 (95% CI: 0.0 to 1.4), 1.6 (95% CI: 0.6 to 2.6), and 1.6 mmHg (95% CI: 0.2 to 2.9) higher SBP, respectively.
Blood values
There was no significant interaction between survivors and controls concerning the associations of MVPA/CRF/MSF with Total/HDL (all Pinteractions > 0.05). However, the associations reached statistical significance in survivors, whereas not in controls. In survivors, higher levels of MVPA, CRF, and MSF were associated with −0.1 (95% CI: −0.1 to −0.0), −0.1 (95% CI: −0.2 to −0.1), and −0.2 (95% CI: −0.3 to −0.1) lower Total/HDL, respectively. There were no associations of MVPA, CRF, or MSF with HbA1c in neither survivors nor controls.
Discussion
We found that adolescent survivors had substantially more android fat mass, and lower SBP, compared with controls, whereas levels of Total/HDL and HbA1c were similar. Furthermore, the associations of MVPA, CRF, and MSF with CVD risk factors were similar in survivors and controls, except for a stronger association of CRF and MSF with android fat mass in survivors compared with controls.
In line with previous studies,9,10,19,31,32 we found that survivors had higher levels of adiposity (+33%) compared with healthy peers, which may be considered a clinically meaningful difference. 33 A longitudinal study by Lätt et al. showed that higher android fat mass at age 12 was associated with higher insulin and insulin resistance, and worse lipid values, in both normal weight and overweight boys 2 years later, suggesting that android fat mass has an impact on future CVD risk. 34 Results from our post hoc explanatory analysis suggest that CNS irradiation may partly explain differences in android fat mass between survivors and controls. This is in line with the current literature, where cranial radiotherapy has been reported as a central risk factor of treatment-induced obesity in survivors. 35
Survivors had lower SBP than controls (−4 mmHg). A recent study by Chow et al. found a similar lower level of SBP in a large sample of adult survivors of childhood cancer (−4 mmHg, n = 571) compared with references. 7 However, our result contrasts with most previous studies where blood pressure levels were similar31,32,36 or higher8–10 in adolescent and young adult survivors versus controls. During puberty, blood pressure increases more rapidly compared with pre- and postpubertal phases. 37 If cancer treatment has affected progression of puberty (i.e., slower pubertal development), 38 this might partly explain the lower SBP in our sample of adolescent survivors to controls. Our adjustment for puberty stage in the analyses might not have been sensitive enough to fully account for this. Future studies should consider matching controls on puberty stage rather than age per se, and preferably assess puberty stage by a more sensitive and objective measurement method.
To our knowledge, no previous study has compared Total/HDL in survivors and controls. However, two previous studies assessing HDL-cholesterol found similar levels in young adult survivors and controls,10,31 whereas three studies found lower levels in adolescent and young adult survivors compared with controls.9,32,36 No study has compared HbA1c in adolescent survivors and controls previously. However, Chow et al. reported higher HbA1c in a large sample of adult survivors of childhood cancer compared with references. 7 Levels of glucose, and hence HbA1c, are well-regulated in adolescents, as the pancreas can maintain its ability to secrete elevated amounts of insulin for years or decades before hyperglycemia manifests. 39 Accordingly, in our sample, only one survivor and two controls had HbA1c values above the prediabetic threshold (HbA1c ≥42 mmol/mol) and one survivor was above the diabetic threshold (HbA1c ≥48 mmol/mol). 40
Results from our interaction analyses imply that survivors profit more from interventions increasing CRF and MFS to reduce android fat mass as compared with the general population. We also found stronger associations between MVPA and android fat mass in survivors compared with controls, however, without statistically significant interaction. Although we did not find any interactions between survivors and controls concerning blood values, we did find lower levels of Total/HDL in survivors who had higher levels of both MVPA, CRF, and MSF. Our findings are in accordance with two articles from Slater et al. who found a stronger association between high/low PA, high/low endurance, and CVD risk factors in adolescent 19 and adult 31 survivors compared with sibling controls. More android fat mass among survivors might explain why the associations between MVPA/CRF/MSF and CVD risk factors were generally stronger in survivors than in controls.
In contrast, Slater et al. found that better endurance was associated with lower SBP in young adult survivors, and higher SBP in controls. 31 We found that higher CRF was associated with higher SBP in both survivors and controls, which might be explained by the natural increase in both CRF and SBP during puberty.37,41 Surprisingly, we did not observe associations between MVPA/CRF/MSF and measures of cholesterol and glucose in controls, which contrasts with previous studies.11–15 This might be owing to an underpowered control sample, especially for analyses on blood values.
The strengths of this study were the inclusion of adolescent survivors with a history of various cancer diagnoses from different study sites, and the use of objective measurement methods. The results are discussed under the assumption that the exposures are associated with the outcomes. However, a directional association cannot be inferred in this cross-sectional study. Thus, it is unclear whether higher MVPA/CRF/MSF is associated with, for example, a lower level of adiposity, or whether a higher level of adiposity is associated with lower MVPA/CRF/MSF. Another limitation was differences in equipment and measurement methods between study sites. Cardiopulmonary exercise testing performed on cycle ergometer compared with treadmill has been shown to underestimate CRF in the general population. 42 However, survivors were tested in the same manner as their matched control, and we accounted for differences in equipment and measurement methods between study sites by including study site as random intercept in all the models.
Similarly, we adjusted for survivor–control pair as a random intercept to account for similarities between survivors and controls that were friends/family. The relatively low participation rate (59%) might result in a selected sample toward participants with interest in physical activity and fitness, impacting the generalizability of our results. Our comparison of participants and nonparticipants in a previous publication from the current project found no significant differences in key characteristics (sex, age, age at diagnosis, time since diagnosis, diagnosis, relapse). 23 However, this is mainly relevant for aim 1 and not the investigations concerning factors associated with CVD risk since the participants still covered a broad range in the outcome and exposure variables.
Conclusions
Our results showed that adolescent survivors had more android fat mass compared with their peers. Clinicians should have the demonstrated higher level of android fat mass in mind when addressing follow-up care for survivors. Furthermore, our findings indicate that survivors may benefit more from increasing their cardiorespiratory and MSF compared with peers, possibly owing to a greater potential for reducing android fat mass. Hence, survivors should be encouraged to increase their physical activity and fitness to potentially reduce their android fat mass and thereby reduce future CVD risk.
Yet, further research using longitudinal designs is needed to assess the direct effect of increasing physical activity and fitness on android fat mass and other CVD risk factors in survivors.
Owing to higher levels of android fat mass already seen in adolescent survivors of childhood cancer and its stronger association with physical fitness compared with controls, this population should get targeted interventions to increase fitness to reduce future risk of CVD.
Footnotes
Acknowledgments
The authors thank the children and their parents/guardians for their time and effort. It is through their generosity that the authors were able to complete the study. The authors thank all members of the PACCS study group not listed as co-authors of this article.
Authors' Contributions
M.B.: Formal analysis, investigation, methodology, visualization, writing—original draft, writing—review and editing. C.S.R.: Methodology, supervision, validation, visualization, writing—review and editing. T.R.: Conceptualization, funding acquisition, project administration, writing—review and editing. M.G.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, writing—review and editing. I.K.T.: Investigation, writing—review and editing. C.S.: Investigation, writing—review and editing. E.R.: Conceptualization, funding acquisition, project administration, supervision, writing—review and editing. S.A.A.: Conceptualization, funding acquisition, methodology, project administration, supervision, visualization, writing—review and editing. All authors have approved the final version of the article, and all have agreed to be accountable for all aspects of the work.
Ethical Approval and Consent to Participate
The PACCS study was approved by the Norwegian Regional Committee for Medical Ethics (reference number 2018/739), the Data protection Officer at Oslo University Hospital, and the Ethics Committee of North-Western and Central Switzerland (project ID 2019-00410). Written informed consent was collected from all participants/parents.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The work in question is funded by the Norwegian Cancer Society (202062), and the Norwegian Research Council (20/00394). C.S. was supported by the Swiss Cancer League, the Swiss Cancer Research Foundation (KLS/KFS-4825-01-2019), and the University of Basel, Switzerland. The funding sources did not have any role in the study design, data collection, analysis, interpretation, writing of the report, or in the decision to submit the article for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.