
Abstract
Background:
Some experts recommend specific ventilator settings during nebulization for mechanically ventilated patients, such as inspiratory pause, high inspiratory to expiratory ratio, and so on. However, it is unclear whether those settings improve aerosol delivery. Thus, we aimed to evaluate the impact of ventilator settings on aerosol delivery during mechanical ventilation (MV).
Methods:
Salbutamol (5.0 mg/2.5 mL) was nebulized by a vibrating mesh nebulizer (VMN) in an adult MV model. VMN was placed at the inlet of humidifier and 15 cm away from the Y-piece of the inspiratory limb. Eight scenarios with different ventilator settings were compared with endotracheal tube (ETT) connecting 15 cm from the Y-piece, including tidal volumes of 6–8 mL/kg, respiratory rates of 12–20 breaths/min, inspiratory time of 1.0–2.5 seconds, inspiratory pause of 0–0.3 seconds, and bias flow of 3.5 L/min. In-line suction catheter was utilized in two scenarios. Delivered drug distal to the ETT was collected by a filter, and drug was assayed by an ultraviolet spectrophotometry (276 nm).
Results:
Compared to the use of inspiratory pause, the inhaled dose without inspiratory pause was either higher or similar across all ventilation settings. Inhaled dose was negatively correlated with inspiratory flow with VMN placed at 15 cm away from the Y-piece (rs = −0.68, p < 0.001) and at the inlet of humidifier (rs = −0.83, p < 0.001). The utilization of in-line suction catheter reduced inhaled dose, regardless of the ventilator settings and nebulizer placements.
Conclusions:
When VMN was placed at the inlet of humidifier, directly connecting the Y-piece to ETT without a suction catheter improved aerosol delivery. In this configuration, the inhaled dose increased as the inspiratory flow decreased, inspiratory pause had either no or a negative impact on aerosol delivery. The inhaled dose was greater with VMN placed at the inlet of humidifier than 15 cm away the Y-piece.
Introduction
Aerosol therapy is commonly used in patients undergoing mechanical ventilation (MV), with reported utilization rates ranging from 22% to 25% in various patient populations.1,2 Unlike ambulatory patients, ventilatory support requires in-line placement of aerosol generators to ensure uninterrupted MV. 3 However, aerosol delivery during MV is influenced by several factors, including positive pressure and constant flow inside the circuit.4,5 Specifically, lower base flow and placing a nebulizer farther from the Y-piece have been shown to increase the inhaled dose.4,6,7 Longer inspiratory time and lower inspiratory flows have also been found to improve aerosol delivery efficiency.
The expert group published consensus recommendations that ventilator settings should not be changed for the sole purpose of increasing aerosol delivery during MV. 3 However, several panel experts advocated that administration of antibiotics should consider specific adult ventilator parameters, including a tidal volume (VT) of 8 mL/kg, an inspiratory to expiration ratio (I:E) of 1:1, respiratory rates (RRs) of 12–15 breaths/min, and an inspiratory pause time (Ti-pause) at 20% of inspiratory time (Ti). To mitigate patient-ventilator asynchrony and alleviate patient discomfort associated with these ventilator settings, a high dose of sedation, even paralytics, has also been recommended.8,9 However, the comparative advantages of these recommendations over conventional ventilation settings in aerosol delivery remains unclear and additional exploration of those settings on aerosol delivery efficiency seemed warranted.
Moreover, several settings are interrelated and adjusting one parameter may affect others. For example, an increased flow can lead to a shorter inspiratory time, a lower inspiratory to expiratory ratio, and a smaller duty cycle (defined as inspiratory time divided by total cycle time). 10 However, most previous studies have focused on investigating individual settings, making it difficult to identify the key determinant of aerosol delivery during MV.11–17 In addition, the impact of the ventilation settings on aerosol delivery during MV has been primarily assessed using a jet nebulizer (JN) or pressurized metered dose inhaler,13–17 while limited comparisons are reported on the interaction of those settings with vibrating mesh nebulizers (VMNs), 18 which are commonly utilized for MV patients.
Importantly, the benefits of incorporating a long inspiratory pause remain unclear. Therefore, this study aimed to investigate the effect of different ventilator settings on aerosol delivery via VMNs during MV. We hypothesized that adding the inspiratory pause would increase drug deposition.
Materials and Methods
An adult ventilator (Puritan Bennett™ 980; Medtronic, Inc., Minneapolis, MN) was connected to a heated passover humidifier (MR850; Fisher & Paykel Healthcare, Inc., Auckland, New Zealand) through a dual limb adult circuit, with temperature set at 37°C, and then to a 7.5-mm endotracheal tube (ETT). A collecting filter (VADI Medical Technology Co., Taiwan) was connected between the ETT and a test lung with compliance of 30 mL/cmH2O and resistance of 5 cmH2O/L/s (SmartLung, IMT analytics, Buchs, Switzerland) (Fig. 1).
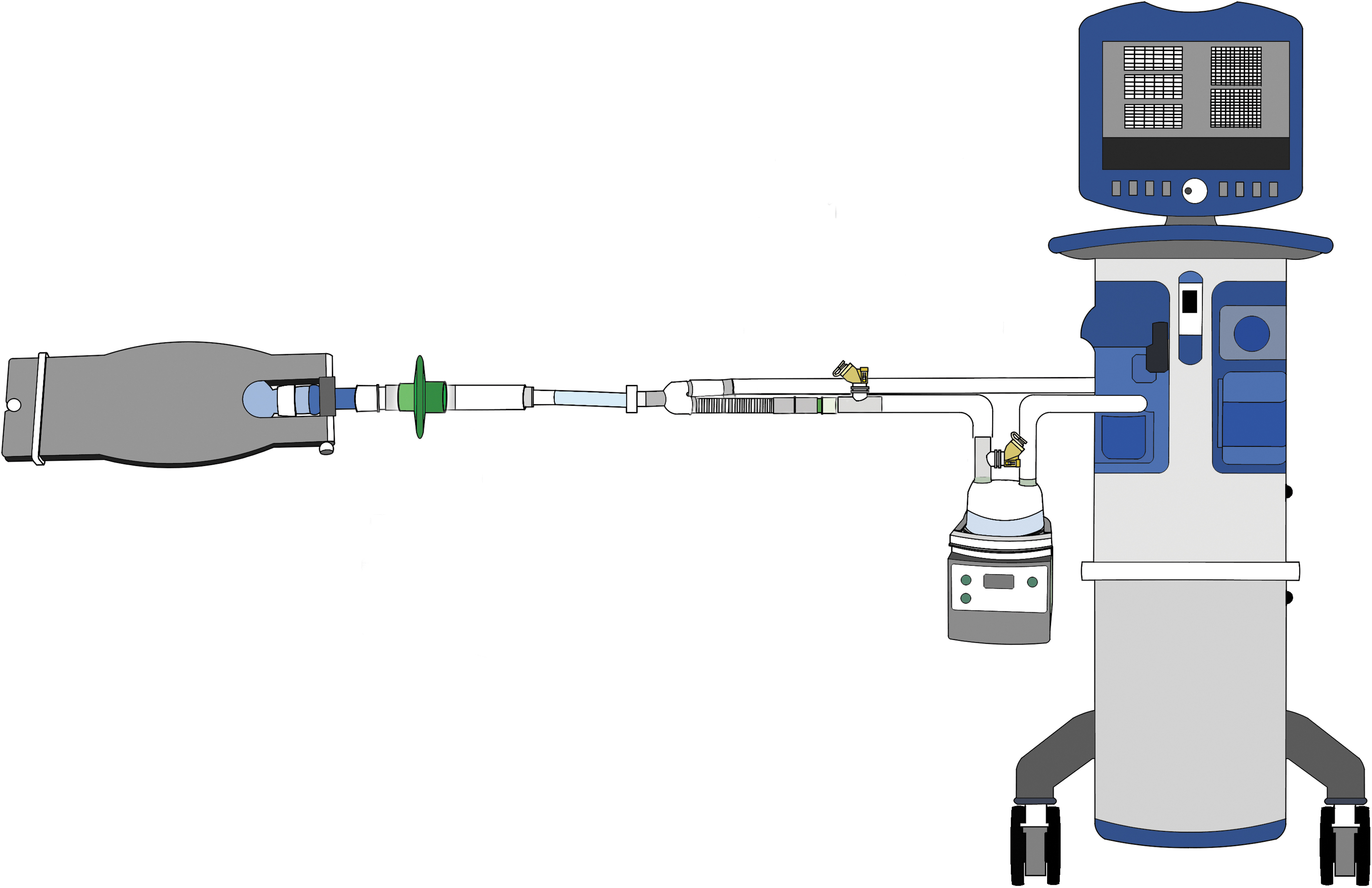
Experimental setup. A VMN was placed either at 15 cm away from the Y-piece of an inspiratory limb or at the inlet of humidifier. VMN, vibrating mesh nebulizer.
Table 1 lists eight ventilator settings used in the study, designed for a hypoxemic patient with low lung compliance and a weight of 70 kg. The volume-targeted assist-control mode was utilized with square flow pattern. VT was set at 420 and 560 mL (equivalent to 6 and 8 mL/kg), positive-end expiratory pressure at 8.0 cmH2O, RRs of 12, 16, and 20 breaths/min, I:E ratios of 1:1 and 1:2, with and without inspiratory pause (Ti-pause) (Table 1).
Ventilator Settings for the Experiment
DC, duty cycle = Ti/TTOT; I:E, inspiratory time to expiratory time; RR, respiratory rate; Ti, inspiratory time; Ti-pause, inspiratory pause time; TTOT, total breathing cycle time; VCV, volume control ventilation; VT, tidal volume.
To evaluate the impact of an inline suction catheter on aerosol delivery, an additional experiment was conducted using an inline suction catheter (Pacific Hospital Supply Co., Ltd., Miaoli, Taiwan) with two subsets of settings (G and H) with VT 8 mL/kg, I:E of 1:2, and RR 20 breaths/min. These settings were consistent with those typically used for treating hypoxemic patients. 19
A VMNs (Aerogen Solo™; Aerogen Ltd, Galway, Ireland) was placed at the inlet of humidifier and 15 cm away from the Y-piece in the inspiratory limb. A unit-dose Ventolin nebule (GlaxoSmithKline, Inc., Victoria, Australia), containing salbutamol 5.0 mg/2.5 mL, was loaded into the drug reservoir and nebulized until no aerosol was visible. For each of the eight breathing pattern, a new VMN was used, and each experimental setting was repeated five times (n = 5). Nebulization time was recorded to ensure consistent VMN performance throughout the study.
Collecting filters were disassembled, eluted with 10 mL of distilled water, and then gently agitated for 2 minutes. The delivered drug was analyzed using an ultraviolet spectrophotometry (ThermoFisher Scientific, Inc., Waltham, MA) at a wavelength 276 nm. An absorption—concentration correlation of salbutamol was predetermined between 2.0 and 250 μg/mL with a slope of 0.0068 (R 2 = 0.9996). Salbutamol drug mass was calculated from the absorption-concentration standard curve, and was calculated into percentage of total initial dose (inhaled dose).
Data analysis was conducted using a statistical software (SPSS 26.0, IBM, Armonk, NY) and Prism GraphPad program (GraphPad Software, Boston, MA). Data were reported with mean and standard deviation. Comparisons of the inhaled dose between two placements and each pair of setting with/without Ti-pause were analyzed by Mann–Whitney test, while Kruskal–Wallis test was performed to compare inhaled doses across different ventilator settings. Spearman's correlation coefficients were computed for correlations among the inhaled dose and inspiratory flow and duty cycle. To account for the confounding factors, an additional partial correlation coefficient between the inspiratory flow and the inhaled dose was used. The level of statistical significance was set at p < 0.05 (two-tailed).
Results
Regardless of the ventilator settings, placing the VMN at the inlet of the humidifier resulted in a greater inhaled dose (all p < 0.001). When comparing the use of inspiratory pause time, it was observed that the inhaled dose with no inspiratory pause time was either higher or similar across all ventilation settings (Fig. 2).
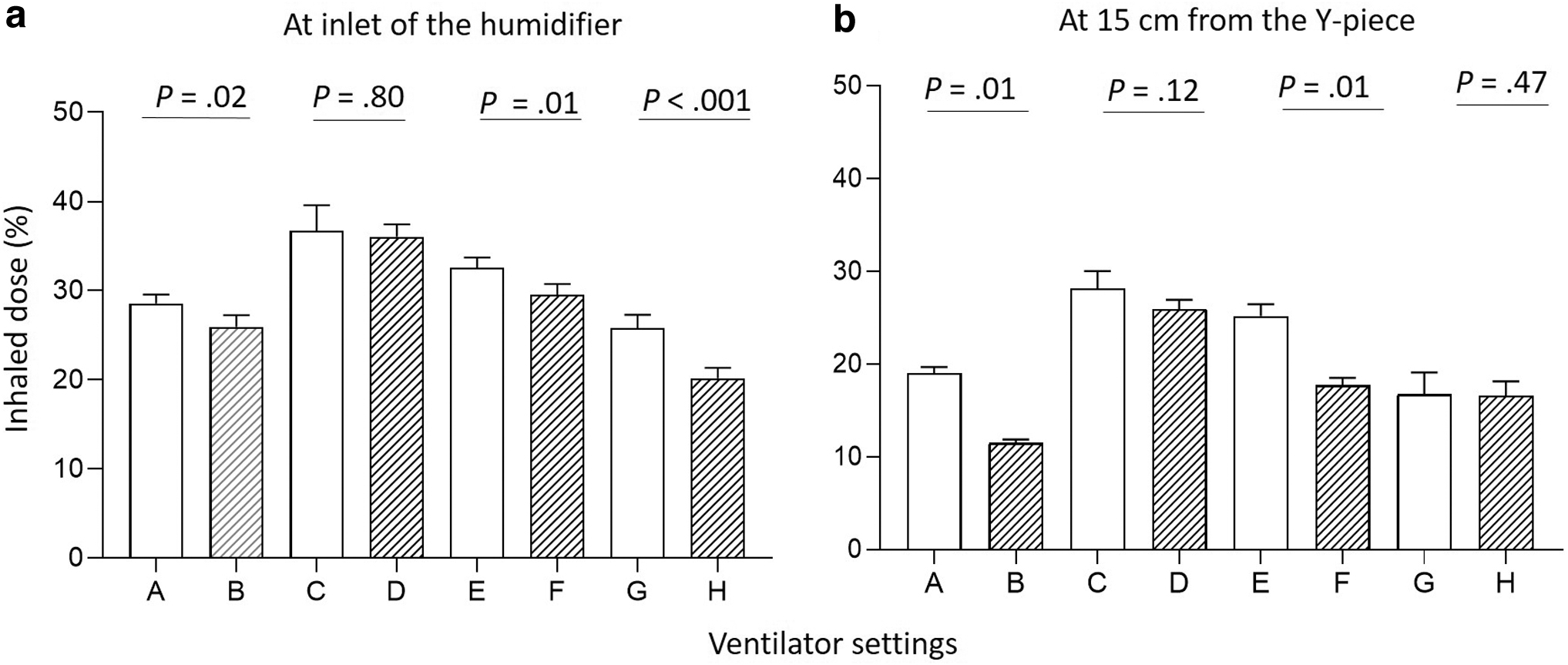
Comparisons of the inhaled dose with and without an inspiratory pause across different ventilator settings. Inhaled doses (mean ± SD) without an inspiratory pause (clear bars) versus with an inspiratory pause (bars with slash lines). Nebulizer was placed at the inlet of humidifier
With both nebulizer placements, the inhaled doses among the eight ventilator settings were significantly different (both p < 0.001). Specifically, in cases where VT (560 mL) and I:E (1:1) were the same (C and E, D and F), higher RR (12 vs. 20 breaths/min) resulted in lower inhaled doses (Fig. 3a). When the I:E ratio was the same (1:2) with similar Ti and Ti-pause (A and G, B, and H), the combination of larger VT with higher RR (560 mL with 20 breaths/min vs. 420 mL with 16 breaths/min) did not lead to an increase in the inhaled dose (Fig. 3b). However, larger VT and higher RR did increase the inhaled dose when the inspiratory flow and Ti-pause were the same (A and E, B, and F) (Fig. 3c). These findings were consistent for both nebulizer placements.
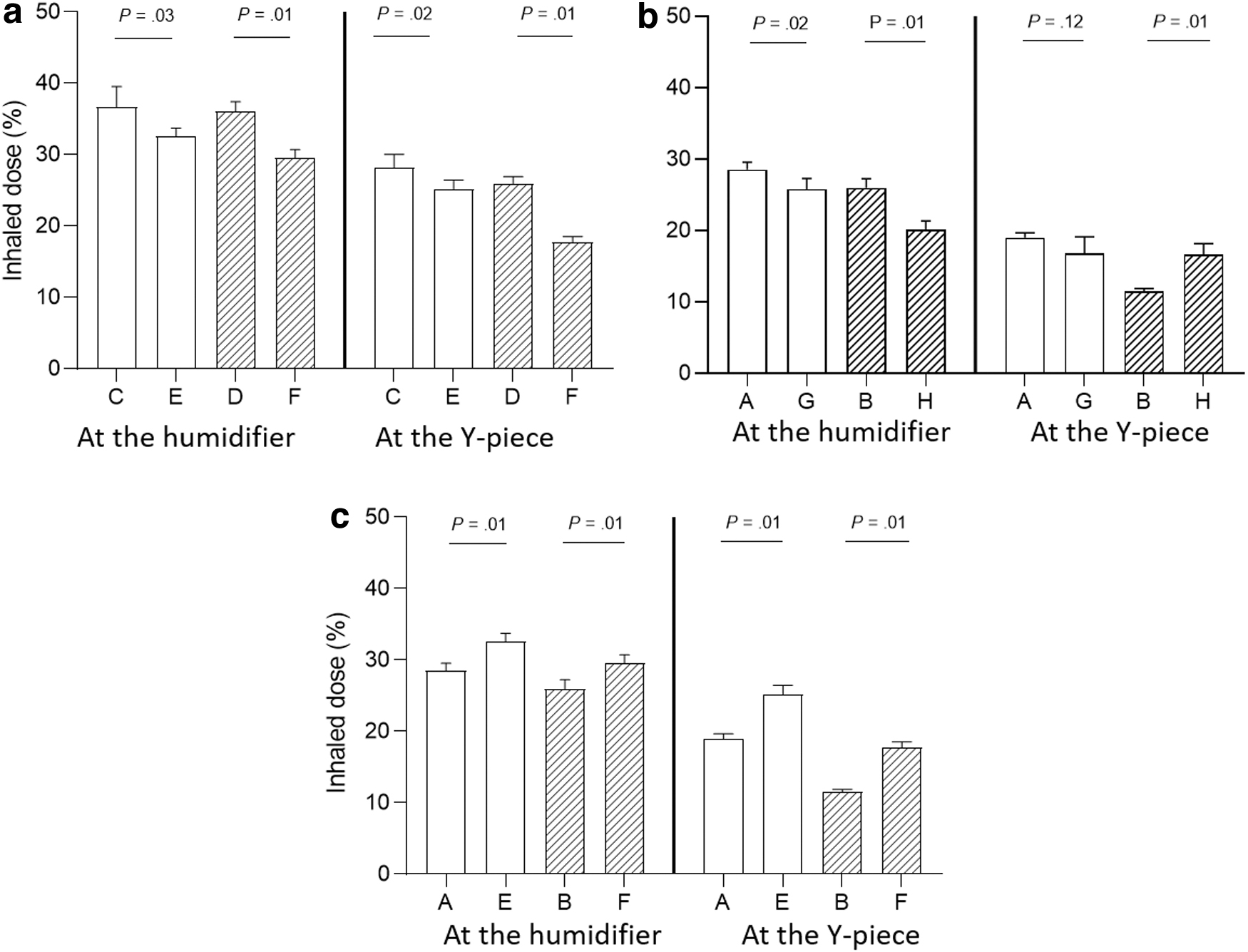
The impacts of VT, RR, I:E, and inspiratory flow on the inhaled dose. Comparisons of the inhaled dose for ventilator settings with nebulizer placed at the inlet of humidifier and 15 cm away from the Y-piece. With the same settings of VT and I:E (1:1)
When evaluating the relationship between the inhaled dose and inspiratory flow, Spearman's correlations showed a negative correlation, with rs = −0.83 (p < 0.001) when VMN was placed at the inlet of humidifier (Fig. 4a) and rs = −0.68 (p < 0.001) when placed 15 cm away from the Y-piece (Fig. 4b). The relationship between the inhaled dose and duty cycle demonstrated a moderate correlation when the VMN was placed at the inlet of humidifier (rs = 0.69; p < 0.001) and 15 cm away from the Y-piece (rs = 0.43; p < 0.001). Accounting for confounding factors, an additional partial correlation coefficient between inspiratory flow and inhaled dose showed a moderate correlation (r = 0.59; p < 0.001), with controlled variables, including VT, Ti-pause, RR, and Ti.
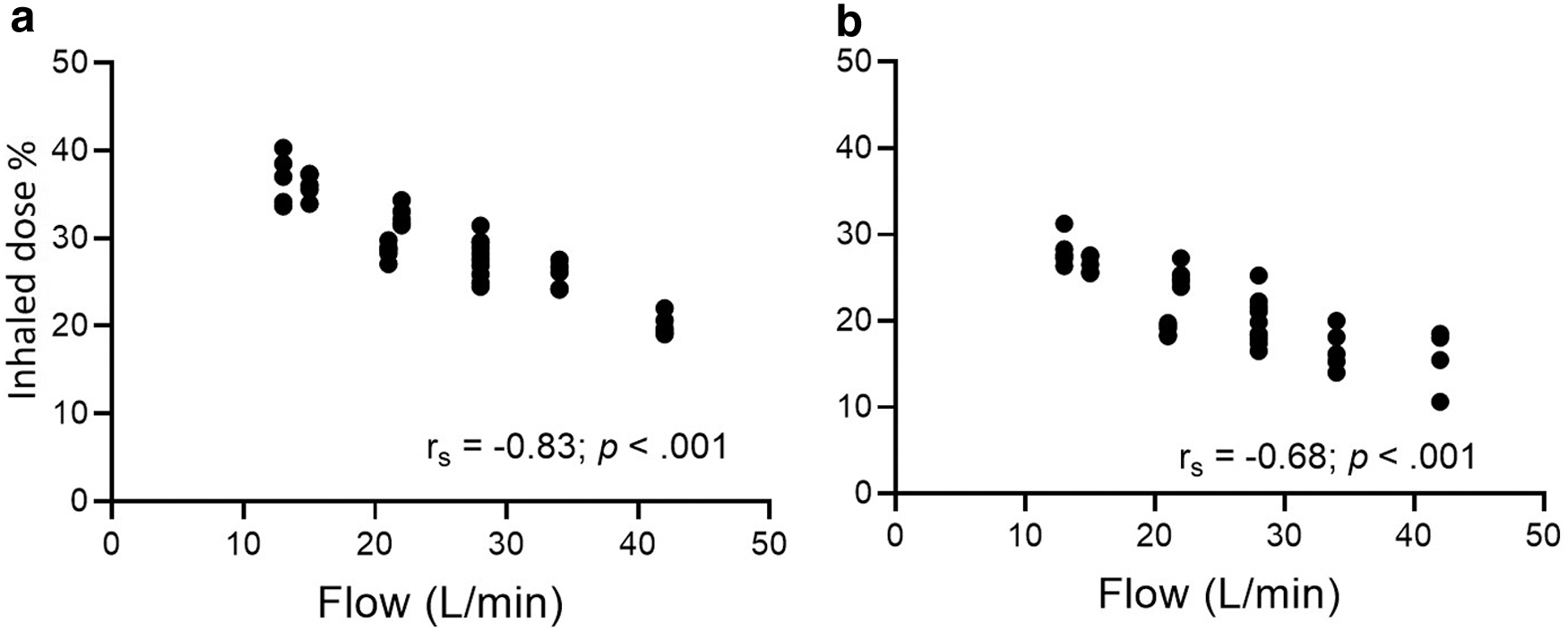
Correlations between the inhaled dose with inspiratory flow. Nebulizers were placed at inlet of heated humidifier
Irrespective of the ventilation settings, the inhaled dose was consistently higher when the nebulizer was placed at the inlet of humidifier compared to when it was placed 15 cm away from the Y-piece (Fig. 2; p < 0.001). Furthermore, the presence of an inline suction catheter resulted in 5%–6% lower inhaled dose than scenarios without a suction catheter (Fig. 5).
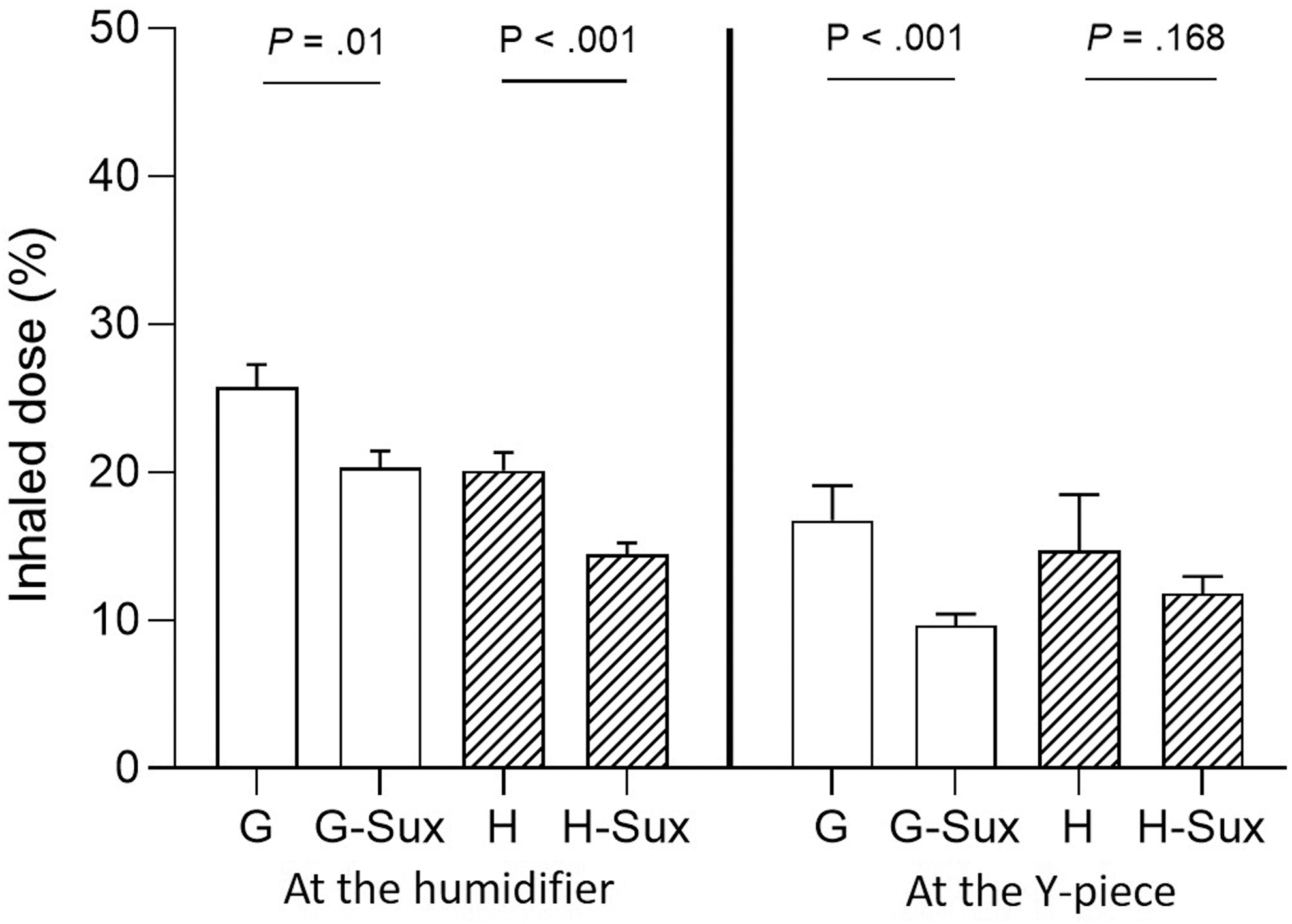
Comparisons of inhaled dose with versus without an inline suction catheter with two nebulizer placements. Ventilator settings were VT 560 mL, RR 20 breaths/min, Ti 1.0 seconds, and I:E of 1:2 and without Ti-pause (G) and with 0.3 seconds Ti-pause (H), with nebulizer placed at two nebulizer placements. Sux: with an inline suction catheter; bars with slash lines: setting with a Ti-pause.
Discussion
To the best of our knowledge, this study marks the inaugural exploration of the impact of inspiratory pause on aerosol delivery during MV. Our results revealed that the inhaled doses were either lower or similar when compared to breathing patterns with no inspiratory pause, and these differences varied with ventilator settings. Our findings confirm previous reports of a strong correlation between the inhaled dose and inspiratory flow. Specifically, as the inspiratory flow decreased, the inhaled dose increased. Furthermore, the presence of an in-line suction catheter consistently reduced aerosol delivery.
During MV, aerosols are transported by the ventilator gas during the inspiratory phase. Higher flow induces more turbulence, resulting in greater impactive drug deposition in the circuit. This observation may account for the inverse relationship we identified between the inhaled dose and inspiratory flow. These findings align with a previous study that investigated the aerosol delivery of a VMN during MV, where the authors reported a lower inhaled dose as the inspiratory flow increased from 40 to 80 L/min. 17 In contrast, Vecellio et al. found no significant differences in the inhaled dose with inspiratory flows ranging from 14.4 to 37.5 L/min when using an inspiratory synchronized JN during MV. 13 The discrepancies between these studies and our findings can be explained by the different mechanisms of the three aerosol generators.
Unlike VMN, JN is driven by an external gas, typically at 6–8 L/min. Inspiratory synchronized JN utilizes a portion of the gas intended for patient delivery during tidal breathing, potentially resulting in variations in total gas flow used to carry the aerosols.
While lower flows have been shown to increase aerosol delivery with a VMN during MV, it is important to consider that low inspiratory flow settings may require longer inspiratory time and extended I:E to deliver the same VT in volume control modes, especially when constant flow pattern is utilized. This can lead to patient's discomfort and flow starvation, necessitating the use of sedation and/or paralytics to eliminate patient-ventilator asynchrony. In addition, shortened expiratory time carries risk such as air trapping, particularly in patients with obstructive airway diseases, which can potentially decrease cardiac output as increased transthoracic pressure reduces venous return. In our study, when the VMN was placed at the inlet of humidifier and the same VT (560 mL) and RR (20 breaths/min) were used, reducing the inspiratory flow from 34 to 22 L/min increased the mean inhaled dose from 26% to 33%.
However, this came at the cost of decreasing I:E from 1:2 to 1:1, thereby increasing the risk of patient discomfort and air-trapping. Likewise, transitioning from the conventional setting (VT 6 mL/kg, RR 16 breaths/min and I:E 1:2) to the setting (VT 8 mL/kg, RR 12 breaths/min and I:E 1:1) recommended by the inhaled antibiotics expert group resulted in a modest increase in the mean inhaled dose from 28% to 37%,8,9 but would require the use of sedation or even paralytics. Thus, the potential benefits of improving aerosol delivery through these settings, may not justify the associated risks. Interestingly, a multicenter observational study investigating the use of inhaled polymyxin B to treat extensive drug‑resistant gram‑negative ventilator‑associated pneumonia utilized the recommended ventilator settings during nebulization. 20 However, they did not find significant improvements in the mortality with and without the utilization of inhaled polymyxin B.
Finally, although inspiratory pause has been recommended,8,9 our study found that the use of inspiratory pause did not increase aerosol delivery, likely due to the increased inspiratory flow when inspiratory pause is used. Therefore, in our recently published consensus on aerosol delivery via MV, changing ventilator settings was not recommended. 3 It should be noted that our study did not involve the use of inhaled antibiotics. Future studies investigating the impact of inspiratory flows and inspiratory pause on aerosol delivery across different drug formulations during MV may be warranted.
Consistent with previous studies,4,6,7 our findings demonstrate a greater inhaled dose with VMN placed at the inlet of humidifier compared to its placement close to the Y-piece. Notably, at this placement, we observed a strong correlation between the inhaled dose and inspiratory flow, while a moderate correlation was noted between the inhaled dose and the duty cycle. The distinction could potentially be attributed to the lack of consideration of inspiratory pause in the duty cycle calculation. Aerosols are inhaled during active inspiration when a gas flow is generated and there is no gas flow during inspiratory pause.
We observed that the use of in-line suction catheter resulted in a reduction of 5%–6% in the inhaled dose, which is consistent with the finding reported by Williams et al. 21 One may suggest to remove suction catheter during nebulization to mitigate this impact; however, it is essential to carefully assess the risks and benefits of this practice. Removing the suction catheter before nebulization and later reconnecting it would necessitate breaking the ventilator circuits twice, potentially leading to the dissemination of condensation and secretions in the surrounding environment. Moreover, this process might cause desaturation due to alveoli derecruitment. Notably, Williams et al. found that the shape of the suction catheter affected the aerosol delivery, using a streamline shape might help improve aerosol delivery.
There are several limitations in this study. First, it was an in vitro study, the findings could not be directly applied to clinical practice. The complex anatomy and pathophysiological factors present in actual patients may impact the aerosol delivery differently. Moreover, our study did not incorporate exhaled heat and humidity, which are important physiological factors that could influence aerosol delivery. 18 Furthermore, our study had limitations in terms of the range of settings explored. Specifically, we only used two VT, three RR, two I:E, three Ti-pause, and four Ti settings, which limited our ability to fully explore the correlation between these variables with the inhaled dose. Further analysis to determine the individual contribution and power of each variable was also constrained.
Future studies should aim to include a wider range of settings, especially in vivo studies conducted with real-life ventilation settings, to better understand the key influential factors in aerosol delivery via MV. Finally, we did not measure circuit losses and expiratory filter losses, future studies on the inhaled mass measurement may be warranted.
Conclusion
Placing VMN at the inlet of humidifier had the greatest effect on improved aerosol delivery during MV, followed by attaching the ventilatory circuit directly to the ETT. In this configuration, the inhaled dose increased as the inspiratory flow decreased. However, it is important to carefully weigh the advantages of improved aerosol delivery against the potential drawbacks associated with decreasing flow settings. In addition, our findings indicate that the use of inspiratory pause either had no impact or resulted in a negative effect on aerosol delivery. These findings underscore the need for a balanced evidence-based approach to optimize aerosol delivery.
Footnotes
Authors' Contributions
J.L. conceived this project. H.-L.L. and J.L. conducted the study, H.-L.L. performed the data analysis. H.-L.L. and J.L. drafted the article, J.B.F supervised the project and provided critical edits on the article. All authors reviewed and approved the article.
Author Disclosure Statement
J.L. discloses relationships with the Rice Foundation, the American Associate for Respiratory Care, Fisher & Paykel Healthcare Ltd, Aerogen Ltd, and Heyer Ltd. J.L. also serves as a section editor for RESPIRATORY CARE. J.B.F. is Chief Science Officer for Aerogen Pharma Corp. H.-L.L. discloses relationships with Chang Gung Memorial Foundation.
Funding Information
No funding was received for this article.
Reviewed by:
Ann Cuccia
Arzu Ari