
Abstract
New York City has been the epicenter of multiple recent infectious disease outbreaks, including COVID-19 and mpox, due to its position as one of the largest international travel hubs in the United States. In response to the imperative need to transport patients to specialized biocontainment units during high-consequence infectious disease outbreaks, the Health and Human Services Region 2 Regional Emerging Special Pathogen Treatment Center at New York City Health + Hospitals/Bellevue and the NYC Department of Health and Mental Hygiene spearheaded a comprehensive patient transport system. Informed by real-world experiences, quarterly drills, and regional partner engagement, the updated Region 2 patient transport concept of operations (CONOPS) ensures safe and seamless patient transfers. This article elucidates key components of the patient transport CONOPS, the multifaceted partner engagement approach used to develop it, and the collaborative workshop that fine-tuned the plan. Organizational skills, partner engagement, and adaptability were all necessary for refining and operationalizing a robust patient transport CONOPS. The finalization of this plan speaks to the collaborative spirit and commitment of regional leaders to ensure the effective management of high-consequence infectious disease outbreaks and the safeguarding of public health within Region 2 and beyond.
Introduction
N
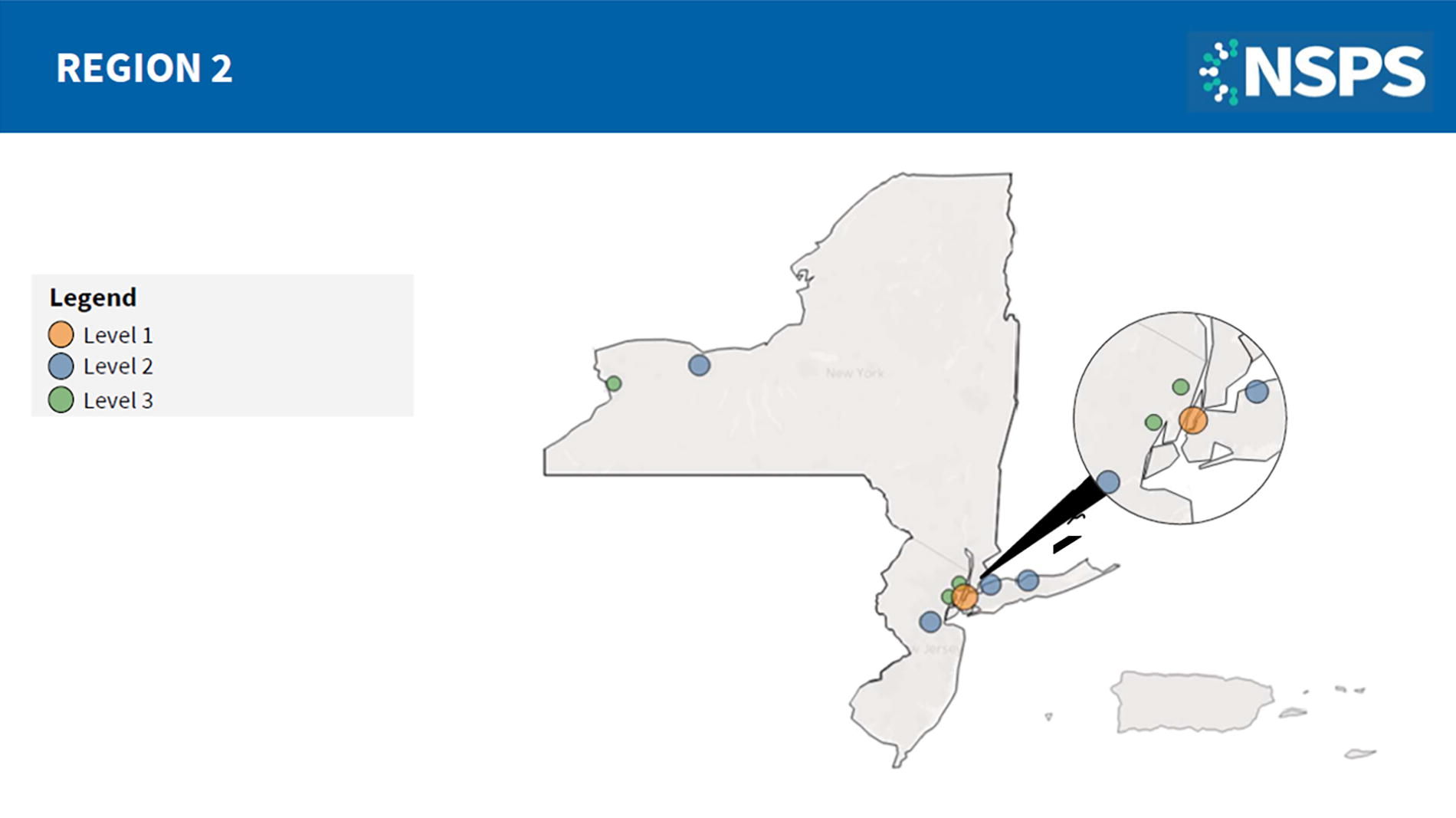
National Special Pathogens System of Care Region 2 facility map. NSPS Level 1 facilities (NYC H+H/Bellevue) can provide clinical care to HCID patients of all ages and acuity for the duration of their illness and also serve as regional resource hubs and leaders for HCID preparedness and response efforts. NSPS Level 2 facilities (Northwell Health Glen Cove, Stony Brook University Hospital, Robert Wood Johnson University Hospital, and University of Rochester Medical Center) can deliver specialized care to a cluster of HCID patients for the duration of their illness. NSPS Level 3 facilities (University Hospital, Hackensack University Medical Center, and Erie County Medical Center) are assessment centers that can stabilize a patient, conduct basic laboratory testing, and coordinate rapid patient transfer to a Level 1 or 2 facility within 12 to 36 hours. All other healthcare facilities are NSPS Level 4, which should be able to identify, isolate, inform, initiate stabilizing medical care, and arrange patient transport. This map was last updated in November 2024. Abbreviations: HCID, high-consequence infectious disease; NSPS, National Special Pathogens System; NYC H+H, New York City Health + Hospitals.
NYC H+H/Bellevue’s RESPTC runs quarterly drills to test its BCU’s processes and procedures. These drills evaluate existing capabilities and identify opportunities for continuous improvement. Following each drill, an after-action report is developed and an improvement plan is established to close those identified gaps. For example, a recent HCID patient transport drill conducted at NYC H+H/Bellevue identified a break in the communication chain. As a result, the communication gap has been resolved and those implemented changes are now outlined in hospital protocols. This refinement process allows for constant improvements in procedures to optimize patient care and staff safety in a real-world scenario.
The value of drilling and exercising protocols is evidenced through real-world events. Before NYC H+H/Bellevue saw its first Ebola patient in 2014, several persons under investigation had been transported and numerous patient transfer exercises had been conducted. Those real-world experiences and drilled scenarios allowed for further testing and refinement of the patient transport workflow. Through testing and improving its patient transfer protocols, NYC H+H/Bellevue was well prepared when an Ebola patient was brought to the hospital on October 23, 2014. 5 Because of the experience gained through prior exercises and experiences, those who participated in the transport were familiar with the choreography of the patient transport protocol, including which doors to open, how to secure the hallways, and how to disinfect the ambulance and affected areas of the facility following the transport, all while preventing further transmission of the pathogen.
Soon after the 2014-2016 Ebola outbreak, the first HHS Region 2 HCID patient transport system concept of operations (CONOPS) was created. The patient transport CONOPS is updated periodically to reflect changing regional capabilities. Because it had not been updated since before the COVID-19 pandemic, the CONOPS required updating due to staff turnover and the increasing risk of another HCID outbreak. This article describes key components of the revamped CONOPS, how regional partners were engaged in updating it, the well-attended workshop that tested the updates, and important considerations for developing a CONOPS.
Key Components of the Region 2 CONOPS
The NSPS System of Care is designed as a hub-and-spoke model, with the National Special Pathogens Treatment and Education Center (NETEC) as the congressionally appointed coordinating body. When a suspected special pathogen patient presents at a frontline facility, that facility will immediately notify their local and state departments of health (DOH) to determine if the patient should transfer to NYC H+H/Bellevue or a closer facility such as an NSPS Level 2 SPTC. If conditions for transport of a patient within HHS Region 2 to NYC H+H/Bellevue are met, the sending jurisdiction will notify the NYC Department of Health and Mental Hygiene (DOHMH) of a requested transfer to the Region 2 RESPTC at NYC H+H/Bellevue. NYC DOHMH coordinates with the local DOH, the
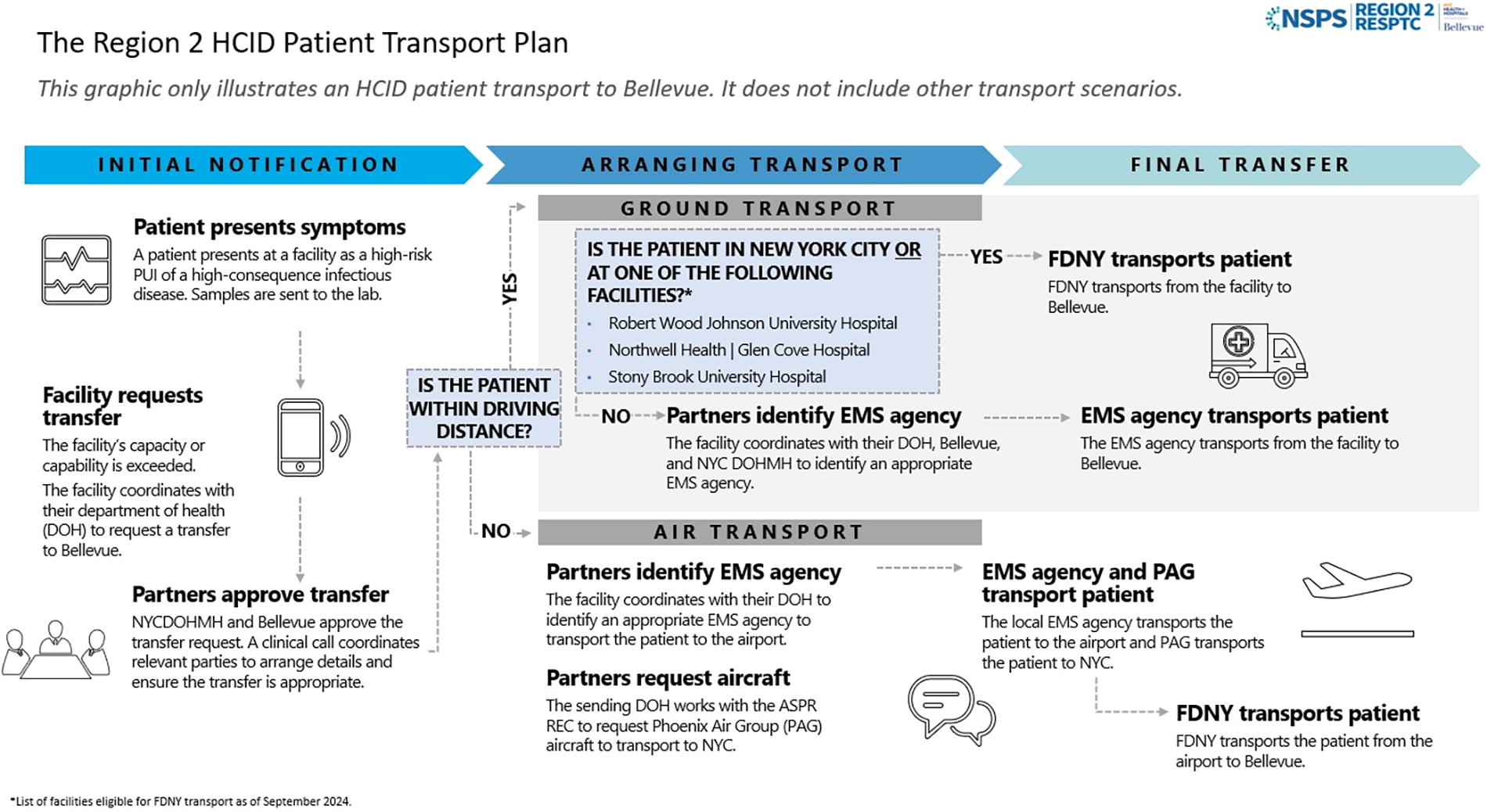
Region 2 HCID patient transport plan—the patient journey to NYC H+H/Bellevue. This diagram depicts the stages of patient transport and key decision points for the patient’s transfer to Bellevue. Abbreviations: DOH, Department of Health; EMS, emergency medical services; FDNY, Fire Department of New York City; NYC H+H, New York City Health + Hospitals; NYCDOHMH, New York City Department of Health and Mental Hygiene; PAG, Phoenix Air Group; PUI, person under investigation; REC, Regional Emergency Coordinator.
The CONOPS outlines scenarios for air and ground transport from each jurisdiction within HHS Region 2. For transports within New York City and directly outside the NYC metro area, FDNY serves as the primary ground transport agency. The level of EMS care provided (ie, basic life support, advanced life support, critical care transport 6 ) is based on the availability and level of training of the local EMS agencies, the patient’s medical status, the potential for decompensation during transport, and the judgment of the EMS agency’s medical officer. Patients transferring from facilities outside of a reasonable driving distance would arrive by a local EMS ambulance to their local airport and then be flown via a Phoenix Air Group (PAG) fixed-wing medical airplane to John F. Kennedy Airport. Because PAG is exceptionally limited in capacity, ASPR would coordinate with HHS to leverage the Department of State’s contract with PAG to access this valuable resource. From John F. Kennedy Airport, FDNY would transport the patient to NYC H+H/Bellevue. Factors considered when determining transport include the capability of the sending facility to treat the patient, while ensuring the safety of its healthcare workers, as well as their ability to provide ongoing care to their community, the patient’s vitality to withstand the transport, EMS capabilities to safely transport the patient to NYC H+H/Bellevue, and the accessibility of PAG if air transport is necessary. If PAG is unavailable for long-distance transport, a patient would be handed off from one EMS agency to the next until they arrive at their final destination.
In parallel, NYC H+H/Bellevue begins to activate its BCU and hospital command center. The unit is prepared by a lead nurse, site manager, and unit lead with refresher just-in-time training, as needed. From the command center, coordination occurs with both external partners—such as the FDNY, New York State DOH, NYC DOHMH, the sending facility, and the CDC—and internal personnel such as hospital leadership, the BCU lead, the nurse lead, the laboratory lead, hospital police, environmental services, and public relations.
There are unique considerations for transporting patients from Puerto Rico and the USVI. Many of the small islands in the USVI do not have airports, thus requiring boat transport of an HCID patient to a nearby island with an airstrip. In addition, if a person under investigation presents in Puerto Rico or the USVI, the best medical and infection control decision may be to transport them to the mainland United States where higher levels of HCID preparedness exist.
Partner Engagement
In May 2023, NYC H+H/Bellevue established 3 levels of engagement with its partners to solicit their input on updating the region’s CONOPS (Figure 3). The first level was the Region 2 CONOPS steering committee, which led the update of the CONOPS. This team—composed of NYC H+H/Bellevue’s special pathogen program director, the NYC H+H ambulatory care chief medical officer, and the NYC DOHMH medical director—was closely advised by the New York State DOH emergency preparedness manager and former New York State DOH leaders.
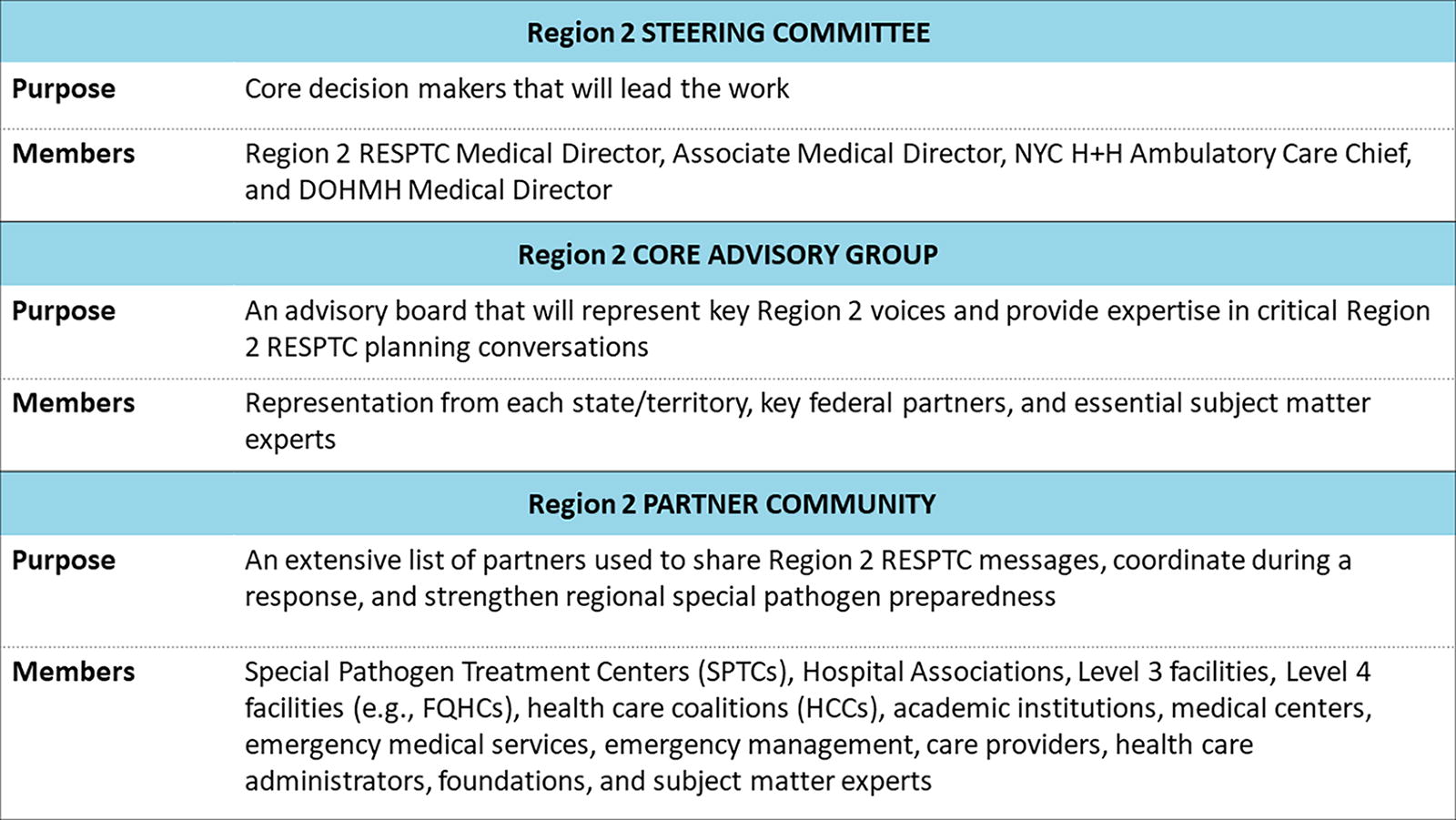
Region 2 partner engagement levels. This table outlines the purpose and members who compose each engagement level. These groups were integral to developing a comprehensive concept of operations. Abbreviations: DOHMH, Department of Health and Mental Hygiene; FQHCs, Federally Qualified Health Centers; HCCs, healthcare coalitions; NYC H+H, New York City Health + Hospitals; RESPTC, Regional Emerging Special Pathogen Treatment Center; SPTCs, Special Pathogen Treatment Centers.
The second level of engagement was with the NSPS Region 2 Core Advisory Group, an advisory board representing key Region 2 voices that provided expertise in critical Region 2 RESPTC planning conversations. Members of the advisory board included public health and healthcare representatives from throughout the region, providing an organic source of engagement and organizational buy-in. This level of engagement allowed members to provide input and ensure that the plan worked for all of Region 2 and the organizations they represent. The advisory board highlighted that high staff turnover, attributed to the COVID-19 pandemic, impacted their number of trained staff. They also sought to exercise the patient transport protocols.
Lastly, the third and largest group engaged in planning was the NSPS Region 2 partner community. The partner community consists of facilities and organizations leveraged to share Region 2 RESPTC messages, coordinate during a response, and strengthen regional special pathogen preparedness. Partner community members include over 500 representatives from healthcare facilities, EMS entities, local governments, hospital associations, academia, and more. For continuous engagement with the partner community, NYC H+H/Bellevue developed a monthly newsletter to share news on potential or ongoing HCID outbreaks and highlight educational resources on the Region 2 RESPTC 7 and NETEC websites. 8 Following the development of the CONOPS, each of these groups remains active for other regional HCID preparedness purposes as needed.
Starting in June 2023, the Region 2 CONOPS steering committee held meetings with key partners from each jurisdiction to update the existing CONOPS plan, last conducted in 2019. By evaluating regional changes and lessons learned since 2019, the updated CONOPS aimed to reflect contemporary patient transfer flows and organizational agreements.
When preparing the approach for targeted partner engagement, the planning committee was intentional in the order in which jurisdictions were engaged. The first conversations were with NYC partners who play a role in the patient transport process including NYC DOHMH, FDNY, and NSPS Level 2 SPTCs. It was critical to understand the needs and capabilities of New York City before expanding to the outer jurisdictions since NYC H+H/Bellevue is situated in the heart of the city and serves as the foundation for special pathogen response in the region. New York City is one of the largest international and domestic travel hubs in the United States, with over 55 million visitors in 2022. 9 With 3 international airports, 2 international shipping ports, and 3 international cruise ports, New York City is at high risk of encountering cases of emerging HCIDs from other parts of the world. The jurisdiction consulted next was New York State (outside of the NYC metropolitan area). The steering committee then met with representatives of the state of New Jersey to address the layers of complexity associated with interstate travel. Lastly, the steering committee met with the territories of Puerto Rico and the USVI. The steering committee scheduled these meetings a month apart to ensure enough time to reconcile items from previous meetings and develop an agenda for the upcoming meeting.
Developing such an intricate plan required ongoing, open channels of communication. Each jurisdiction has unique elements, which made it essential to provide each a platform to voice their needs to the steering committee. Strategies to increase partner engagement and buy-in included early engagement, open dialogue, listening to concerns, and welcoming contributions.
CONOPSorkshop
Culminating on November 16, 2023, NYC H+H/Bellevue and NYC DOHMH cohosted a large-scale workshop to review and discuss the CONOPS for the transfer of a patient with a likely or confirmed HCID. The workshop was well attended, with representatives from federal agencies such as ASPR, representatives from all Region 2 state departments of health, local hospital associations, NETEC, regional NSPS Level 2 SPTCs, and EMS agencies from across the region. The attendance of federal partners showed the significance of this work, not only for Region 2 but also for its applicability to address similar challenges in other US regions and on a national level. To accommodate those who could not attend in person, a virtual option was provided. While organizing hybrid events comes with its challenges, the benefits of providing an online option ensured that partners from across the disparate region could provide input and have their unique challenges heard.
The objectives of this workshop were to bring together players from local and state health departments, emergency managers and directors of infectious disease programs at regional healthcare facilities, and representatives from EMS agencies to assess interjurisdictional and intrajurisdictional notifications and communication protocols while identifying planning gaps for the transport of a suspected or confirmed HCID patient within Region 2. The workshop included an overview of updates to the CONOPS, a discussion about NSPS and the varying levels of care for an HCID patient, and several activities to facilitate dialogue on the plan and systems in place.
Attendees participated in scenario-based discussions and were grouped based on jurisdiction as they worked through 2 patient journey scenarios. The scenarios allowed participants to discuss how and when an HCID patient would be transported from their jurisdictions to NYC H+H/Bellevue. Participants discussed the pros and cons of transport out of jurisdiction, the complexities of patients and movement, and the impacts on the healthcare delivery system to care for an HCID patient. Throughout the workshop, players worked to solve problems in real time, identify areas for further improvement, and discuss strategies to increase the interjurisdictional coordination required to support the safe care of patients with HCIDs.
Aside from working through exercises and fine-tuning processes and procedures, an important feature of the workshop was the opportunity for in-person (and virtual) connections, allowing participants to familiarize themselves with their HCID patient transfer counterparts throughout the large region. Dedicated networking opportunities were available between presentations to enable organic interpersonal and interagency connections. As participants collaborated on scenarios, their relationships strengthened and buy-in increased. Networking in person makes it easier to pick up the phone and collaborate during an actual emergency. The relationships fostered at the workshop will continue to enhance Region 2 readiness for a special pathogen patient.
The Region 2 CONOPS workshop united participants around a single mission and goal to successfully refine and test the regional CONOPS draft. Following the workshop, the steering committee updated the Region 2 CONOPS and, once finalized, distributed it to all relevant parties for approval. In the future, we look to exercise the CONOPS.
Important Elements Contributing to the Revamped CONOPS
Through the steering committee’s efforts to update the CONOPS, the following elements were identified as important contributors to success or crucial gaps to address in the future (Figure 4).
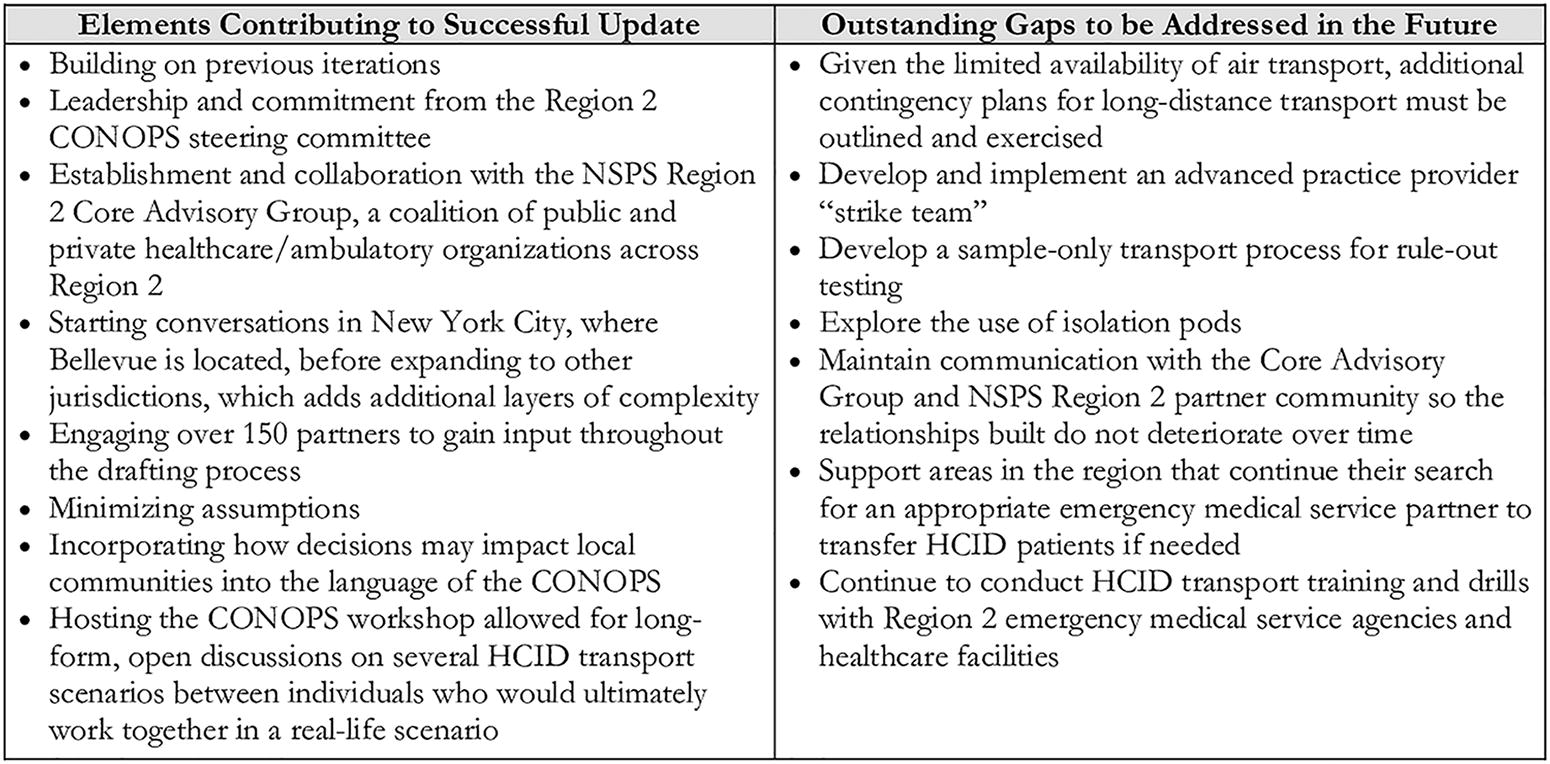
Key elements in updating the Region 2 CONOPS and gaps to address. Abbreviations: CONOPS, concept of operations; HCID, high-consequence infectious disease; NSPS, National Special Pathogen System.
Organization
Two skills necessary to complete a complex CONOPS with a myriad of partners are problem-solving to overcome barriers and organizational abilities to keep the project on track. One strategy employed to push through barriers was to schedule smaller group discussions on specific issues with key partners to achieve a compromise. Arranging participants by jurisdiction allowed them to become familiar with the people they would work most closely with in a real-world activation of the plan. Organizing by jurisdiction mimicked the real-life process in the development stage, making for a robust and inclusive product.
Meetings were scheduled for 90 minutes to facilitate in-depth conversations in order to review the intricacies of a patient transport plan. Effective time management is also critical. Sending participants a draft of the CONOPS and meeting agenda in advance enabled the discussions to be more efficient and focused. The steering committee also limited the number of meeting attendees to ensure that all participants had a chance to voice their thoughts and perspectives.
Another important consideration was to minimize the number of assumptions made throughout the plan to consider as many real-world possibilities as possible. For example, when speaking to the USVI representatives, it became clear that the need for boat transport was critical, which had never previously been included in the CONOPS. Boat transport will now be a future addition to the CONOPS.
Engagement With All Communities in the Region
The steering committee considered the potential impacts of an HCID patient on communities with varying degrees of healthcare resources. For example, EMS agencies in low-resource rural settings may not have adequate training, equipment, and preparation to safely transport a patient infected with an HCID. In addition, an HCID patient could paralyze a small community’s healthcare infrastructure and its ability to provide lifesaving care to other members of the community. It is important to balance the interests of the patient with those of healthcare workers and the local community when deciding whether to transfer an HCID patient. To address this challenging scenario, the creation of an advanced practice provider “strike team” was proposed to provide telehealth recommendations or be deployed directly to a healthcare facility where a patient is isolated. However, obtaining authorization for advanced practice providers to treat a patient at any facility across multiple states remains a massive bureaucratic and regulatory hurdle. Another key consideration is that shipping a diagnostic testing sample is often more feasible than moving a patient. This option is ideal for a stable patient isolated in a facility that can provide supportive care. If a frontline facility provides care for an HCID patient, NYC H+H/Bellevue must ensure they have the proper personal protective equipment accompanied by training to prevent transmission to healthcare workers.
One of the keys considerations was ensuring that partner engagement was inclusive. The steering committee actively built the CONOPS through the lens of inclusivity, with partners from across the region represented during all steps of a patient transfer. Partners had high levels of expertise, each with diverse backgrounds, experiences, and perspectives. Ensuring the diversity of partners involved in creating the CONOPS is critical to developing a plan that will work well for everyone. Listening to and learning from all partners ensures equity and enhances regional readiness and preparedness to respond to an HCID outbreak.
The relationships built between agencies through engagement in the CONOPS development may be more important than the plan itself. Each patient’s transport will be unique, making it impossible to plan for every scenario. Personal connections among partners allows them to become familiar with each other and facilitates future coordination efforts. When the time comes to transport an HCID patient, knowing who to call, how to contact them, and how to work well together is integral to ensuring that the response goes smoothly. The plan may change with the situation, but the individuals and their roles will remain consistent.
Impact on the Local Healthcare System
Region 2 has substantial geographic diversity, each requiring specific considerations. In the rural outskirts of New York and New Jersey, many hospitals and ambulance services are small and understaffed.10,11 Having an HCID patient in a hospital could shut it down completely, preventing the hospital from providing lifesaving care to the communities they serve. Likewise, EMS agencies in these areas have limited ambulances and staff. A 2023 report found that 82.2% of counties in the state of New York have an ambulance desert, defined as living more than a 25-minute drive from where an ambulance is stationed. 12 Using a small town, local ambulance to transport an HCID patient could mean the community would be without an ambulance for an extended period of time, considering the time required to transport a patient and drive back from the dropoff location as well as the time needed to decontaminate an ambulance post-transport. Thus, the decision to transport a person under investigation must also consider the repercussions to the local community.
Limitations of HCID Air Transport
Lastly, it is important to remember that air transport resources may not be available when they are needed. Although air transport is included in the regional CONOPS plan, there are a limited number of planes and airlines capable of safely transporting an HCID patient across the region. In the event of a large outbreak, accessibility of air transport will likely be severely limited. In such a scenario, other solutions must be considered such as a ground ambulance to NYC H+H/Bellevue or a closer HHS Region 2 NSPS Level 2 SPTC.
Crucial Gaps
Through conversations with partners across HHS Region 2, NYC H+H/Bellevue identified gaps in special pathogen management capabilities. One area for improvement was the need for training and exercises in special pathogen patient transport due to the high staff turnover attributed to the COVID-19 pandemic and its impact on the healthcare workforce. As a result of collaboration on the CONOPS, more Region 2 partners are now familiar with the training and resources that both NETEC and NYC H+H/Bellevue provide.
Looking beyond the interagency workshop hosted by NYC H+H/Bellevue on behalf of HHS Region 2, NYC H+H/Bellevue aims to continue expanding the interagency communication that brought an updated CONOPS to fruition. Using the additional insights gained at the workshop, the CONOPS was updated. However, the CONOPS is a living document that will be adjusted and altered as the capabilities and needs of the region change over time. Some gaps identified at the workshop require more discussions before being formally incorporated into future iterations of the plan.
To improve response capabilities and maximize the level of care provided to sick patients in the future while minimizing their impact on the community, NYC H+H/Bellevue has begun work on developing an advanced practice provider strike team to aid the initial healthcare facility as well as enhance EMS capabilities across the region. Future versions of the CONOPS may include the strike team, as well as a sample-only transport option and deployment of isolation pods, which create a negative pressure environment for patient isolation when a transfer is not necessary or possible.
Conclusion
Thanks to the dedication and leadership of the Region 2 RESPTC’s CONOPS steering committee and in close collaboration with key regional partners, the regional HCID patient transport plan has been updated and reviewed to ensure the special pathogen preparedness of the region, informed by the recent COVID-19 and mpox responses. The Region 2 patient transport workshop helped foster collaboration and began to break down the various barriers to patient transportation. Workshop participants brought back insights to further improve their jurisdictional plans with a better understanding of their role within the regional plan.
The current version of the CONOPS is a work in progress but remains invaluable in an emergency. As more information becomes available, the plan will be refined and expanded to include the breadth of contingencies at our disposal. Engaging regional representatives and partners early was integral to success. The success of this plan is not attributed to any single agency, but rather it relied on a myriad of individuals from different backgrounds and organizations who came together to prioritize patient safety and care for the larger community, consistent with the NSPS vision. Engaging with regional partners was a collaborative effort with active learning on all sides. Incorporating individuals from different disciplines—including physicians, registered nurses, paramedics, hospital leadership and operations, EMS leadership, and state and local departments of health—from the outset was fundamental to the creation of an inclusive, robust CONOPS.
Footnotes
Acknowledgments
Vikramjit Mukherjee, Andrew Wallach, Jory Guttsman, Laura Hillard and Anthony Lo Piccolo are members of Health and Human Service’s Region 2 Regional Emerging Special Pathogen Treatment Center at NYC H+H/Bellevue, which receives funding from the Administration for Strategic Preparedness and Response. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Office of Readiness and Response, Centers for Disease Control and Prevention.