
Abstract
Cross-border disease surveillance and response is critical for addressing the increasing burden of infectious disease outbreaks and heavy metal poisoning in West Africa, particularly between Niger and Nigeria. This study assesses the collaborative efforts of Niger and Nigeria in strengthening cross-border disease surveillance, addressing health security threats, and improving response strategies for heavy metal poisoning and infectious diseases. The West African Health Organization, in collaboration with regional partners, convened a cross-border meeting in June 2024, to bring together health experts and key stakeholders from both countries and from regional organizations. The meeting included technical sessions, working group meetings, and the development of a joint action plan. The discussions highlighted major challenges, including gaps in surveillance, delays in data sharing, and resource limitations. Key recommendations from the meeting included harmonizing surveillance tools, strengthening laboratory capacity, enhancing risk communication, and securing funding for sustainable cross-border health initiatives. Strengthened collaboration between Niger and Nigeria is essential to mitigate the public health risks associated with cross-border disease transmission. Policy actions, resource mobilization, and sustained engagement with regional and international partners are necessary for a robust and effective cross-border disease surveillance system.
Background
The cross-border spread of infectious diseases in West Africa is a significant public health challenge, exacerbated by the region’s high mobility, porous borders, and weak health systems.1,2 West Africa is home to various interconnected communities, economies, and ecosystems that transcend national boundaries, making disease control complex. Infectious diseases such as Ebola, Lassa fever, mpox, measles, and COVID-19 often spread rapidly across national borders—particularly in regions with dense populations, nomadic lifestyles, and shared ecological conditions 3 —necessitating cross-border collaboration for effective disease surveillance and response. 4 Cross-border surveillance is crucial in the global fight against infectious diseases that can spread quickly, especially in regions with porous borders and significant cross-border movement. This surveillance is essential for early detection, timely response, and effective management of transboundary health threats.
In August 2023, Nigeria underwent its second Joint External Evaluation (JEE) of International Health Regulations (IHR) core capacities. 5 The evaluation revealed a significant improvement, with Nigeria’s overall score increasing from 39% in 2017 to 54% in 2023. Notably, Nigeria’s 2023 JEE scores showed strong point of entry (POE) capacity (4), better surveillance (3 to 4), moderate laboratory systems (2 to 3), and well-developed emergency response (3 to 4). However, the identified gaps in specimen transport, workforce surge capacity, and public health–security collaboration pose substantial challenges for outbreak containment and response. Strengthening capacities at subnational levels remains a priority to ensure a more robust and decentralized response mechanism.
While the last JEE assessment in Niger was in 2018, historical assessments and regional analyses suggest that Niger faces similar challenges in health security. Niger’s 2018 JEE scores indicated weak POE capacity (1), limited surveillance (2 to 3), poor emergency response (1 to 2), and moderate laboratory capabilities (2 to 4). 6 The country struggled with border health security, specimen transport, and emergency activation, making it vulnerable to undetected disease outbreaks. The country has been working toward improving its health system capacities, but gaps persist, especially in areas such as surveillance, laboratory capacity, and emergency response.
These disparities contribute to cross-border disease spread and porous border challenges between the 2 countries. Niger’s weaker POE capacity and limited disease surveillance make it more vulnerable to undetected outbreaks, which can easily spill into Nigeria through informal crossings and trade routes. Nigeria’s relatively stronger response mechanisms may help detect outbreaks faster, but without synchronized cross-border surveillance and real-time data sharing, undetected cases from Niger can undermine Nigeria’s containment efforts. The long shared border, with high human and livestock movement, informal trade, and security constraints, further complicates effective disease control, making joint cross-border surveillance, early warning systems, and harmonized POE interventions essential for reducing the risk of regional outbreaks. The high mobility of populations and the common social and economic ties between communities on either side of the border necessitate a coordinated approach to disease surveillance and response.3,4
The 2 border countries have faced multiple outbreaks, including cholera, meningitis, and, more recently, COVID-19. The differences between the countries’ health system capacities, particularly their surveillance systems, laboratory capacities, and response mechanisms, can hinder timely data sharing and coordinated responses to public health threats. These gaps underscore the need for harmonized strategies and collaborative efforts to strengthen cross-border health. The collaborative efforts between Niger and Nigeria aim to strengthen surveillance, enhance information sharing, and coordinate public health responses to contain and mitigate the spread of diseases.
Heavy Metal Poisoning and its Historical Impact in West Africa
Heavy metal poisoning has had significant historical and ongoing impacts in West Africa, primarily due to artisanal gold mining, industrial activities, and the use of lead products. 7 For example, artisanal gold mining, a longstanding practice in the region, uses mercury to extract gold, releasing toxic vapors into the environment. 8 Additionally, the widespread use of leaded gasoline until the early 2000s and poor industrial waste management have contributed to soil, water, and air contamination. Major incidents, such as the 2008 lead poisoning outbreak in Dakar, Senegal, where informal battery recycling exposed residents to dangerous lead levels, highlight the risks of unregulated practices. Similarly, oil exploration in Nigeria’s Niger Delta and gold mining in Burkina Faso and Ghana have led to widespread mercury and lead contamination, affecting ecosystems and communities.
In Nigeria, extensive oil exploration and artisanal refining have resulted in substantial heavy metal pollution. Studies have reported lead concentrations in water sources reaching up to 39 ± 33 mg/L, significantly exceeding the World Health Organization (WHO) permissible limit of 0.01 mg/L. 9 Similarly, cadmium levels have been found at 2.4 ± 3.1 mg/L, surpassing the WHO guideline of 0.003 mg/L. 10 These elevated concentrations pose serious health risks to local communities reliant on these water sources.
In Ghana, heavy metal contamination has been linked to both industrial discharge and mining activities. For instance, water samples from the Iture estuary exhibited lead levels of 0.075 mg/L and cadmium levels of 0.041 mg/L, both exceeding WHO standards. 10 Such contamination is attributed to waste carried by rivers flowing through rapidly industrializing regions.
The health impacts of heavy metal poisoning are severe, especially for children and pregnant women. Lead poisoning causes neurological damage, developmental delays, anemia, and kidney failure, while mercury exposure leads to tremors, memory loss, and cognitive impairments. Cadmium and arsenic, also prevalent in contaminated areas, can cause kidney damage, cancer, and cardiovascular diseases. These health issues strain already fragile healthcare systems and reduce workforce productivity, further hindering economic development.
Socioeconomic consequences are profound. Contaminated soil and water reduce agricultural productivity, threatening food security and livelihoods. Children exposed to heavy metals suffer irreversible cognitive damage, limiting their educational and future opportunities. The economic burden of treating poisoning and managing environmental cleanup further exacerbates poverty in affected communities.
Efforts to address heavy metal poisoning include regulatory measures, such as Nigeria’s 2002 ban on leaded gasoline, and international initiatives like the Minamata Convention on Mercury. 11 which aims to reduce mercury use globally. Community education programs and cleanup initiatives, such as those in Thiaroye Sur Mer, have also been implemented. However, many challenges remain, including weak enforcement of regulations, reliance on artisanal mining for livelihoods, and limited resources for cleanup and healthcare.
Heavy Metal and Infectious Disease Context in Nigeria and Niger
Heavy Metal Poisoning in Northern Nigeria and Southern Niger
Both Nigeria and Niger face challenges related to environmental pollution, including heavy metal contamination, primarily due to mining activities and artisanal gold mining.
The collaboration between Niger and Nigeria is crucial to contain this crisis, as contaminated water sources and pollutants cross borders easily, affecting both human health and agricultural productivity.
Infectious Disease Outbreaks and Response
Both countries have experienced significant outbreaks of infectious diseases, particularly diphtheria, Lassa fever, and meningitis. Table 1 shows the number of cases and deaths from infectious diseases from March 2023 to March 2024 for both countries.
Infectious Disease Cases and Deaths in Both Countries, March 2023 to March 2024
Abbreviations: CFR, case fatality rate; NA, not applicable.
Both countries face the dual challenge of addressing heavy metal pollution from mining activities and managing endemic infectious diseases, with the cross-border movement of miners, artisans, 17 and other people further complicating disease control efforts.
Existing Framework for Cross-Border Public Health Surveillance and Information Sharing
Niger and Nigeria have established formal frameworks for cross-border public health surveillance and information sharing. These frameworks through the existing agreements of the Abuja Declaration of 2010 18 and a draft memorandum of understanding facilitate the timely exchange of public health information, particularly in response to infectious diseases and emergencies, while adhering to the principles of the WHO Regional Office for Africa’s Integrated Disease Surveillance and Response (IDSR) in the Africa Region, 19 the Economic Community of West African States (ECOWAS) standard operating procedures for information sharing before, during, and after public health emergencies, and the ECOWAS interinstitutional communication and coordination strategy for coordinated action during public health emergencies. 20 These frameworks facilitate the systematic collection, analysis, and dissemination of health data to inform public health decisions They are tailored to include cross-border surveillance strategies, such as joint outbreak investigations and synchronized data collection and sharing efforts across West African Member States.
In cases of suspected cross-border disease outbreaks, joint teams from Niger and Nigeria, often comprising representatives from national health ministries, WHO, the West African Health Organization (WAHO), and other international partners, conduct investigations.21,22 Effective cross-border surveillance relies heavily on timely information sharing between countries. Niger and Nigeria have established bilateral communication channels, including regular meetings, data exchange platforms, and emergency hotlines to share real-time information about outbreaks. This approach allows for synchronized responses to public health threats.
Representatives from Niger and Nigeria met June 11 to 13, 2024, to address shared health challenges and cross-border needs. This article describes the outcomes of these efforts and showcases how the collaboration has enhanced information sharing and coordinated responses to public health emergencies.
Cross-Border Collaboration Framework
The cross-border collaboration framework between Niger and Nigeria (Figure) is designed to enhance public health security through coordinated efforts in surveillance, information sharing, and emergency response. It consists of 4 key components:
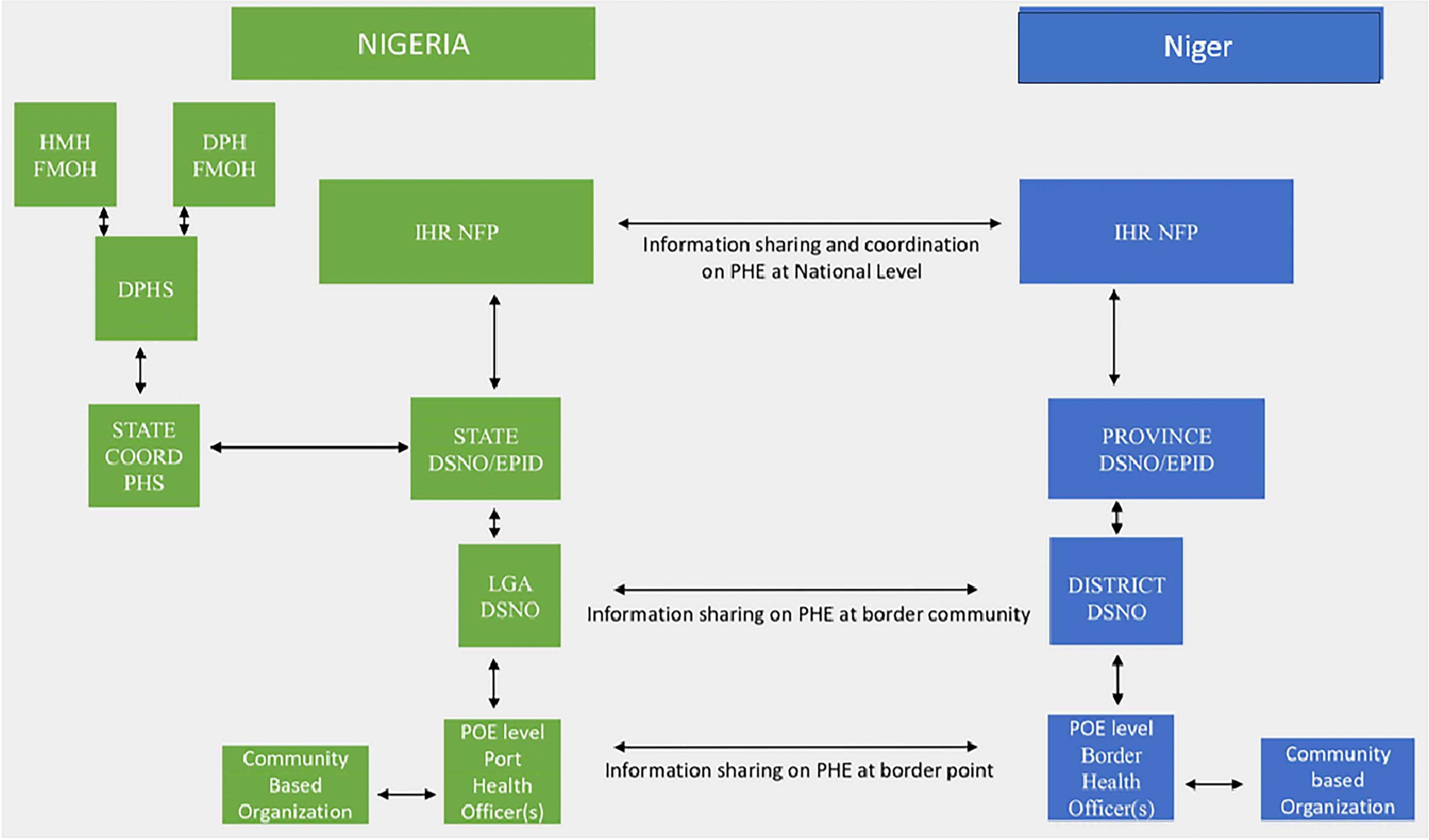
Cross-border collaboration and communication framework between Niger and Nigeria for public health events. Abbreviations: DPH, Department of Public Health; DPHS, Department of Port Health Services; DSNO, disease notification officer; EPID, epidemiologist; FMOH, Federal Ministry of Health; HMH, Honourable Minister of Health; IHRNFP, International Health Regulations Focal Person; POE, point of entry; State COORD PHS, state coordinator port health services.
This framework underscores the importance of close collaboration between Niger and Nigeria, promoting a unified response to cross-border health threats and contributing to the regional effort to strengthen public health systems.
Cross-Border Meeting Between Niger and Nigeria
WAHO organized a cross-border meeting leveraging the existing framework on cross-border surveillance and information sharing between Niger and Nigeria from June 11 to 13, 2024, in Nasarawa, Nigeria. The meeting aimed to address the need for a coordinated approach to disease surveillance and response, emphasizing collaboration in managing outbreaks of heavy metal poisoning, meningitis, diphtheria, and other diseases. The cross-border meeting included technical sessions on the epidemiological situation of both countries. Delegates from both countries discussed lessons learned from recent outbreaks and identified gaps in surveillance, diagnosis, and response. Four working groups were formed to develop a joint action plan focusing on the following areas:
Recommendations
The participants made the 5 key recommendations to address the identified challenges: enhance training and capacity building initiatives, strengthen joint surveillance and data sharing, build and strengthen community engagement and risk communication, establish joint cross-border surveillance committees, and secure funding for cross-border initiatives.
Challenges for Implementing Recommendations
While the framework for cross-border surveillance between Niger and Nigeria is robust, several challenges persist.
Both countries face significant logistical, human, and financial resource constraints that hinder their ability to maintain continuous accessible surveillance and rapid response capacities and convene regular cross-border meetings. Despite established communication channels, inconsistencies in data sharing and reporting formats between Niger and Nigeria sometimes lead to delays in response actions. Harmonizing data collection tools and reporting standards is still a work in progress.
26
The low availability of trained personnel and necessary laboratory facilities remains a critical challenge.
27
The border regions between Niger and Nigeria are often fraught with security challenges, including insurgent activities and armed conflicts. The frequent movement of nomadic populations and informal trade across borders complicates surveillance efforts, making tracking disease transmission and environmental contamination difficult.
Discussion and Next Steps
Cross-border disease surveillance and response remain critical in mitigating public health risks posed by heavy metal poisoning and infectious disease outbreaks between Niger and Nigeria. Despite existing frameworks, challenges persist, including inadequate data sharing, limited laboratory capacity, and resource constraints. A comparative analysis of similar initiatives across Africa provides valuable insights into best practices and strategies that can be adapted to strengthen cross-border surveillance between Niger and Nigeria.
The initiative between Niger and Nigeria shares similarities with programs such as the East African Community cross-border disease surveillance efforts, 28 which have successfully leveraged joint outbreak investigations, harmonized data collection, and rapid response mechanisms between Burundi, Kenya, Rwanda, South Sudan, Tanzania, and Uganda. For instance, the East African Community has developed a regional health surveillance system that enables real-time data sharing among member states. The use of digital health platforms and mobile-based reporting systems has facilitated quicker identification and response to disease outbreaks. Similarly, the collaboration between Guinea, Liberia, and Sierra Leone during the 2014-2016 Ebola outbreak demonstrated the importance of cross-border coordination, emphasizing the need for harmonized policies and integrated response mechanisms. Best practices from these initiatives highlight the need for political commitment, sustainable funding, and well-defined governance structures to support continuous information exchange and surveillance activities. The Niger–Nigeria initiative can adopt establishing a centralized, real-time data-sharing platform that can improve surveillance efficiency, reducing delays in reporting and response.
Another example is the Southern Africa Cross-Border Health Initiative. 29 Countries in Southern Africa (Botswana, Mozambique, South Africa, and Zimbabwe) have developed cross-border health policies to address HIV, tuberculosis, and malaria. The initiative includes a harmonized laboratory network, ensuring consistent diagnostic standards across countries, and cross-border health posts, offering routine testing and treatment for high-risk populations and joint risk communication strategies, targeting mobile populations such as migrant workers and traders. The Niger–Nigeria initiative can benefit from harmonized diagnostic protocols, particularly for laboratory testing of infectious diseases and heavy metal poisoning. Establishing joint health posts at border crossings would improve access to healthcare services for highly mobile populations.
Lessons learned from other African cross-border surveillance programs suggest that increasing investment in digital surveillance tools, strengthening workforce capacity through continuous training, and fostering multisectoral engagement can significantly enhance the effectiveness of these initiatives. By adapting these best practices, the Niger–Nigeria collaboration can further strengthen its public health security framework and serve as a model for other regions facing similar cross-border health threats.
Policy Next Steps
Governments in both countries should prioritize cross-border health initiatives by integrating surveillance activities into national health policies. Strengthening existing agreements and regulatory frameworks will ensure streamlined data sharing and emergency response coordination. Additionally, regional bodies such as ECOWAS and WAHO should play a key role in facilitating the implementation of standardized surveillance and response mechanisms.
To sustain this collaboration, work plan metrics were suggested for both countries (Table 2). Countries should invest in digital surveillance tools to enhance real-time data exchange and improve outbreak detection. Regular joint simulation exercises, workforce training, and capacity-building programs should be institutionalized to ensure preparedness for future public health threats. Furthermore, securing long-term funding from international donors and regional health organizations will be essential for maintaining these efforts.
Workplan With Metrics to Monitor Cross-Border Collaboration
Abbreviations: Africa CDC, Africa Centres for Disease Control and Prevention; NGO, nongovernmental organization; WAHO, West Africa Health Organization; WHO, World Health Organization.
Conclusion
The cross-border meeting between Niger and Nigeria in June 2024 marked a significant step toward improving public health security in the region. By addressing the dual threats of heavy metal poisoning and infectious disease outbreaks through enhanced collaboration, both countries can mitigate the impact of these health crises. Continued support from international partners, strong political will, and community engagement will be essential for building a resilient and effective cross-border disease surveillance and response system.
Footnotes
Acknowledgments
The authors would like to express their gratitude to all individuals and organizations who contributed to the successful completion of this study. We extend our deepest appreciation to WAHO for their support and collaboration. We also thank the Niger and Nigeria ministries of health, whose commitment to cross-border surveillance and collaboration made this project possible. A special acknowledgment goes to Dr. Rebecca Merrill of the US Centers for Disease Control and Prevention in Indonesia for her immense contribution to this work. Her expertise, guidance, and unwavering support were invaluable throughout the manuscript drafting process.