
Abstract
High-level isolation units (HLIUs) have been established by countries to provide safe and optimal medical care for patients with high-consequence infectious diseases. We aimed to identify global high-level isolation capabilities and determine gaps and priorities of global HLIUs, using a multiple method approach that included a systematic review of published and gray literature and a review of Joint External Evaluations and Global Health Security Index reports from 112 countries. A follow-up electronic survey was distributed to identified HLIUs. The landscape analysis found 44 previously designated/self-described HLIUs in 19 countries. An additional 33 countries had potential HLIUs; however, there were not enough details on capabilities to determine if they fit the HLIU definition. An electronic survey was distributed to 36 HLIUs to validate landscape analysis findings and to understand challenges, best practices, and priorities for increased networking with a global HLIU cohort; 31 (86%) HLIUs responded. Responses revealed an additional 30 confirmed HLIUs that were not identified in the landscape analysis. To our knowledge, this was the first mapping and the largest ever survey of global HLIUs. Survey findings identified major gaps in visibility of HLIUs: while our landscape analysis initially identified 44 units, the survey unveiled an additional 30 HLIUs that had not been previously identified or confirmed. The lack of formalized regional or global coordinating organizations exacerbates these visibility gaps. The unique characteristics and capabilities of these facilities, coupled with the likelihood these units serve as core components of national health security plans, provides an opportunity for increased connection and networking to advance the field of high-level isolation and address identified gaps in coordination, build an evidence base for HLIU approaches, and inform HLIU definitions and key components.
Introduction
I
Distinct from conventional hospital isolation wards, HLIUs are equipped with engineering controls generally analogous to biosafety level (BSL) 4 laboratories, highly trained teams, and infection prevention and control measures atypical of routine clinical care.2,5 The 2001 anthrax attacks in the United States and the 2003 severe acute respiratory syndrome (SARS) pandemic prompted the construction of several HLIUs in Europe and the United States; however, these facilities were used sparingly for infrequent HCID cases, if at all.2,4,5 It was not until the 2014-2016 West Africa EVD epidemic that HLIUs were collectively leveraged during an outbreak, when confirmed cases were treated in HLIUs in Europe and the United States. Nosocomial transmission declined when patients were cared for in an HLIU, and mortality rates for patients treated in HLIUs in Europe and the United States were significantly lower than mortality rates for patients treated in West Africa during the outbreak (18.5% compared with ranges of 37% to 74%, respectively).6–8 Since 2014, HLIUs have provided care for patients with Lassa fever,9–11 Crimean-Congo hemorrhagic fever,12,13 and Mpox (clade I), 14 and they played pivotal roles during the early weeks of the COVID-19 pandemic, when SARS-CoV-2 emerged as a novel virus. 15 Despite HLIUs providing these roles and several units published findings on their experiences,7–14 little has been published on the current landscape of global high-level isolation, 16 including locations, requirements or standards for HLIU designation, and formalized networks of HLIUs.
The National Emerging Special Pathogens Training and Education Center (NETEC) was established in 2015 to enhance capabilities of healthcare facilities within the United States to prepare for and respond to HCID events. 17 In 2021, NETEC launched its International Partnerships and Programs (IPP) to strengthen collaboration and partnerships among global HLIUs. 16 This focus was grounded on the recognition that increased collaboration among this unique cohort of facilities can advance the fields of high-level isolation and HCIDs by facilitating information-sharing and knowledge generation, promoting research collaborations and innovation, advancing practices, and demonstrating the value of HLIUs and accompanying specialized capabilities locally, nationally, and globally. In 2022, the NETEC IPP team conducted a landscape analysis to inform its strategy. The aims of this study were to identify global high-level isolation capabilities and previous HLIU efforts, determine gaps and priorities of global units, and ultimately establish relationships among existing global HLIUs. This article describes the methodology and key findings from that landscape analysis, as well as a subsequent survey conducted to validate and improve awareness of HLIU locations and priorities.
Methods
Landscape Analysis
A multipronged approach was used to identify global high-level isolation capabilities. We used the definition of HLIU from the European Network for Infectious Diseases (EUNID) in 2009: “a [healthcare] facility specifically designed to provide safe, secure, high-quality, and appropriate care, with optimal infection containment and infection prevention and control procedures, for a single patient or a small number of patients who have, or who may have, a highly infectious disease.” 2
From January to April 2022, a literature review was conducted on PubMed and Embase using combinations of the keywords “biocontainment unit,” “high-level isolation unit,” “high-consequence infectious disease,” “special isolation,” “high-level containment,” and “highly infectious disease.” We used a snowballing method to identify other articles through reference checks to expand the search strategy. The literature search yielded 311 items. Titles and abstracts for all results were screened for peer-reviewed articles that included the following details about HLIUs: clinical and operational capabilities, location, experiences, and procedures and protocols. Full articles were reviewed if the abstract described an HLIU or facility that had potential high-level isolation capabilities.
Following the literature search, we conducted a web search of gray literature using combinations of the key terms described above. The search was augmented with the inclusion of specific continents or countries to aid in targeting the search. The web search identified approximately 80 news articles, websites, and publications relating to a confirmed or potential HLIU. Additionally, reports produced by organizations with mandates or interests related to HCIDs and their isolation were reviewed. These included Joint External Evaluation (JEE) reports from 112 countries, 18 Biological Weapons Convention reports, 19 Global Health Security Index 2021 country reports, 20 and select United Nations Security Council national reports related to resolution 1540. 21 These reports were reviewed for keywords and information on confirmed or potential high-level isolation capabilities. All relevant journal articles, web sources, and reports were reviewed for specific information related to confirmed or potential HLIUs, including their locations, capabilities, and leadership contact information. Sources were then reviewed independently by 2 of the authors to determine if the facility met the EUNID definition of an HLIU. HLIUs were considered “confirmed” if they were previously designated/self-reported and information on capabilities or status was found since 2014, the time when many HLIUs were rapidly designated for the EVD epidemic. HLIUs were considered “potential” if they were previously designated but no updated information on status was found or there was reference to advanced capabilities but not enough information to determine if those capabilities would meet the definition of an HLIU. All sources were in English, although the Global Health Security Index country reports included non-English sources.
Survey of HLIU Priorities and Networking Interests
The landscape analysis was designed to identify potential HLIU partners and collaboration areas to inform NETEC IPP’s strategy and focus. Findings from the landscape analysis coupled with a list of HLIUs generated an opportunity to validate findings and further guide NETEC IPP efforts through a survey to existing HLIUs.
Of the 44 HLIUs identified in the landscape analysis, we found updated contact information for 36 units. In December 2022, a 42-question electronic survey, developed using Qualtrics software (Qualtrics, Provo, Utah), was disseminated via email to representatives from those 36 HLIUs. The survey aimed to understand HLIUs’ areas of challenges and best practices and priorities for increased networking and collaboration with a global HLIU cohort, as well as to inventory their high-level capabilities and engagement in HLIU networks or activities; the latter 2 areas are the subject of another manuscript. Participation in the survey was voluntary and individual responses were confidential. Data were coded and analyzed using descriptive statistics in Microsoft Excel.
Results
Landscape Analysis: Terminology and Definitions
Several terms and definitions have been adopted to describe both the specially designed units (referred to as HLIUs in this manuscript) and the diseases warranting this level of advanced isolation capabilities. We found HCID to be the most common and current term for the disease; however, the terms “highly infectious disease” and “highly hazardous communicable disease” were also used. “HLIU” was the most globally used term for the unit, but “biocontainment patient care unit” was most common in North American publications. Other terms used included “special pathogens unit,” “high-level containment care unit,” and “high degree isolation unit.”
Table 1 details terms, definitions, and pathogens warranting care in a specialized unit that have been adopted by networks or groups that have previously defined the terms. Pathogens vary substantially in the level of care required and include certain viral hemorrhagic fevers, Middle East respiratory coronavirus (MERS-CoV) and severe acute respiratory syndrome coronavirus (SARS-CoV-1), Nipah virus, smallpox, and emerging highly pathogenic agents.
Definitions, Terminology, and Lists of Diseases Warranting High-Level Isolation by Previous High-Level Isolation Unit Efforts
Abbreviations: BSL-4, biosafety level 4; HCID, high-consequence infectious disease; HLCC, high-level containment care.
Landscape Analysis: Previous Efforts in HLIU Coordination
Two regional consensus efforts were conducted in the mid-2000s: (1) a 2006 US consensus meeting attended by civilian and military professionals with expertise in high-level isolation that concluded with a consensus statement outlining the key technical, infection control, and ethical issues in planning, designing, and constructing an HLIU5; and (2) meetings in Europe supported by the European Commission—through the EUNID (2006-2009) and European Network for Highly Infectious Diseases (EuroNHID) projects (2009-2011)—resulted in consensus recommendations for the framework and design of HLIUs, checklists to assess HLIUs, and a mapping of high-level isolation capabilities in Europe.2,23,24 As of 2010, EuroNHID reported 18 HLIUs in Europe and mentioned national networks of HLIUs in France and Germany. 24 The US and European consensus efforts generated recommendations that remain the pillars for designing an HLIU.
National networks of HLIUs were identified in several countries, including France, 25 Germany,26,27 Japan, 28 Spain, 29 the United Kingdom, 30 and the United States. 31 While information on requirements for these facilities and descriptions of how HLIUs collaborate, coordinate, and network were available for some countries, this information was lacking for others.26,27,30-33 We found 2 cases of international networking of HLIUs: (1) representatives from 22 HLIUs convened for a workshop in 2018 to share best practices and approaches based on experiences caring for HCID cases, and (2) an informal network of 5 HLIUs across the United States, Europe, and Asia was established in 2017 and was leveraged for rapid knowledge exchange in the first months of the COVID-19 pandemic.34,35
NETEC’s IPP is building on both efforts by regularly convening HLIU representatives to discuss and address unique challenges facing HLIUs. 36 However, we found no formalized networks or convening bodies that oversee or convene HLIUs regionally or globally.
Landscape Analysis: Locations of Global HLIUs
Findings on global high-level isolation capabilities are detailed by country in Table 2 and mapped in Figure 1. Nearly all identified HLIUs are in high-income countries in Europe, North America, Australia, and Asia. We found references to “special isolation” facilities, designated hospitals for EVD cases in 2014, or dedicated infectious disease units in several low- or middle-income countries; however, further details on the existence and specific capabilities of these facilities were not available. Many HLIUs were established following the 2014-2016 West Africa EVD epidemic; for many of these units, however, it is uncertain whether those capabilities were maintained after the immediate threat of the epidemic waned due to a lack of references or updated information since 2015 or 2016. Conversely, we found several instances of HLIUs being established in the last several years.
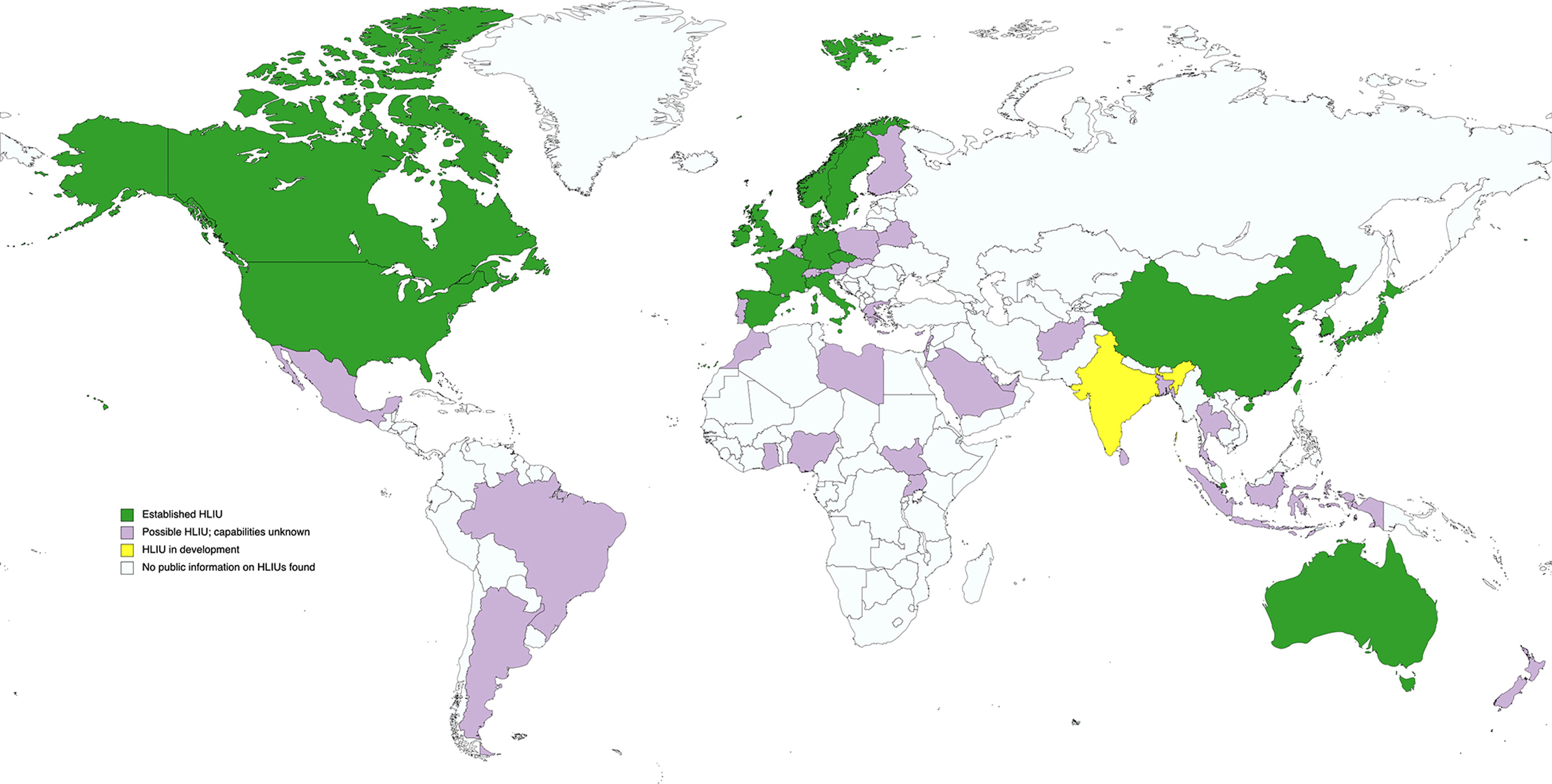
Global mapping of confirmed (established), in development (planned), and potential (possible) high-level isolation units (HLIUs) based on a search of peer-reviewed and gray literature, April 2022. Map created with mapchart.net.
Potential and Confirmed High-Level Isolation Capabilities, Organized by Country
Note: High-level isolation capabilities were identified through a global landscape analysis of literature conducted January to April 2022.
“Confirmed” indicates the unit was previously designated or self-reported as an HLIU and information on unit capabilities/status have been published since 2014. “Potential” indicates previous designation as an HLIU with no information on status since 2014, or there was reference to advanced capabilities but not enough information to determine if those capabilities would meet the definition of an HLIU.
At the time of the landscape analysis, there were 10 federally designated HLIUs in the United States. In September 2022, an additional 3 HLIUs were designated.
Abbreviations: EUNID, European Network for Infectious Diseases; EuroNHID, European Network for Highly Infectious Diseases; EVD, Ebola virus disease; GHS, Global Health Security; HCID, high-consequence infectious disease; HLIU, high-level isolation unit; JEE, Joint External Evaluation; MERS, Middle East respiratory syndrome; SARS, severe acute respiratory syndrome; SEARO, South-East Asia Region Office; VHF, viral hemorrhagic fever, WHO, World Health Organization.
In total, we found 44 previously designated/self-described HLIUs in 19 countries. Of note, the landscape analysis was conducted prior to the naming of 3 additional US units as Regional Emerging Special Pathogens Treatment Centers 88 ; as such, only the 10 US HLIUs that were designated as of early 2022 were included in these data. Findings indicated another 2 units were in development; 1 of these units was in a country with a confirmed HLIU (Italy) 64 while the other was in a country without reference to established HLIUs (India). 76 An additional 33 countries had potential HLIUs; however, there were not enough details on capabilities to determine if they fit the HLIU definition. We found no confirmed reference to HLIUs in Sub-Saharan Africa, Latin America, or the Middle East and North Africa regions.
Survey of HLIU Priorities and Networking Interests
Of the 36 HLIUs that were sent the survey, 31 (86%) completed it, representing units from 16 countries in Asia, Europe, North America, and the Pacific. Notably, 2 of the 5 facilities that did not complete the survey no longer had active HLIU programs. Responding HLIUs were asked to list the number of HLIUs in their country and names of any HLIUs they currently networked or collaborated with outside of their country. Of the 16 countries represented in the survey, 12 (75%) had multiple HLIUs, although several respondents noted that capabilities varied between those designated units. In total, responses revealed an additional 30 confirmed HLIUs that were not identified in the landscape analysis. Several of these were considered “potential” HLIUs in the landscape analysis, as they were listed in the EuroNHID project as HLIUs but updated information on their capabilities was not available at the time of the study. However, most of these newly identified HLIUs are in addition to units in countries where we found reference to only 1 or 2 HLIUs through the landscape analysis.
Responding HLIUs reported several areas of challenges and best practices (Figure 2). Maintaining a cadre of highly trained staff was the most cited challenge (n=22, 71%), followed by global networking and coordination with other HLIUs and hospitals in their area (n=20, 65%), research (n=17, 55%), and training (n=18, 58%). All responding units indicated their willingness to share best practices with other HLIUs, with training (n=21, 68%), physical infrastructure/design (n=21, 68%), and infection prevention and control practices (n=19, 61%) being the most cited areas where these best practices were available. All 31 responding HLIUs (100%) reported interest in networking with other HLIUs, including through virtual or in-person meetings (n=30, 97%), joint trainings or exercises (n=30, 97%), knowledge-sharing webinars (n=29, 94%), and collaborative multisite clinical research protocols (n=27, 87%) (Figure 3).
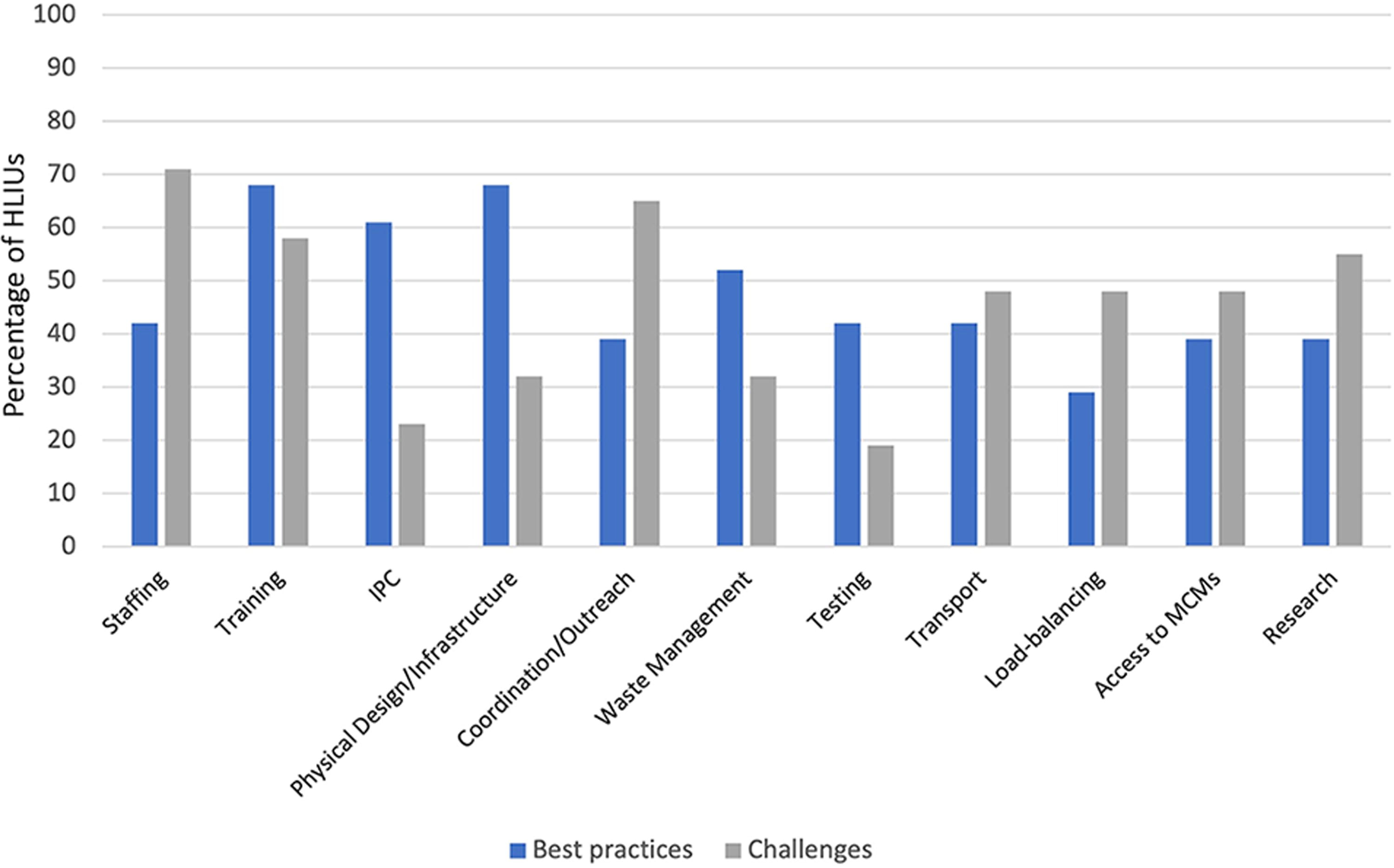
Reported best practices/innovations and challenges or areas that could benefit from increased global networking and collaboration, by percentage of responding HLIUs (N=31). Abbreviations: HLIU, high-level isolation unit; IPC, infection prevention and control; MCM, medical countermeasure.
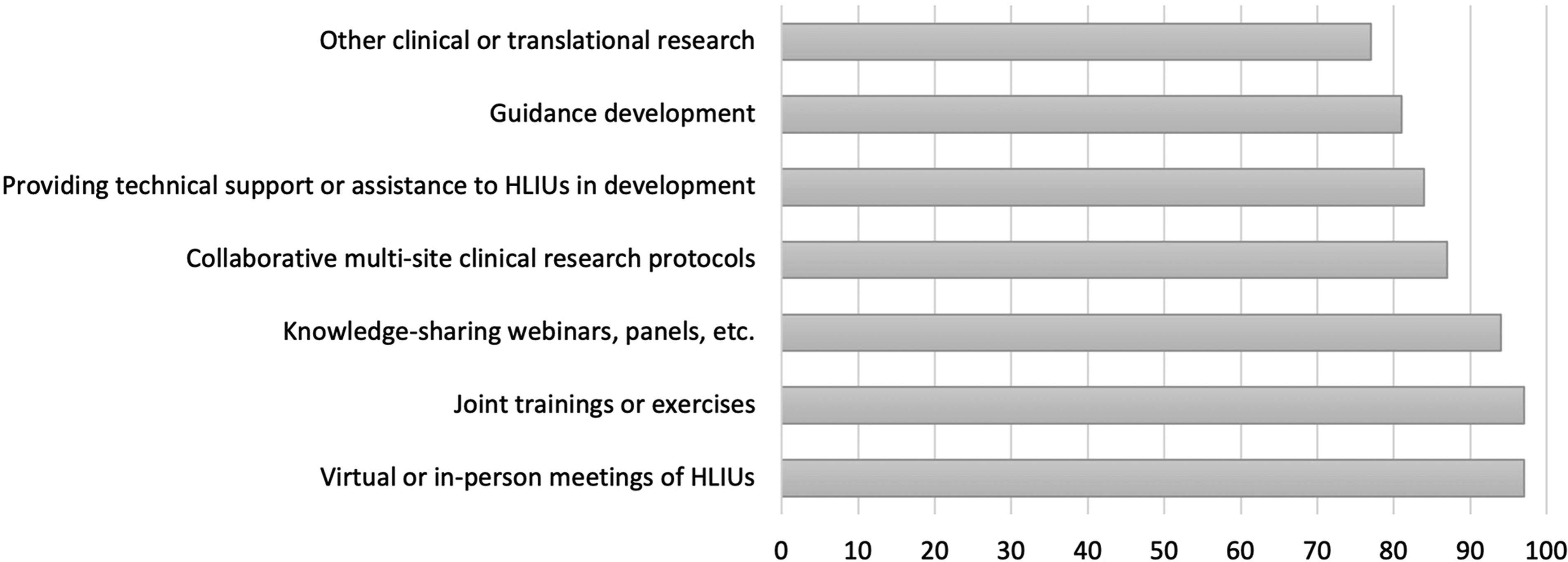
Reported priority areas for increased global networking and collaboration, by percentage of responding HLIUs (N=31). Abbreviation: HLIU, high-level isolation unit.
Discussion
The primary functions of HLIUs are to provide safe and effective care for patients with HCIDs and to mitigate transmission risks to healthcare personnel and the community through physical infrastructure and other engineering controls, administrative controls, personal protective equipment, and highly trained multidisciplinary teams.2,5 As such, HLIU processes and approaches differ from routine clinical settings, and they face challenges atypical of other clinical teams. Common challenges reported by HLIUs in the literature (summarized in Lukowski et al 89 ) and in the survey include determining (1) the appropriate frequency, duration, and type of training necessary for HLIU team members to maintain competencies; (2) optimal infection prevention and control processes; (3) strategies to recruit and maintain highly trained teams, and (4) physical design and necessary infrastructure features. Although previous consensus efforts have agreed upon critical components of HLIUs,2,5 and although facilities that have cared for patients with HCIDs have published their approaches, 89 there remains a lack of data and validation testing to guide process development and physical design. There is an opportunity to advance these approaches by cultivating forums for HLIUs to share best practices and collaborate to conduct translational and applied research.
It is unknown how frequently and to what extent existing global HLIUs are being assessed. The EuroNHID project developed checklists to assess isolation facilities in the European region in 2010 and used those checklists to evaluate the capabilities of 48 isolation facilities in 16 countries, including 18 facilities that fulfilled the definition of an HLIU. 24 However, this assessment was conducted over a decade ago, and no other information was found on how frequently, if at all, these 18 units have since been assessed nationally or regionally. In Germany, national regulations describe technical rules for biological agents including constructional and technical requirements for HLIUs, while the UK-designated facilities for airborne HCIDs have specifications from NHS England.32,33 In the United States, NETEC facilitates annual assessments of the 13 federally designated HLIUs, a requirement for their designation by the US Administration for Strategic Preparedness and Response. 90 The EuroNHID project found that most isolation centers in Europe did not have access to legally binding regulations on issues of infrastructural or technical requirements at the time of establishment; it is unclear if over 10 years later more legal requirements are in place. It is also unknown if other countries have requirements (legal or otherwise) for HLIUs. The lack of a standard definition for what constitutes an HLIU results in ambiguity in a shared understanding of the minimum requirements and resources to optimally protect healthcare teams. Further, although outcomes of the US consensus meeting and the EUNID and EuroNHID projects continue to be guiding posts for the critical components of an HLIU, the last decade has vastly increased the operational experience of many HLIUs and transformed the field of HCID preparedness and response; indeed, there is much to be learned just from the roles HLIUs played in the early COVID-19 pandemic and their response to a novel pathogen. There is opportunity for the global HLIU community to collaborate to close this gap and update previous consensus efforts to define recommendations for HLIUs.
As evidenced by comparing results from the landscape analysis and HLIU survey, there are major visibility gaps in global high-level isolation capabilities. The survey identified an additional 30 HLIUs for which we found either no confirmed reference in the literature or web searches, or the reference(s) to the unit were dated more than 10 years ago. This lack of global visibility has several implications, including challenges in rapidly identifying hospitals to transport HCID cases within countries, regionally, or globally; gaps in perceived regional and global preparedness for HCID cases; HLIUs working in silos to address problems and challenges that many other units likely face (eg, recruiting and maintaining highly trained teams, funding and/or sustaining the unit and its capabilities, determining optimal infection prevention and control processes); and potential resource distribution gaps for HLIUs. Moreover, to our knowledge, informed by results of the landscape analysis and survey, we found no formalized networks or convening bodies that oversee HLIUs regionally or globally that would maintain a comprehensive list of known global HLIUs. There is an opportunity for an international organization to document these resources and convene a network to collectively advance the gaps, challenges, and issues identified in the landscape analysis and survey.
Notably, an initiative by the European Commission, the Strengthened International Health Regulations and Preparedness (SHARP) Joint Action project, published a report in fall 2023 (after our landscape analysis was complete) identifying 47 HLIUs in 16 European countries. 91 While this is an important addition to the literature, results were self-reported by member states and not by individual HLIUs using a clinical vignette; it is unclear how many of those units would fit the definition of an HLIU. In addition to validating some of our landscape analysis findings, the SHARP Joint Action project reported HLIUs in several countries (eg, Estonia, Lithuania, Slovenia) where we found no previous HLIU reference. In addition to a mapping of HLIUs, the SHARP Joint Action project conducted a feasibility study for a formal HCID expert clinical support network. Such regional and international clinical networks can strengthen national HCID plans as well as broader global health security.
There is an economic element and inherent inequity to the location of HLIUs, as nearly all identified units were in high-income countries. HLIUs have previously reported significant financial and resource demands to establish capabilities and sustain readiness. 34 Although these costs are a barrier to HLIU development regardless of location, the lack of identified HLIUs in 3 populous world regions means that only a small minority of the global population has access to an HLIU. It is important to acknowledge that there has undoubtedly been successful management and care of patients in HCID outbreaks in non-HLIU facilities in these regions; however, HLIU capabilities offer additional safeguards to enhance the protection of healthcare teams and provide advanced controls for delivering higher-level supportive care. Further exploration is warranted to determine (1) whether capabilities exist in these regions (but are not public), (2) the barriers to establishing such capabilities in these regions, (3) interest of regional and national authorities to strengthen or establish these capabilities, and (4) the need for or potential value, structure, and role of HLIUs in these regions. There are also opportunities for the global HLIU collective to publish findings on how to optimize the HLIU program to offset costs of maintenance, which may include evaluating the return on investment for these units. Such an analysis should look at not only the individual hospital cost-benefits, but also those of the local, regional, and national communities.
This research was not without limitations. The list of identified HLIUs in the landscape analysis is not exhaustive; as was found in the survey, many countries/hospitals have high-level isolation capabilities but have not published or been publicized. The landscape analysis focused only on HLIU capabilities and did not capture the capacity of these units (ie, number of HLIU beds). The search was also conducted in English, which possibly excluded local or national references to high-level isolation capabilities. The current definitions of what constitutes an HLIU are vague; while the landscape analysis and subsequent selection of HLIUs for the survey included facilities that have been reported in the literature or media as HLIUs, the capabilities between these facilities vary. Moreover, many of the listed units in the landscape analysis had previously been identified as HLIUs, but their current capabilities and designations were unknown. This is especially true for many of the listed European units that were assessed in the 2009-2011 project; whether they maintain that designation over a decade later is unknown. Likewise, several units listed as “unknown capabilities” in some regions were designated units for EVD in 2014-2016, but we could find no further information on whether those capabilities were sustained after the epidemic ceased. Lastly, we did not validate the HLIUs that were reported by responding HLIUs in the survey.
Conclusion
NETEC’s IPP conducted a landscape analysis of global high-level isolation capabilities to inform its strategy and guide its efforts. To strengthen and validate the findings, we disseminated a survey to 36 known HLIUs identified in the landscape analysis. To our knowledge, this was the largest ever survey of global HLIUs. Survey findings identified major gaps in the visibility of HLIUs: while our landscape analysis initially identified 44 units, the survey unveiled an additional 30 HLIUs that had not been previously identified or confirmed. The additional fact that 2 of the HLIUs invited to respond to the survey were no longer active programs reflects the ever-evolving global landscape. The lack of formalized regional or global coordinating organizations exacerbates these visibility gaps.
The unique characteristics and capabilities of these facilities, coupled with the likelihood these units serve as core components of national health security plans, provides an opportunity for increased connection and networking to advance the field of high-level isolation and address identified gaps in coordination, build an evidence base for HLIU approaches, and inform HLIU definitions and key components. Increased networking of these units can enhance opportunities for research and collaboration to inform and improve approaches, procedures, and processes; in turn, this could lead to validation testing and evidence-based standards or guidelines, particularly around areas unique to HLIUs where evidence is currently scarce or lacking. More formalized mechanisms of engagement could increase visibility of these facilities and be leveraged to advocate for resourcing and funding to sustain HLIU programs. Lastly, facilitating networking of this unique cohort could generate innovation and knowledge advancements more broadly for HCID readiness.
Footnotes
Acknowledgments
The National Emerging Special Pathogens Training and Education Center is funded by the US Administration for Strategic Preparedness and Response (U3REP150549).