
Abstract
Objectives:
Reiki is an energy medicine type, with growing evidence for its benefit for various conditions and populations. The “energy” in energy medicine implies a life force rather than a conventional physics definition. Many people feel they can perceive this energy through extended perception beyond their traditional five senses. This study's objectives were to evaluate extended perception during Reiki energy medicine sessions.
Design/Methods:
Six expert Reiki Masters (RMs) gave 30-min sessions to 40 participants. Participants had one or more conditions: acute physical injury (such as broken bone), mental symptoms of memory loss, and psychological symptoms (anxiety and/or depression). Six people vetted for extended visual perception made observations before, during, and after sessions using quantitative and qualitative measures. Participants and RMs also recorded their observations. Data were analyzed for corroboration: (1) within-perceivers, (2) between the RM and perceivers, (3) between the participant and RM, and (4) between the participant and perceivers. Participants' well-being outcomes and potential predictors were also evaluated.
Results:
Well-being improved after the sessions [F(3, 159) = 12.3, p < 0.00005; baseline −55.7 ± 18.8, before −58.9 ± 18.1, after −73.2 ± 16.2, 1-week later −64.3 ± 20.3; effect size is 0.61, 95% confidence interval [0.39–0.59]). The perceivers generally reported similar information in free-form drawings and free text. Perceivers' observations about the participants' health were highly corroborated and matched participants' self-reports. Further, the symbolic information that perceivers noted was meaningful to the participants, but perceivers did not see the same symbols nor ascribe the same meaning to them.
Conclusions:
Future studies must refine the methods developed here to continue exploring the extended perception's validity and practical application in health care.
Clinical Trial Registration:
ISRCTN16257705.
Introduction
Reiki is an energy medicine technique, also called biofield therapy, that originated in Japan, based on the principle that the therapist can channel energy into the patient, activating the natural healing processes of the patient's body to restore physical and emotional well-being. 1 Health care settings have incorporated Reiki 2 and observed positive outcomes for various conditions and populations.3–6
In Reiki, the word “energy” refers to a felt sense that therapists describe as energetic-like, magnetic-like, or tingling-like sensations in or around the body rather than definitions physicists might use. Experimental and anecdotal reports demonstrate that physical measures correlate with these feelings, for example, electromagnetic and magnetic fields,7,8 mechanical vibrations, 9 and other less conventional approaches. 10 However, there is currently no reliable detection method to assess when the presumed energy is present.
Extended perception, the ability to perceive information beyond our traditional five senses, is present throughout humanity's recorded history. 11 Many practical applications demonstrate its veracity,12,13 including informing medical diagnoses,14–17 despite no verified materialist mechanism of action.
In a case study, we included a perceiver (i.e., an individual with the capacity to perceive information beyond the traditional senses) to investigate their ability to sense and describe the energy exchanged between a practitioner and the recipient during various energy medicine modality sessions. 18 Qualitative analysis of the observations revealed common themes about the exchange (e.g., energy attributes between the practitioner/participant and the space around them).
Informed by this case study, this study examines one healing modality (i.e., Reiki) in a larger sample (i.e., 6 practitioners and 40 receivers) to further explore the possibility that the perceiver observations could elucidate how energy medicine works. This exploratory study focused on five primary questions: (1) do different perceivers perceive in a similar manner? (2) do perceivers, Reiki Masters (RM), and recipients (here referred to as participants) experience the healing modality in a similar fashion? (3) specific to symbolic information, does the meaning ascribed to symbols by the perceivers agree with the meaning ascribed by participants? (4) can perceivers accurately perceive the participant's health before the session? (5) does participants' well-being improve from the session, and what, if any, variables predict those improvements?
Methods
The Institute of Noetic Sciences (IONS) Institutional Review Board (IORG No. 0003743) approved all study activities. The study was pre-registered at the Open Science Forum (osf.io/vzxqf) and registered at the ISRCTN registry (ISRCTN16257705). Measure details are listed in Supplementary Data S1.
Recruitment
Participants
Forty participants were recruited using multiple methods such as IONS membership and network, NextDoor, Craigslist, and Facebook from June 22, 2021 to August 5, 2021. Interested volunteers completed an initial informed consent to proceed to the screening questions. Inclusion/exclusion criteria were: (1) aged 18 years or older, (2) no COVID-19 symptoms, (3) agree to Reiki session at the site, (4) willingness to complete study activities, and (5) current presence of one of the following: physical injury, memory loss symptoms, anxiety, or depressive symptoms.
These symptom categories were chosen to ensure variability in the symptoms that participants were experiencing and because Reiki practitioners purport that it is beneficial for anyone for any condition. Further, having heterogeneous participants allows for greater generalizability of the results.
This question determined injury: “Have you had an acute physical injury within the last four weeks (e.g., recent sprain, strain, fracture, or broken bone)?” The date of injury, injured body part, and presence of any removable supportive device were collected, if applicable. Memory loss, anxiety, and depressive symptoms inclusion scores were: <15 on the Inoue Computerized Test Battery, 5 to 15 on the Generalized Anxiety Disorder-7 (GAD-7), and 16 to 25 on the Center for Epidemiologic Studies Depression Scale (CESD-5), respectively. Participants with scores higher than 15 on the GAD-7 and 25 on the CESD-5 could be enrolled if under the care of a mental health provider and at the principal investigator's discretion.
Recruitment produced 174 responses, of which 156 met inclusion/exclusion criteria and 139 left contact information and were screened (Fig. 1). Forty qualifying volunteers were accepted on a first-come, first-serve basis. Participants received $100 for participation.

Consort flow diagram.
Reiki Masters
Five RMs were recruited through the IONS network, the International Center for Reiki Training, and the Center for Reiki Research with at least 10 years of regular Reiki experience as their primary modality in any tradition or lineage determined by self-report (i.e., experience was not formally verified). The RMs received $1000 and were reimbursed for travel expenses, if applicable.
The perceivers were uncomfortable with one RM's energy, and a sixth replacement RM was recruited. The RMs were five females and one male, 57.5 ± 7.6 years of age with 20.2 ± 3.4 years of education. All but one identified as European, who identified as Middle Eastern. The RMs had an average of 17.7 ± 4.7 years of experience, having conducted ∼2333.3 ± 2137.0 sessions.
Perceivers
Twenty-nine referred perceivers were contacted through the IONS network, and 14 interviews were conducted. Inclusion/exclusion criteria for perceivers were: (1) professional experience, (2) ability to observe external visual phenomena associated with energy, such as external colors, movement, and light and internal visual impressions, and (3) willingness to stay neutral (i.e., not influence the session through their potential healing abilities).
Potential perceivers provided the principal investigator with a session to demonstrate their skills. Only those who perceived substantial accurate information were invited to participate. Six perceivers were selected with the following characteristics: female, 53.3 ± 14.6 years of age with 17.0 ± 3.0 years of education, and all but one identified as European, who identified as Asian. They had 13.2 ± 9.3 (range 2–25) years of extended perception experience and approximately client sessions (range 500–6000).
Two men were interviewed, one declined participation, and the other did not provide accurate information. Perceivers received $4000 and accommodation and travel expense reimbursement. Perceiver training/certifications included a Master Certificate of Intuition Medicine from the Academy of Intuition Medicine, Barbara Brennan School, indigenous shamanic visioning skills, the Berkeley Psychic Institute, and innate abilities often starting from childhood.
Measures
All participants completed a second informed consent and initial well-being measures via SurveyMonkey (www.SurveyMonkey.com). Figure 2 depicts the measures participants, RMs and perceivers completed and the timeline for their administration. Please see Supplementary Data S1 for references and details on the measures used.
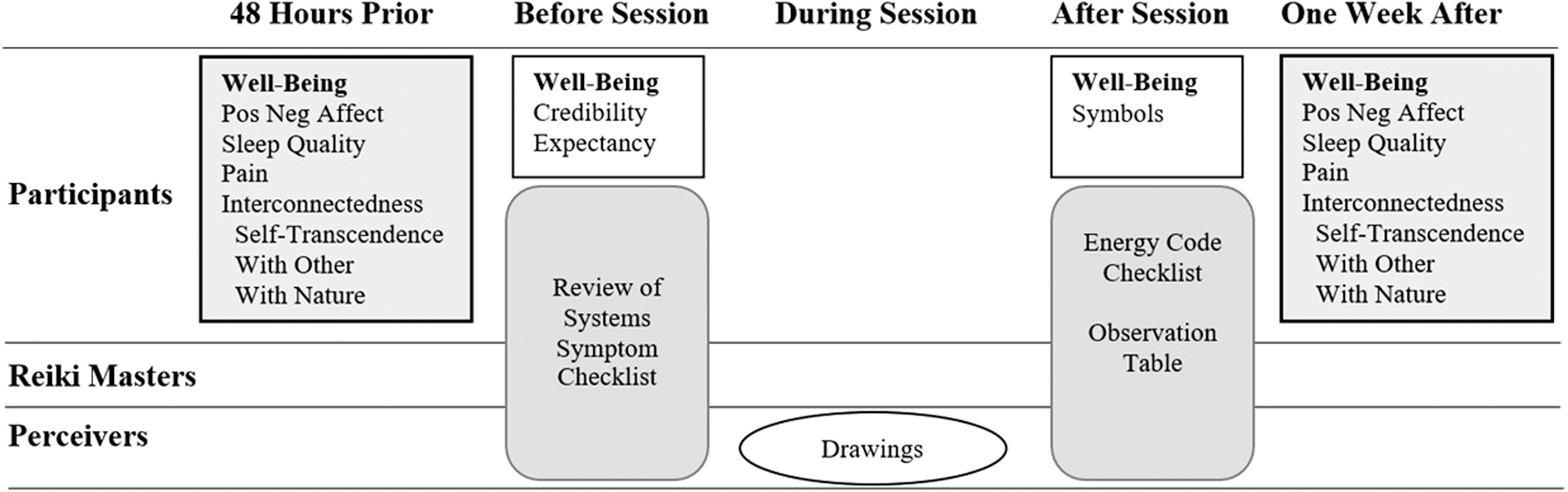
Measure schedule.
The participant well-being measures were the Arizona Integrative Outcomes Scale 19 (AIOS; primary outcome), Positive and Negative Affective Scale, Sleep Quality Scale, Numeric Pain Rating Scale, Cloninger Transcendence Subscale, Interconnectedness with Self (INS), and Interconnectedness with Other (IOS). The Credibility and Expectancy Scale assessed beliefs and expectations regarding Reiki efficacy. The Noetic Experience Belief Scale evaluated paranormal beliefs and experiences. Immediately after the session, staff sent participants an email inquiring about the meaningfulness of any symbolic information noted by the perceiver (e.g., a key, a flower, an animal, a blue door).
Participants also completed the investigator-designed Review of Systems Symptom Checklist (Symptoms), including 14 categories typically reviewed in a clinical setting (e.g., respiratory, cardiovascular, nervous), and Energy Code Checklist (Energy Codes), including 6 energy categories (e.g., energy attributes, symbols, participant receptivity, RM/participant rapport, other beings, and the healing process). The Energy Codes measure was based on the thematic codes generated from our pilot study 18 and feedback from RMs who we asked to review the codes.
Perceivers noted their observations during the session with colored pens on a paper with an outlined person's front and back with three ceiling-mounted cameras recording this process. The three video streams were time locked with a corresponding time stamp to capture common marks for intra- and inter-perceiver drawing analyses.
Reiki sessions
The 30-min Reiki sessions occurred at a Hilton Hotel Sonoma Wine Country conference room from July 26 to August 6, 2021. Four sessions were scheduled each day with 30 min between each for pre- and post-session measure completion and treatment space cleansing with Clean Sweep Spray (Energy Tools International, OR) and all study staff's intention to clear the room. Four RMs administered eight sessions and two RMs four (4 each day) according to their standard procedure.
Participants arrived and met the RM and perceivers. Participants sat in a reclining chair, RMs in a rolling chair, and perceivers (two per table) at six-foot conference tables arranged in a semi-circle around the room's edges. The distance between perceivers and the treatment was ∼10 feet, ensuring adequate visibility.
Analyses
Thirty-three participants were needed for 80% power to detect a 0.15 difference in the overall versus hypothesized mean using a standard deviation of 0.30 on Krippendorff's alpha interrater reliability score (Kalpha). Percentages, means, and standard deviations were calculated and described where appropriate. All relevant variables were assessed for normality using the Shapiro–Wilk test and examining a data histogram. Each analysis is briefly reviewed next, with details provided in Supplemental Data S1.
Qualitative correspondence
Authors (H.W., G.Y.) and an IONS staff member qualitatively judged the correspondence of the Observation Table (i.e., observation, meaning, overall) and Drawing data with the following scale:
Excellent correspondence with essentially no differing information. Good correspondence with relatively little differing information. Good correspondence with unambiguous unique matchable elements, but some differing information. Good correspondence with several matchable elements intermixed with some differing information. Mixture of matching and not matching elements, but with enough matching to indicate that the answers are similar. Some matching elements, but not sufficient to suggest results beyond chance expectation. Little correspondence No Correspondence
Drawing timeline analysis
Replaying the video recordings, staff recorded the number of new marks for each perceiver and 2-min windows centered on each initiation. Staff evaluated the presence of similar marks in these 2-min windows across perceivers.
Quantitative interrater reliability
Kalpha was calculated for the Symptoms and Energy Codes forms across the six perceivers and then pairwise for the perceiver, RM, and participant, with one value for (1) each item, (2) each session, (3) all codes per session, and (4) each code for all sessions. The planned Kalpha metric was deemed inappropriate for the collected data despite its appropriateness for this study design (see Supplementary Data S1 for a discussion of this), and so percent agreement was also calculated with values representing the following inter-rater agreement among perceivers: 100% = 6/6; 83% = 5/6; 67% = 4/6; 50% = 3/3.
Normally distributed data were analyzed with a one-sample t-test using the alternative hypothesis that mu is greater than or equal to 0.80 or 80%. Non-normally distributed data were analyzed with the one-sample Wilcoxon signed-rank test with the alternative hypothesis that the true location is greater than or equal to 0.80 or 80%.
Well-being changes and predictors
Non-normal variables were transformed, if necessary. If normalization was impossible, the Friedman test (non-parametric repeated-measures analysis of variance [ANOVA]) was used. The analysis included four AIOS time-points (baseline, pre-session, post-session, 1-week follow-up) with Tukey's honestly significant difference for post hoc pairwise comparisons. The other well-being measures used two time-points, baseline to 1-week follow-up. We calculated Hedges's g effect size and 95% confidence intervals using an effect size calculator (https://effect-size-calculator.herokuapp.com).
ANOVA evaluated potential predictors with AIOS change scores as the dependent variable, with each potential predictor as the independent variable (RM, demographics, personality, paranormal belief and experiences, credibility, and expectancy). The False Discovery Rate multiple comparison correction 20 to establish significance for these 16 total models was p ≤ 0.0051. In addition, a linear mixed-effects model evaluated the relationship between AIOS score and time (before/after the session), practitioner, credibility, expectancy, acute injury, memory, CESD, and GAD. The model was fit with random intercepts for each individual using the R package nlme. 21
Hypotheses
The hypotheses for the five research questions are as follows:
Question 1 (perceiver's corroboration)—That the average correspondence scores for the Observation Table (observation, meaning, overall) and Drawings would be ≥3 averaged over all the sessions with no significant difference by RMs; that the perceiver's Energy Codes average Kalpha would be ≥0.80 by session and overall; and that similar elements would be noted within 2 min of each other for ≥2 perceivers in a majority of the sessions.
Question 2 (pairwise perceiver, RM, participant corroboration)—That the Symptoms and Energy Codes' Kalphas would be ≥0.80 for each code and by session and in a pairwise fashion using a one-sample t-test assuming a normal distribution; and that the Observation Tables parameters average pairwise correspondence scores would be ≥3.
Question 3 (perceiver/participant symbolic information corroboration)—That ≥3 perceivers would observe similar symbols; that participants would report ≥25% of those symbols as meaningful; and that ≥25% of the participants would note a similar meaning to the perceiver's ascribed meaning.
Question 4 (perceiver assessment of participant health)—That the perceiver's and participant's Symptoms average Kalpha would be ≥0.80 by session and overall.
Question 5 (participant well-being improvement and predictors)—That the AIOS score would significantly improve over the four-time points, and the personality trait of openness and health categories would be significant predictors.
Results
Participants
Table 1 depicts participant characteristics with number, percentage, mean, and standard deviation. Column 4 is the statistics results for each characteristic as a predictor.
Participant Characteristics (N = 40)
The AIOS change score was calculated immediately before to after the session. None of these predictors was significant with an FDR multiple comparison correction.
AIOSΔ—the change in the AIOS.
Participants could check more than one ethnicity.
Resources were measured with the single-item question, “Please rate your access to material goods, money, friendship, networks, healthcare, leisure time, or educational opportunities,” with the answer options of a slider anchored by 0—I have no access to 100—I have unlimited access.
AIOS, Arizona Integrative Outcomes Scale; CESD, Center for Epidemiological Studies Depression Scale-5; FDR, false discovery rate; GAD, Generalized Anxiety Disorder-7; Inoue, Inoue Computerized Test Battery; N, participant number endorsing that characteristic; SD, standard deviation.
Question 1. perceiver corroboration
Observation table
The average correspondence scores were 4.6 ± 0.7 for the observation text, 3.5 ± 1.5 for the meaning text, and 4.4 ± 0.7 for the overall score. The observation (χ 2 = 16.4, p = 0.006) and meaning text [F(5, 34) = 8.90, p > 0.00005] showed significant differences by RM, but the overall score did not (χ 2 = 8.6, p = 0.13).
Energy codes
The most commonly endorsed energy codes are listed here, followed by the number of endorsements by the perceivers (total possible is 6 × 40 = 240):
Participant is receptive (224).
Energy moving from the RM to the participant (220).
Energy is blocked (218).
Rapport between the RM and participant is good (212).
Healing occurred (211).
Quality of the energy in the room was safe (205).
Energy was moving out of the participant (discharge, clearing, releasing) (198).
Emotional and psychological healing occurred (194).
Quality of the energy being transmitted by the RM was safe, calm, and relaxed (193).
Participant's systems are calmed or soothed (193).
The average agreement was 70%, 56%, and 74% for code, session, and overall, respectively, and the Kalpha was −0.01, 019, and 0.04 for code, session, and overall, respectively.
Drawings
The content's average correspondence score was 4.7 ± 0.6, with no difference by RM (χ 2 = 5.4, p = 0.37).
In total, 34 sessions were video recorded, 2 with only 4 perceivers. Camera power issues prevented recording for six sessions. Thirty-four sessions (100% of videotaped sessions) had at least 1 instance where ≥2 perceivers drew a similar element within 2 min of each other. Perceivers drew 94 instances of similar elements, 20 with 3 perceivers, 1 with 4 perceivers, and none with >4 perceivers.
Thirty instances were for color, 41 were for part of the body, and 23 were for both. The average number of similar elements in each session was 2.8 ± 1.5 (range 1–7). Perceives noted most similar elements (66 instances or 70% of the total number of instances) in the first 10 min of the session (see Supplementary Data S1 for similar element timings).
Question 2. Pairwise perceiver, RM, participant corroboration
Symptoms and energy codes
Table 2 presents the means and standard deviations of the percent agreement and Kalphas for the Symptoms and Energy Codes forms. The Energy Codes percent agreement and Kalpha were not statistically significant (all p's = 1), despite the overall percent agreement being higher than 80%. Most percent agreement and Kalpha values for the Symptoms form were significant.
Kalpha Means, Standard Deviation, and Range for the Review of Systems Symptom Checklist (Symptoms) and Energy Code Checklist (Energy Codes) Pairwise Comparisons for Perceivers and Reiki Masters, Perceivers and Participants, and Reiki Masters and Participants
0.0001 ** <0.00005 p-values for evaluating values greater or equal to 80% or 0.80.
RM, Reiki Master; SD, Standard Deviation.
Observation table
There were no significant correspondence scores from pairwise comparisons across perceivers, RMs, and participants (range 0–1.2). Perceivers generated significantly more text in their Observation Tables than participants and RMs [F(2, 133) = 10.92, p < 0.00005; Perceivers 720 ± 641 characters, participants 238 ± 343, RMs 120 ± 52]. Correspondence values were likely low primarily because of text volume.
Question 3. Perceiver/participant symbolic information corroboration
An average of 6.5 ± 2.7 (range 1–13) symbols were noted each session. Perceivers rarely noted the same symbol (number of perceivers noting the same symbol −0.83 ± 1.11, range 0–3). More perceivers reported similar symbol categories, for example, animal, geometry, face (1.05 ± 1.08, range 0–3). Thirty-five participants (88%) felt that at least one observed symbol was meaningful to them.
Perceivers reported 243 symbols overall, 110 of which were meaningful to the participants (45.3%). Forty-seven percent (47% ± 35%, range 0–100%) of the symbols were meaningful to the participant if perceivers reported more than one symbol for the session. Only in one session did the meaning the perceiver gave the symbol match what the participant said.
Questions 4. Perceiver assessment of participant health
Table 3 displays the Symptoms form percent agreement and Kalpha. The overall percent agreement was significant, but the others were not (p's 0.85 to 1.0).
Perceiver Correspondence for the Review of Systems Symptom Checklist
<0.00005 p-values for evaluating values greater or equal to 80% or 0.80.
Question 5. Participant well-being and predictors
There were no adverse events or unintended effects from the sessions and no missing data for the primary and secondary outcomes. The AIOS well-being primary outcome significantly increased over the four time-points [F(3, 159) = 12.3, p < 0.00005; baseline −55.7 ± 18.8, before −58.9 ± 18.1, after −73.2 ± 16.2, 1-week later −64.3 ± 20.3]. Post hoc analyses revealed significant differences from baseline to post-session (t = 4.25 p < 0.00005) and pre-session to post-session (t = 3.48 p = 0.004). The effect size is 0.61, 95% confidence interval [0.39–0.59] (Fig. 3).
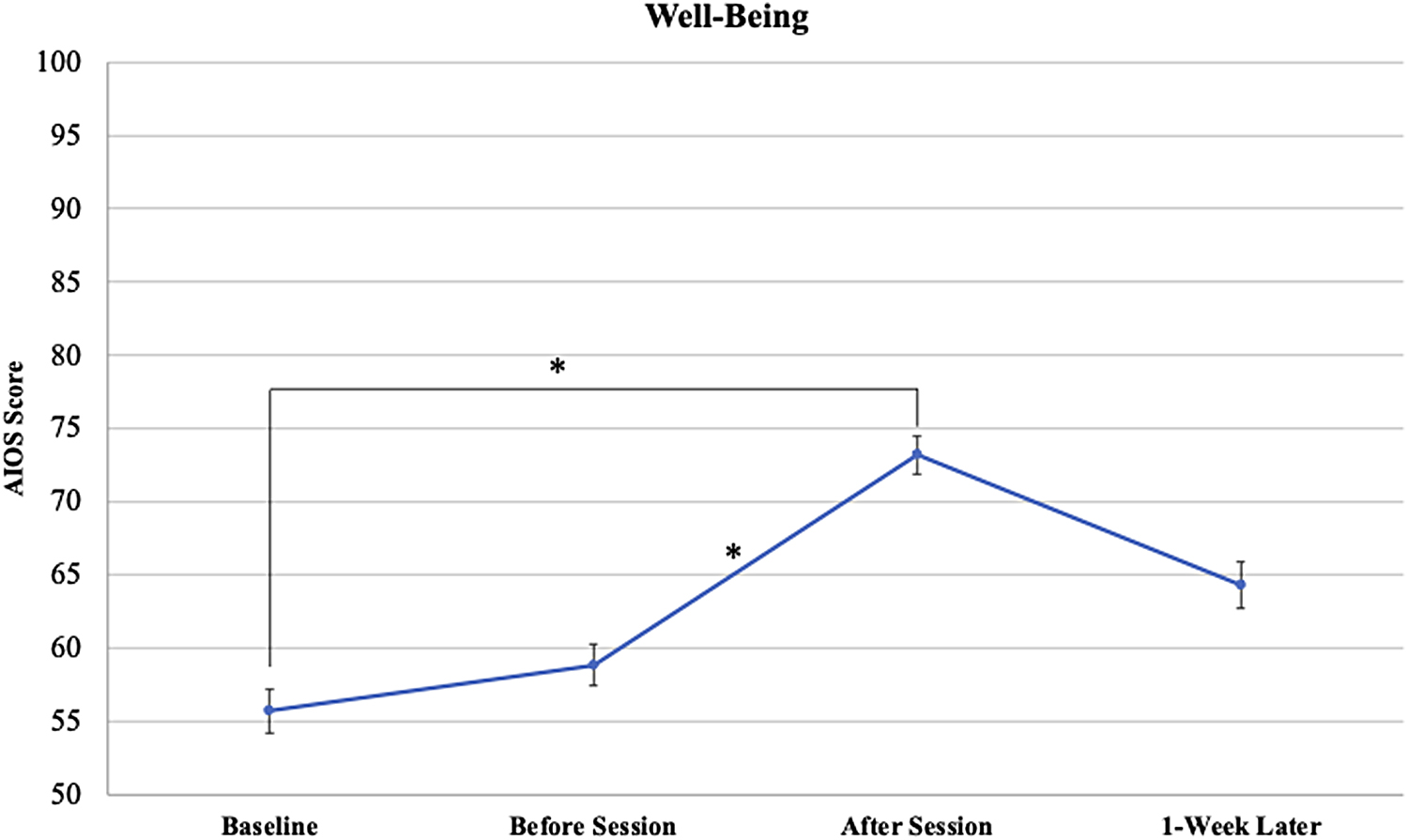
Well-being changes over time. Well-being was measured using the AIOS. Scores range from 0 to 100, with 0 anchored by “Worst I've ever been” to 100 anchored by “Best I've ever been.” Each point represents average scores with standard error bars. *Denotes significant pairwise comparisons. AIOS, Arizona Integrative Outcomes Scale.
Table 4 presents the means, standard deviations, and statistical tests evaluating changes in the secondary well-being outcomes. Negative affect demonstrated significant improvement (decrease), which persisted after the multiple comparison correction.
Secondary Well-Being Outcomes
FDR, p ≤ 0.0051 cutoff for significance; Log, log transformation used to achieve normality; Pain, The Numeric Pain Rating Scale; PANAS-X, Positive and negative affective well-being; Self-Transcendence, Cloninger Transcendence subscale; Sleep Quality, Sleep Quality Scale; Square, square transformation used to achieve normality. Z, Wilcoxon signed-rank test because the pain score is not normally distributed despite various transformations.
Predictors for well-being change
No potential predictors were significant for predicting AIOS change after correction for multiple comparisons when examined in separate models (see column 4, Table 1 for statistics). Similarly, there were no significant predictors in the combined predictor model, including RM, credibility, expectancy, or health category (see Supplementary Data S1 for statistical output).
Discussion
In summary, this exploratory study evaluated qualitative and quantitative data collected before, during, and after 30-min Reiki sessions in 40 participants with various health symptoms. Enthusiasm for the study was high in that numerous RMs and volunteers wanted to participate. Overall time-points, participants' well-being statistically improved.
Pairwise tests demonstrated that baseline to post-session and pre-session to post-session changes drove statistical significance. Thus, even though 1-week post-session well-being averages were higher than baseline and pre-session averages, they were not statistically different.
The perceivers generally perceived similar information as noted in the drawings and text and had a high overall Energy Codes agreement (74%). Perceivers' perceptions about the participants' symptoms before the session were highly corroborated and matched participants' self-reports. Further, participants felt that symbolic information was meaningful, although perceiver corroboration on symbolic information was low, and their ascribed meaning differed from the participants. Table 5 broadly summarizes the research questions and results.
Research Questions and General Summary of Results
Participants
Participants were generally middle-aged to older, college-educated, and mostly women of European descent. Many participants had overlapping health symptoms as assessed with our four categories (acute injury, memory loss, anxiety, and depression), resulting in them being included as separate predictors for well-being improvements to reflect these co-morbidities better. These four symptom categories ensured a diverse participant pool with varying health conditions, not limited to only physical conditions but also mental and emotional conditions, so that outcome differences by the condition could be assessed.
Credibility and expectancy also did not predict the well-being outcome. Namely, whether participants believed in Reiki efficacy or felt it would help them did not predict their well-being scores. This potentially supports the idea that although placebo effects often influence mind-body and energy medicine, 22 placebo may not have influenced well-being scores in this study. Also, for consideration is the potential for participants to change their behavior because of observation, such as changing their self-report answers (i.e., Hawthorne effect).
Reiki Masters
The RMs were receptive to the research setting and unfamiliar study requirements (e.g., having six perceivers observing them). One unexpected occurrence was that the perceivers expressed discomfort with one RM's energy and believed that the RM had a malevolent spirit attachment blocking their perceptive abilities. Although it is impossible to verify this belief, many cultures and spiritual traditions worldwide describe spirit attachment phenomena. 23
The study team decided to replace the RM for their second day of sessions to eliminate any potential impairment of the perceivers' abilities, because they were essential to the study's primary purpose. Finding a replacement proceeded efficiently, because numerous well-qualified RMs applied.
Perceivers
Numerous perceivers applied. Selected perceivers had to be able to perceive externally (i.e., endorse seeing energy, its color, texture, and movement). This criterion assumes that this “energy” exists and that skilled people can observe it. Although all the perceivers endorsed seeing energy externally, the data revealed other perceptions, including mental, emotional, spiritual, and physical information from the participant's past and present, in addition to session-specific observations. This study's a priori research questions focused on perceiver corroboration rather than the content. Future qualitative analysis of this rich dataset will explore the content.
The extensive volume of information that the perceivers received and conveyed was problematic, because it was challenging to distinguish the signal from the noise. Future studies would benefit from clarifying what the perceivers observe in a stepwise fashion. For example, rather than asking the perceivers to record all they observed during the 30 min, they could begin with someone who was not receiving a session, sequentially asking about the participant's emotional, mental, physical, and each body system.
Also, many perceiver training programs use the chakra system model for the body's energy anatomy. 24 A percentage open or other quantitative measures for each chakra's state could be incorporated. Perceivers could complete a detailed static read of the participant before the session begins. Session instructions would focus only on the energy movement, color, texture, etc., through their external sight perception, ignoring other information. These methods should reduce noise and allow easier corroboration analyses.
Perceivers agreed during the vetting process that they could contain their energy, not interfering with the session or their fellow perceivers. Future studies could consider perceivers observing from separate rooms through closed caption video cameras as an extra measure. Perceivers discretely observing would also support the RMs and participants who initially expressed minor nervousness at being observed despite knowing that observation would occur.
The perceivers committed not to discuss the sessions, and there is no reason to believe they did. However, they ate meals together and developed a sense of community and positive regard toward each other. This congeniality raises the question of whether their outside interactions interfered with their ability to perceive independently from each other.
The extended perception's mechanism is unknown; thus, the proximity between perceivers may or may not influence the results. A brief, informal data review shows that perceivers sitting at the same table did not always report similar information. Future study designs where perceivers are physically isolated can elucidate whether perceiver proximity is essential.
Study procedures
Having the entire study in the same place with all study staff present supported excellent data collection, with no form missing data, a rarity in clinical studies. The missing video recordings because of the power issue could be prevented by using electronic recording devices, such as tablets with drawing capabilities or text programs, which could timestamp marks made or text entered. If the perceivers are in separate rooms, they could audio record their impressions that could later be transcribed with timestamps.
Perceiver corroboration
The qualitative judging, symptoms, timeline analyses, and high percent agreement for most of the calculated values support our hypotheses for question 1. Some might argue that the 80-threshold level is too high for such a complex information source and that cutoff scores for interrater reliability measures are arbitrary.
For example, Landis suggests a very different strength of agreement criteria for categorical data (<0 Poor, 0–20 Slight, 21–40 Fair, 41–60 Moderate, 61–80 Substantial, 81–100 Almost Perfect). 25 In this case, the a priori hypotheses thresholds of 80 would reflect an almost perfect agreement. The lowest percent agreement for our analyses was 56, representing moderate agreement with Landis' criteria.
Corroboration between each perceiver, RM, and participant
The agreement was high for the Symptoms form (range 67% to 91%) and moderate to almost perfect for the Energy Codes (range 60% to 84%) using Landis criteria. The perceivers' observations of the participants' health before the session highly agreed with the participants' self-reports. Thus, not only did the perceivers have a high agreement with each other overall, but they also had high agreement with the participants. These results lend support to the idea that perceivers can detect information about the people they view.
Symbolic information
Perceivers often mention symbolic information during sessions. Thus, we explored if perceivers observed similar symbols and found that they did not. Nevertheless, the symbols observed were meaningful to the participant. Perhaps the participants wanted to please the study staff by reporting positive meaning to the symbols.
However, some were unique, such as the lightning or lucky charms. The angel or guide symbol was ubiquitous in almost all sessions. Spiritual helper anecdotes are as old as humanity's written record. 11 Although we cannot confirm or deny the presence of spiritual beings supporting the Reiki session, perceivers observing them was meaningful to the participants and imparted a sense of comfort and healing.
Well-being improvement
The participants benefited from the sessions, as evidenced by their well-being score and negative mood improvement, reflecting other Reiki studies' positive outcomes. 3 The participants were diverse in age and ethnicity, supporting the generalizability of this outcome. Notably, many participants were visibly affected by the sessions. Most felt not only very relaxed but also “out of it,” such that they had to sit quietly for 10–15 min before they could resume their normal activities.
The non-significant predictor results potentially support the premise that Reiki energy affects the receiver in the ways most needed, regardless of any specific pathology, regardless of a recipient's health condition, beliefs, or expectations about Reiki, other paranormal phenomena, or their characteristics. This aligns with traditional teachings about Reiki and that it may be universally applied to any condition for health promotion.
Limitations
Several limitations should be considered when reviewing the study's results and planning future studies. First and foremost, this is an exploratory study. No analyses were meant to be definitive. The study was uncontrolled; thus, we cannot rule out the possibility that data generated with mock perceivers would yield similar results. Similarly, we cannot confirm whether well-being improvements resulted from placebo, Hawthorne effects, or natural progression.
Participant health categories were collected using validated self-report screening tools and were not verified. The study authors conducted the qualitative judging, introducing possible bias because the research team was familiar with the study's design and hypotheses.
The Kalpha interrater reliability measure was appropriate for the study design and data type; however, our data distribution did not allow for the proper implementation of this statistical metric. We could not have known this until we collected the data. Percent agreement is a valid and commonly used measure of interrater reliability, 26 and we could have chosen percent agreement a priori instead. Thus, although many Kalpha values were not significant, we invite the reader to reflect on the broader corroboration picture from the qualitative judging and percent agreement in interpreting the findings and planning for future studies.
Future applications
Extended perception is especially intriguing, as researchers could pair it with relevant clinical outcomes and verify it with biological testing. For example, participants with specific ailments diagnosed with gold-standard testing, such as computerized tomography, X-ray, or bloodwork, would be vital to assessing the validity of extended perception readings.
The capacity to perceive information about the body in this way, sometimes called medical intuition, is likely the most practical and easily verifiable application of extended perception and should be strongly considered to move the field of extended perception forward. A few medical intuition studies have been conducted,14–17,27 but more are needed. Medical intuitives can also provide insight into etiology, diagnoses, and treatment plans in collaboration with medical professionals without usurping their authority.28,29
Conclusions
Participants reported well-being measure improvements from a 30-min Reiki session. Multiple analyses showed that perceivers observe similar information during Reiki sessions. Further, there was correspondence between the perceivers' observations of the participant's health condition and their self-reported health. Future studies are needed to refine the methods developed here to continue the exploration of extended perception, its validity, and practical application in health care.
Footnotes
Acknowledgments
The authors would like to thank the Emerald Gate Charitable Trust and Jeffrey C. Walker for their generous support of this work. They would also like to thank the Institute of Noetic Sciences staff and members, Maria Wojakowski, Monica Summers, the Reiki Masters, Perceivers, and participants, for their support and contributions to the project.
Authors' Contributions
H.W.—Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing—original draft, and Writing—review and editing. P.S.—Data curation, Formal Analysis, Writing—original draft, and Writing—review and editing. G.Y.—Conceptualization, Formal Analysis, Supervision, Writing—original draft, and Writing—review and editing.
Data Availability
The data for this project are publicly available on the Figshare Repository 10.6084/m9.figshare.17251811.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Emerald Gate Charitable Trust and Jeffrey C. Walker supported this work. The investigators shared the study design, measures, and procedures, in regular meetings with the funders. The funders gave feedback, and it was incorporated if applicable and aligned with the project's overall goal. The investigators were not required to incorporate feedback to receive funding and freely rejected any funder ideas not aligned with the project. Nor did the funders have any vested interest in the study outcomes, potential financial gain from the study results, or financial connection to Reiki, energy medicine, or extended perception.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.