
Abstract
Purpose:
Participatory design (PD) is a collective creative design process involving designers and nondesigners. There is limited reporting on the experience of using PD for adolescent and young adult (AYA) care. This study summarizes lessons from employing PD to develop care for AYAs with cancer.
Methods:
A qualitative multiple-case study method was conducted of three PD processes addressing food (FfC), intimacy and sexuality (I&S), and integrative medicine (IM) in caring for AYAs with cancer.
Results:
Local key stakeholders, who were exposed to a problem and had not been successful at solving it individually, were recruited to “dream” together. Through this synergy, a shared understanding of the problem and a joint mission emerged to find a solution. PD tools were used to develop a problem definition. An open mind and explorative research helped to understand the problems, and stakeholders were managed such that idea-sharing and learning were enabled. Designers translated ideas into prototypes. The PD process was prolonged due to the hierarchical hospital environment, business considerations, and additionally required evidence. The FfC program produced an effective new food service for the whole hospital. The I&S initiative developed a podcast, two articles, and a prototype website. The IM project developed a pilot study.
Conclusions:
For a PD process to successfully develop care for AYAs, one needs to use designers and skilled people, PD tools, and an open-ended approach to visualize and materialize new forms of care. Furthermore, recruitment and facilitation techniques help leverage knowledge and create a synergy in a democratic environment between stakeholders.
Introduction
Each year, about 2700 adolescents and young adults (AYAs) aged 18-35 are diagnosed with cancer in the Netherlands. 1 Since the Dutch AYA Care Network (AYA Care Network) was established in 2014, specific care for AYAs has been implemented in eight university hospitals and basic AYA care in a growing number of general hospitals across the Netherlands. However, there is still room for improvement in AYA care with many unmet needs during treatment, into adulthood, and beyond.1–5
The AYA Care Network has always set out to harness collaboration between health care professionals, AYAs, and their relatives.1,6 The AYA Care Network focuses strongly on AYA engagement with the vision “Nothing about AYAs without AYAs.” Collaborative design methods, involving AYAs themselves, have been suggested to tackle the complex challenges in cancer care.7,8 Participatory design (PD) is a collective creative design process involving three phases whereby designers and nondesigners are considered partners in the design process. 9 The three phases are exploration, creation, and testing.10–12 The aim of the exploration phase is to clarify and define the problem by combining the perspectives of all the stakeholders. The creation phase is expected to develop prototypes of potential solutions. The evaluation phase should test these prototypes which, if successful, can be implemented in practice.
Designers, particularly, help to understand and integrate the perspective of different stakeholders, for example, AYAs, into physical solutions, called prototypes of a certain product or a service. These prototypes are initially simple and then further iterated. This iterative process involves creative tools.
In PD, one of the guiding principles is that every relevant stakeholder can and should be involved in the design process.9,13 Examples of PD “make” tools, which can be utilized by designers, and also nondesigners are mind-maps, storyboards, and prototypes. 14 Such “make” tools help stakeholders express deeper lying knowledge such as complex emotions, dreams, or needs, which are hard to describe in words. 15 These insights are crucial to develop a successful service or product.
The use of PD to improve cancer care is seen as especially advantageous for AYAs for several reasons. First, AYAs receive treatments that have a life-changing impact as they go through important life events 16 and PD enables exploration of deeper levels of knowledge through these evolving phases. Second, the problems associated with caring for AYAs need to be explored with stakeholders beyond the medical paradigm, which is an inherent strength of PD. For example, not only physicians and specialized AYA nurses but also fertility and sex specialists, social workers, psychologists, and many more are involved. 16 The AYA population is also very active and open to innovation and collaboration 1 to harness their own experience for the common good, and this open mind-set can foster a successful PD project. 12 However, the implementation of AYA care services can be challenging for various reasons, including financial hurdles.16,17 Actively involving stakeholders through all the PD design phases can facilitate implementation. 9
To date, researchers have described two other PD projects where AYAs were involved. They reported that there was good engagement with AYAs in designing a care pathway, 18 and an app was positively evaluated.19,20 However, these studies did not provide in depth lessons about the use of PD as their main focus was on the developed products and services rather than evaluating the PD method.
The aim of this study is to summarize the lessons for employing PD when developing care services for AYAs. These insights may help health care professionals overcome the key challenges when employing PD to develop AYA care.
Scientific Background to Case Studies
Three case studies regarding food intake (Food for Care, FfC), intimacy and sexuality (I&S), and integrative medicine (IM) were identified by AYAs during an initial meeting organized by the AYA Care Network. 21
Food for care
The food intake of all oncology patients, including AYAs, tends to change substantially due to changes in taste, appetite, and experiencing pain when consuming food as a consequence of chemotherapy and radiotherapy. 22 Even though 40%–80% of all individuals, including AYAs, with cancer suffer from malnutrition and poorer treatment outcomes, this issue is often overlooked. 22
Sexuality & intimacy
One-third of AYAs experience sexual dissatisfaction and one-third of these desire supportive care in this area. 23 Cancer can interfere with normal sexual development.24–29 A combination of physical24,30 and psychological issues (body image) result in AYAs feeling less arousal, pleasure, and satisfaction 25 at the beginning of their sexual development phase.
Integrative medicine
AYAs not only find the use of complementary therapies such as massage, 31 music, 32 acupuncture, 33 and mindfulness 34 meaningful but also challenging. Patients are often unsupervised by physicians when using complementary therapies. 35 IM aims to combine mainstream medical and complementary therapies. 35 To avoid pitfalls of “alternative medicine,” legal and ethical issues are addressed, for example, to cope with unsupervised administration of treatments, both patients and health care professionals need to be educated about drug interactions, product contaminants, other alternative therapies and evidence on effectiveness and safety using IM interventions. 35
Method
A qualitative multiple-case study method 36 was employed following the COREQ guidelines. 37
Methodological framework
A multiple-case study approach was used to explore how PD is used in real-world applications to develop AYA care. 36 Three case studies (FfC, I&S, and IM) were selected, in which PD meetings were held and PD tools used to develop AYA care. The PD projects were called “dream teams” by the stakeholders, emphasizing the collective creative aspect of developing better AYA care while daring to imagine completely new forms of care.
Study design
Data were collected and triangulated using documents, interviews with key stakeholders, and one observation. The data collection was conducted by the lead author (PV), who had experienced leukemia at a young age himself and was trained in qualitative research before this study. Face-to-face interviews of typically one hour duration were conducted (and audio recorded) at the workplace or by a video call (audio and video recording). The interview questions (see template in Appendix A1) were piloted and adapted if necessary. Introductions were made at the start of the interviews apart from with the director of the AYA Care Network who was already well acquainted with PV. At the end of each interview, a summary of the interview was discussed for comments or corrections.
The key stakeholders (age range 23–58) interviewed were all intensively involved in one of the three case studies: four FfC, five I&S, and three IM (Table 1). Other stakeholders, who were not involved throughout the entire process, were not interviewed. They were in the FfC case: four AYA and three partners, a clinical manager, a chef, a catering company, and the hospital board of directors; in the I&S case: the Director of the AYA Care Network, six AYAs, a sexologist, a journalist, and several MSc student designers; in the IM case: the Director of the AYA Care Network, four AYAs, a specialist AYA care nurse, a massage therapist, and other complementary care specialists. The AYAs were not reimbursed and received information before the PD process started by the Director of the AYA Care Network about how to leverage their story for the greater good of this project.
Characteristics of Key Stakeholders Interviewed Per Case Study
AYA, adolescent and young adult.
Even though the contribution of all stakeholders had equal weight, there were one or more facilitators in each PD project. FfC was directly facilitated by the Director of the AYA Care Network; in I&S, there was cofacilitation with the Director of the AYA Care Network and a sexologist-urologist; and in IM, there was cofacilitation with the Director of the AYA Care Network, an oncologist and a pediatrician. The administration of the PD activities was supported by a secretarial assistant of the Director of the AYA Care Network.
Most of the documents studied (FfC: 100, I&S: 25) were collected through the director of the AYA Care network. No documents were available for IM. In each interview, stakeholders were asked if they could supply additional documents if they had any. The documents consisted of meeting notes, photographs or drawings of prototype ideas, presentations, and the master's dissertation of I&S Designer 1. 38 Three further websites were consulted: of the AYA care network, 39 of FfC, 40 and of I&S. 41 Observational data were collected during the most recent national AYA congress on the March 7, 201942 where the I&S project presented and discussed their findings. The researchers discussed the moment of data saturation at the end of the data collection process.
Ethical approval was granted by Erasmus Medical Centre Ethics Committee, no. MEC-2019-0232. The research data were solely managed by the lead researcher (P.V.).
Data analysis
A timeline and summary of the interviews and documents of each case study was developed and annotated. The data were iteratively coded and analyzed in Atlas.ti by the lead researcher (P.V.) (Appendix A2). Ambiguities were discussed and resolved with other researchers (M.d.D. and A.d.D.). First, the process of the PD projects was mapped over three PD phases: exploration; creation; test; and a fourth phase of implementation was added. Second, thematic and open codes were used to analyze the key events in each phase further. Given the large amount of data available, visualizations were made of the idea process development for FfC in Microsoft PowerPoint. Third, the most emphasized success factors of each case study were identified per PD phase and grouped in themes (Appendix A2). The variation between these themes was compared across case studies. Lessons were drawn from this comparison when success factors were present in all three case studies or if other case studies could benefit from applying insights from another case study.
Results
The FfC, I&S, and IM PD processes were at different stages at the time of data collection and all projects were still developing. The FfC PD process resulted in a new implemented food service 40 for the entire hospital, reaching a much wider target audience than AYAs alone, potentially being implemented in other health care institutions. I&S had developed a podcast, 43 two research articles about communication25,44 and a prototype website, 38 and IM developed a pilot study about communication about IM topics by caregivers. Across the case studies, seven themes were identified (Table 2).
Themes Identified Regarding the Use of Participatory Design to Develop Adolescent and Young Adult Care (Translated from Dutch)
Recruiting key local stakeholders directly exposed to the problem leads to synergy
The key stakeholders were interested in solving a problem that they had been previously exposed to. They were recruited in their local environment, where they were in contact with the problem, for example, at their workplace or where they studied, or at an event they attended. The dietician and the facility manager were recruited (FfC) at the hospital ward where the project was taking place. Designers were recruited (I&S) at a design school together with an AYA to present that project more vividly. AYAs were recruited (IM) through a national AYA conference 42 after a presentation on IM. During initial PD sessions, the “dreams” of each stakeholder to solve the problem were made explicit and each stakeholder was motivated to understand each other's dream. They therefore felt a shared experience of the problem and a joint mission to solve it together, as they realized that they could not solve the problem on their own. Joining all these stakeholders in this way leads to a “synergy.” They were enthusiastic to contribute their extensive experience to solve the problems, and they were motivated to create solutions. They also had networks of people who made important contributions such as a food designer and chef in FfC and a journalist in I&S. In summary, a synergy emerged when stakeholders were recruited with relevant experience in places where they were directly exposed to the problem.
Using design tools helps to explore the problem from different angles
Design tools were used to visualize what was being discussed. Broadly framing a problem can prove challenging, as indeed the IM stakeholders experienced, and it can take considerable time to gather information. In the I&S case, the problem was framed more narrowly with the help of Designers 1 and 2 by visualizing the problem through a mind-map (Fig. 1) and a so-called customer journey, which visualizes the journey of the patient (Fig. 2). The mind-map helped them to more easily discuss both solvable problems, such as improving communication, and more difficult problems, such as a system-wide health care change. To get a better understanding of the place and time of the communication problem, Designer 1 developed a customer journey based on interviews with AYAs and other stakeholders. This helped to pin down the communication problem in the complex referral process (Fig. 2).
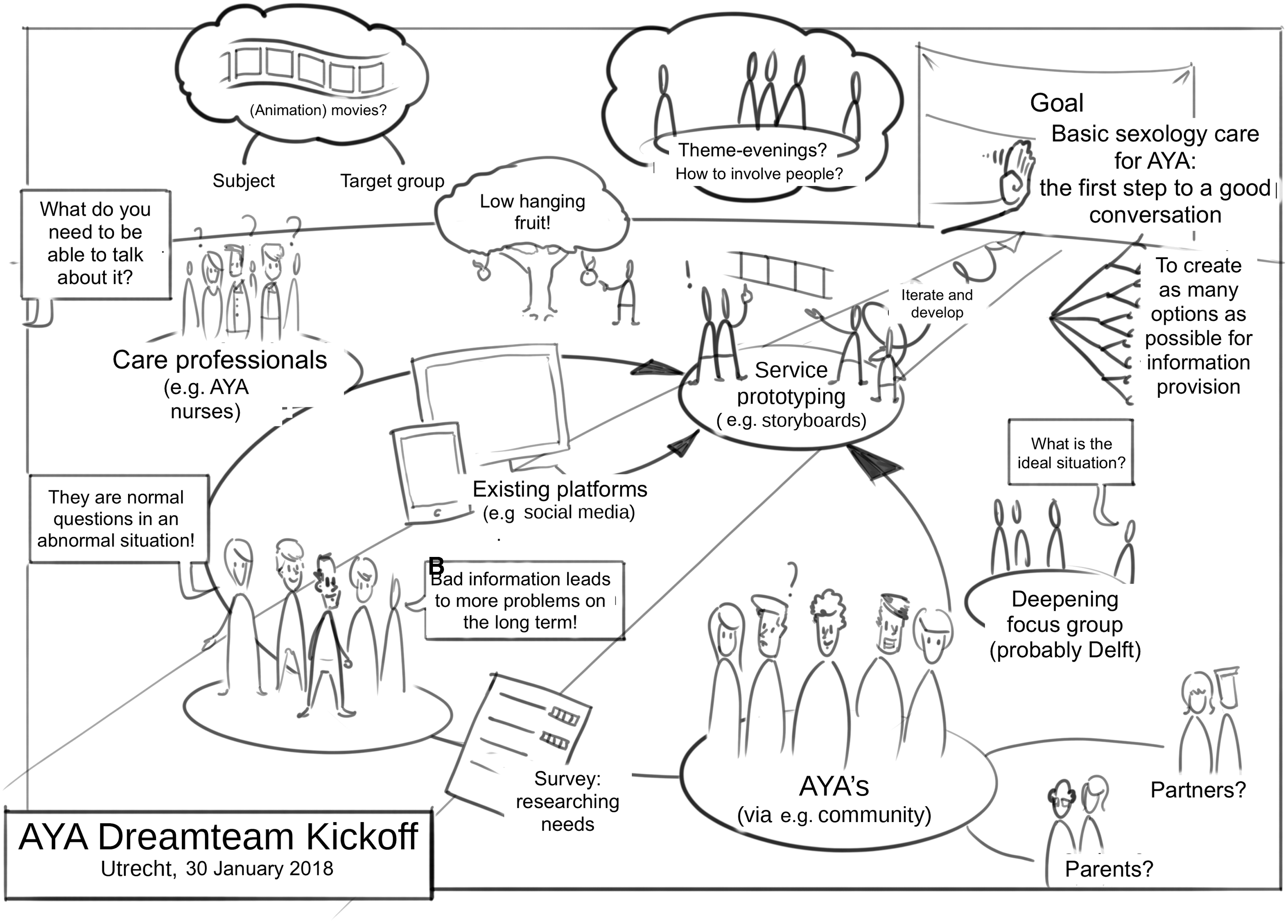
Mind-map visualizing problems and solutions by Designer 2 for the Intimacy and Sexuality case.
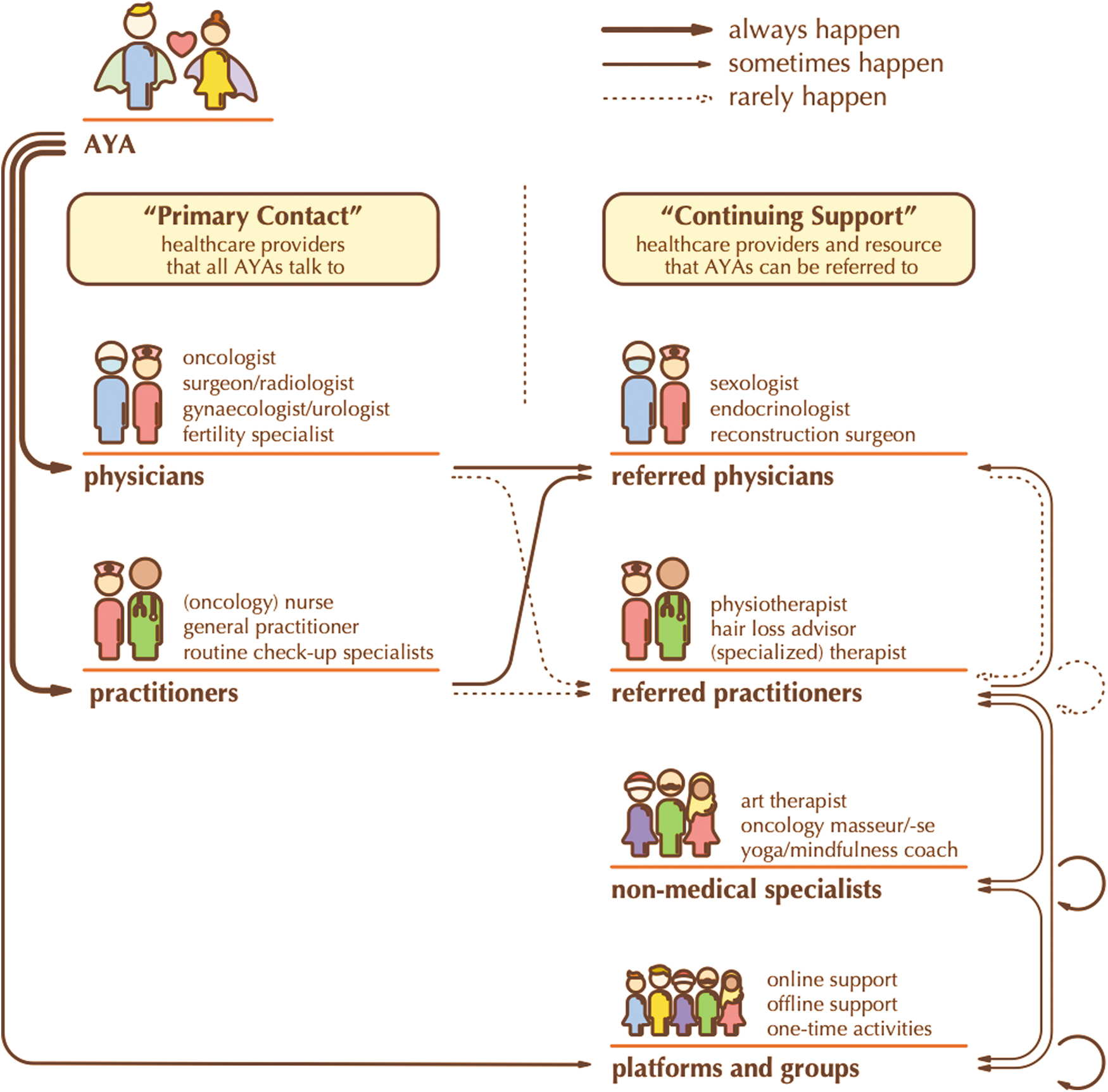
Customer journey visualizing the journey of the patient by Designer 1 for the Intimacy and Sexuality case.
By listening and conducting research, first a deeper shared understanding was created
The facilitators in each case explicitly invited everyone to share their own stories and dreams to improve care, and they actively sought AYA input. They facilitated an open and safe atmosphere that allowed empathy to grow between stakeholders and between the stakeholders and the problem. In doing so, the stakeholders became aware that their frustrations and dreams were similar and that connecting dreams worked synergistically. To further understand the communication problem identified in the I&S case, a survey was conducted. 25 The survey revealed that there was a misalignment in expectations about who should provide information, and that AYAs preferred to engage about this topic with nurses and sexologists. AYAs further indicated that the preferred mode of conversation was through a website, which contradicted the assumption made before the study that people would prefer an app.
Taking small steps toward a vision facilitates imagination
The Director of the AYA Care Network used particular wording to stimulate imagination and collaboration among stakeholders: “taking small steps” to make the progress achievable while holding on to “a vision on the horizon” to maintain a sense of direction. For example, the vision developed in the IM case included specialist nurses for complementary care, websites with reliable information, greater awareness, a referral network, and reimbursement structures. Combining an open approach with a sense of direction was crucial for some stakeholders, who felt that the problem was overwhelming. By having a direction, stakeholders could carry out activities outside the meetings and were seeking feedback in their own communities. A key challenge throughout the process was to keep that sense of direction, given that not everyone could attend every meeting. Health care professionals had conflicting agendas, and many had to combine what was voluntary work with their official job.
Respecting stakeholders in an equal collaborative environment fosters learning
Following the cocreation process of the AYA Care Network, the sharing of ideas and experiences was promoted by showing respect and empathy toward all stakeholders (Fig. 3). For instance, to emphasize that everyone would be involved equally in the process, the care professionals would not be allowed to wear white coats during the meeting and the Director of the AYA Care network, would use a virtual “eraser” at the start of meetings to emphasize the openness toward diverse backgrounds and cultures. This was important as the stakeholders were used to working in the hierarchical settings of health care institutions. The democratic environment that was created equalized the power relationships and stimulated knowledge sharing and knowledge integration, with each stakeholder contributing essential knowledge that others lacked.

Cocreation process of the AYA Care Network “The AYA Network way of doing things.”
Learning from each other about technical topics was important given the range of stakeholders. In the IM case, the oncologist presented an ethical framework (Appendix A3) that helped the other stakeholders understand how physicians define complementary care. In the FfC case, the idea was developed to use a “waiter” to encourage the patients, which was identified through a combination of patients' needs and the expertise of the Facility Manager (Fig. 4). Here, the knowledge of the Dietician also helped in sourcing ingredients to help patients recover. This was combined with the knowledge of the AYA cancer patients on what flavors and portions were desired.

Presenting food to AYA cancer patients in the Food for Care project: a result of integrating experiences of different stakeholders. AYA, adolescent and young adult. Photo printed with permission.
Designers and skilled people help to translate ideas into prototypes
The involvement of people such as designers or journalists could be decisive in coming up with potential solutions because other stakeholders realized that they needed someone with more creative skills to help them visualize their ideas about a solution. In the I&S case, Master's student designers took on the challenge to develop solutions, which were further developed by Designer 1. This designer developed further prototypes for an app, which were turned into a website following the survey, to provide information and guidance for AYAs with questions about I&S (Appendix A4). In the FfC case, a designer helped visualize the food dishes (Fig. 5), and a highly rated chef gave crucial input for producing the prototypes. Research has shown that the FfC project did improve the experience and health of patients.45,46 In the I&S case, a journalist experienced in sexuality communication helped to combine the knowledge of AYA cancer patients and sexologists in a podcast containing several episodes. 43

Prototype food dishes in the Food for Care project.
A hierarchical hospital environment, business considerations, and additionally required evidence prolong the PD process
Due to the success of the initial pilot study of the FfC prototypes service, the board of directors was highly impressed and wanted to explore the possibility to provide FfC for the entire hospital. At this point, there was a long delay in the process for various reasons. First, two extra pilot studies had to be conducted for different patient groups and the results had to be included in a revised business case. Second, negotiations regarding the business case with the board of directors and the catering company took longer than expected. Third, there were additional bilateral discussions between the hospital and the catering company as the food could not be prepared in the hospital kitchen and food assistants would have to be contracted by the catering company to provide the innovative formula for the entire hospital.
To overcome these hurdles of FfC, crucial attributes required of the AYA Director were described by other FfC stakeholders as being solution-oriented, daring and strategic, and being able to connect people. Once the Director of the AYA Care Network could no longer take part in the project, the hierarchical hospital environment resurfaced. Only after 2 years of piloting with other patient groups, developing a business case for the whole hospital and negotiations, was the business case accepted and the FfC ideas embedded in several of the hospital's wards. 40 Notably, the Facility Manager stressed that upscaling this project only seemed to be successful in those wards where a PD approach was used to redesign the original FfC service to meet the needs of their patients and the setting. Even though I&S and IM were not at the implementation phase, the challenge of the hierarchical hospital environment also resonated with them as they were consciously looking for solutions outside of the hospital frame to experiment with new forms of care. In addition, IM suffers from the image of quackery of “alternative medicine,” which meant that they had to be extra careful when starting a pilot study.
Discussion
Table 3 presents the key lessons from the three case studies and makes practical recommendations on how to develop a successful service or product for AYA care. To employ PD to develop care for AYAs, one needs to involve designers and skilled people, PD tools, and an open-ended approach to visualize and materialize new forms of care. Through the initiative of a designer to use PD tools, the I&S stakeholders were able to quickly identify the problem. Furthermore, the designer's skills were instrumental in both the I&S and FfC projects quickly developing prototypes. Furthermore, the skills of the journalist (I&S) and a highly rated chef (FfC) were crucial in developing prototypes. Using the inputs of a designer and other skilled people, and employing the PD tools in an open-ended way, helped all stakeholders to develop novel solutions they would not have thought of on their own.
Lessons and Practical Implications to Employ Participatory Design to Develop Adolescent and Young Adult Care
PD, participatory design.
In addition, recruitment and facilitation techniques helped to leverage knowledge and cooperation among the stakeholders. Stakeholders were brought together who had been exposed to a particular problem and had relevant expertise in the area. Each stakeholder was limited by their own field of knowledge, and the integration of this knowledge proved essential later in the prototyping process. The knowledge integration process was facilitated by creating an open-minded environment and equalizing power relationships by showing empathy and respect. Also, enabling the collaborative development of innovative care, participants found this approach to be highly satisfying and joyful.
Furthermore, the PD tools that the designers used helped to create a shared frame between stakeholders, in which new solutions could emerge. The mind-map in I&S, for example, set out the various ways in which one could frame the problem, that is, as an information “low hanging fruit” problem, as a conversational problem or as a service problem. The visualization of the food dishes in FfC helped the nondesigner stakeholders to frame the solutions as food dishes, rather than separate ingredients.
In line with earlier publications, the supportive role of design tools is highlighted as they help to share stories in a mutual language and build trust between staff and patients.11,47,48 The findings favor the use of creative PD tools over a research-focused PD approach that had been used in a previous AYA PD project.18,48 Involving a designer avoids “quick-fix” solutions – solutions which do not address the more fundamental underlying issues of a problem. 48 Furthermore, an open-ended approach is recommended in early design phases to enhance the creative process. 9
Similar to what this study highlights, others have also stressed the importance of recruitment10,12 and of knowledge integration.49–51 However, the relationship of recruitment and knowledge generation requires further examination. Facilitating a “beginner's mind set” is recommended as a way to overcome previous assumptions and iterate in the PD process. 12 To this end, stimulating a democratic environment and enabling mutual learning should be promoted as it is emphasized as a key aspect of PD.9,13,52
Turning to the implications for the development of AYA care, the findings highlight the need to integrate tools and techniques from PD in health care innovation practices. The hierarchical and clinical research-focused approach to delivering and developing care, which emphasizes high-level evidence from randomized controlled trials, is in sharp contrast to employing an open-ended creative design mind-set. Even though health care institutions are increasing multidisciplinary activities, these are still far from creative PD practices. As the deeply rooted cultural differences pose challenges, special attention should be given to highlighting the value of PD to health care stakeholders.47,48
Future recruitment strategies for using PD in an AYA setting could focus on identifying effective locations, where AYA care professionals, AYAs, and designers are based. In addition, financial and politically involved stakeholders could be approached at an early stage to hasten the implementation process. 17 To anticipate the implementation process, we would recommend engaging the manager of the cancer center and board members at an early stage. This may require some patience and slow the process down, but this patience may pay off later. The process may speed up due to their help to manage potential financial issues, building a robust business case, and advocating to other decision-makers within the often complex hierarchical hospital management structure. Furthermore, considering their involvement, one should try to explicitly discuss the need to conduct pilot studies early on so that data can be collected to demonstrate the required clinical and organizational value. To secure the longevity of the project, one should make sure that when replacing team members, one should communicate the required competencies clearly to avoid a conflict of interest.
A range of creative tell, make, and enact tools10,14 can be used to leverage the engagement of AYAs. Adopting an open-ended approach to manage these tools may be a significant contribution in the context of AYA care since this age group goes through a continuous identity construction process and a series of important life phases.2,16,53
Facilitating the PD process should not be underestimated in the AYA context given the need and value in respecting the various stakeholders. 17 Creating a safe and efficient process is perhaps even more crucial, given the limited time available to stakeholders employed in the health care sector. Elsewhere, it has been suggested that momentum in the PD process can be built through ownership and inclusion in ideation, setting expectations, and encouraging a critical attitude to constraints. 48 Furthermore, these facilitation techniques may be particularly crucial in sustaining the PD process when moving from a design testing phase 12 to an implementation phase, as was seen in the FfC project.
The main limitations of this study are related to the data collection process as only key stakeholders were interviewed and there were no direct observations of meetings. Interviewing more stakeholders of each type of stakeholder could enrich the findings and provide more interdisciplinary insights. Possible insights may have been missed due to recall bias, given that this was a complex interactive process. Nevertheless, a comprehensive image of events was reconstructed through triangulating a range of data sources. Although each case study was focused on a different problem, involving different stakeholders, one may still question the generalizability of the lessons drawn. Future research could validate the findings by examining PD applications in other, non-Dutch, AYA projects.
Conclusions
For a PD process to successfully develop care for AYAs, one needs to use designers and skilled people, PD tools, and an open-ended approach to visualize and materialize new forms of care. Furthermore, recruitment and facilitation techniques help leverage knowledge, raise awareness among stakeholders of different perspectives, and create a synergy in a democratic environment between stakeholders.
Footnotes
Acknowledgment
The authors acknowledge the research assistance of Ramon van Aert and Radboud University Medical Centre, Nijmegen for enabling the food project and Jaap Buis for supporting the food project.
Author Disclosure Statement
There are no competing financial interests.
Funding Information
No funding was received for this article.