
Abstract

Keywords
Introduction
M
Today, the system is mostly used to support state and local medical resources for domestic disaster events through the deployment of disaster medical assistance teams, with limited deployment of its patient movement or definitive care components.4‐6 Since its inception, the NDMS has never had to activate for its original purpose to support a large-scale combat operation. Therefore, it is unclear whether this system could handle the medical surge needs required for such a demanding and complex event.4,5 Furthermore, while the US military has not been required to manage hundreds of combat casualties daily over an extended period since World War II,6,7 a repeat of such a scenario is increasingly conceivable given the current state of international conflict and tension in Europe, the Middle East, and Asia. 8
Recognizing this potential national security threat, Congress directed the US Secretary of Defense to conduct an NDMS Pilot Program (NDMS Pilot) to strengthen interoperability between the NDMS’s military and civilian partners and to expand the medical surge capabilities and capacities of the NDMS.9,10 Launched in 2020, this program aims to establish and strengthen partnerships with public, private, and nonprofit healthcare organizations to achieve these objectives. 11 The NDMS Pilot is being conducted over a 5-year period at regional NDMS sites comprising local networks of military, federal, and civilian healthcare entities (Figure 1). These sites (Denver, Colorado; Omaha, Nebraska; Sacramento, California; San Antonio, Texas; and the National Capital Region in the greater Washington, DC, metropolitan area) were selected based on numerous factors, including proximity to military transportation hubs, previously demonstrated surge capacity, and established expertise in disaster medicine and public health response, advanced trauma care, and combat casualty care. 11 The NDMS Pilot’s work focuses on the scenario of providing definitive care for 1,000 military casualties repatriated to the United States daily for 100 consecutive days.
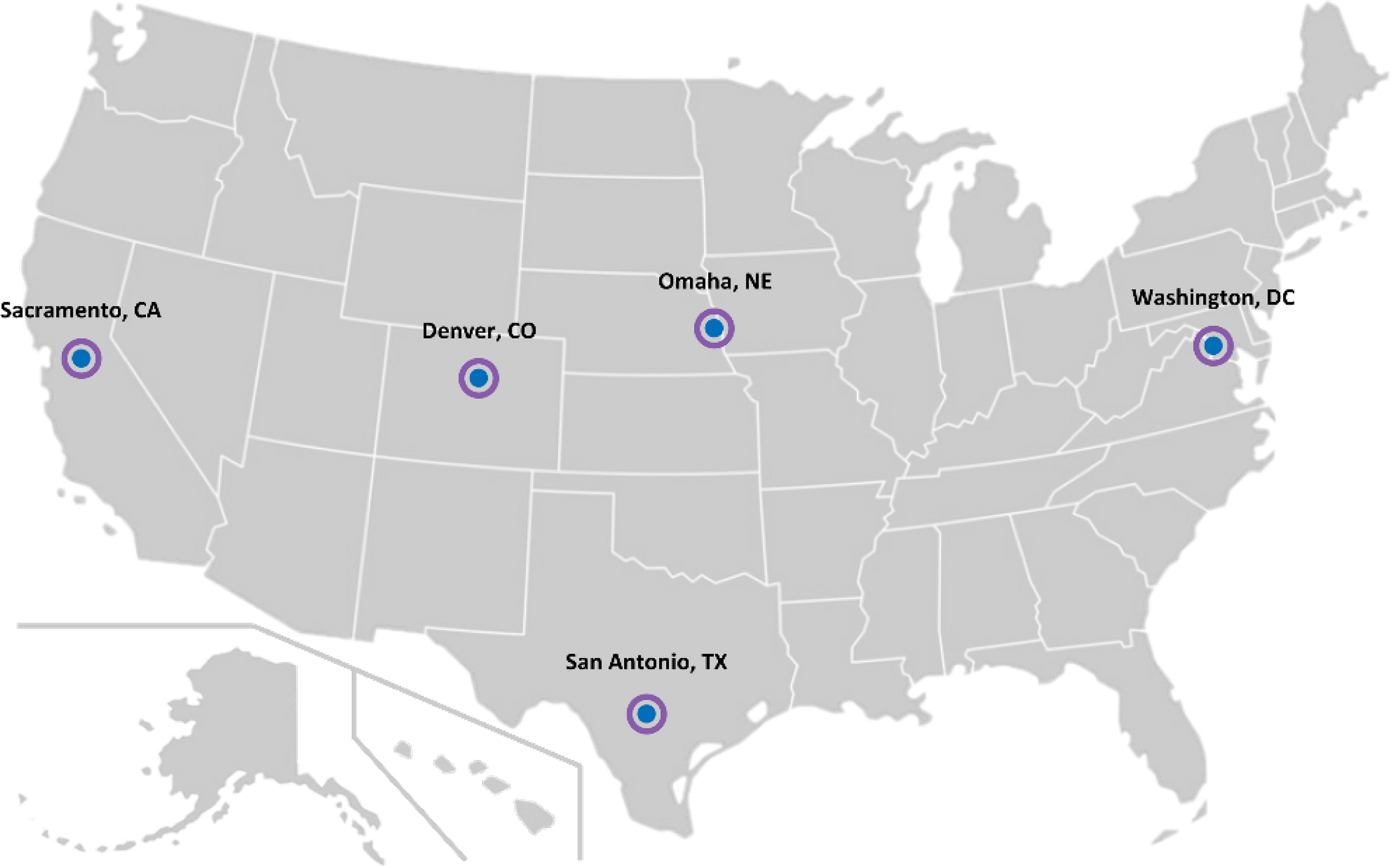
Map of the 5 National Disaster Medical System Pilot Program sites.
The NDMS Pilot Program is being executed in 3 strategic phases: (1) initial study, (2) implementation, and (3) expansion (Figure 2). As of April 2024, the NDMS Pilot has completed its initial study effort and the first 2 years of its implementation phase. The implementation stage of the NDMS Pilot aims to apply a partner-based approach to further study and prioritize solutions identified in foundational research, execute suggested interventions, and measure program effectiveness.

The National Disaster Medical System Pilot Program timeline.
This commentary describes the conclusion of the NDMS Pilot’s previously published foundational research studies and the major efforts of the first 2 years of implementation activities. Year 1 of the NDMS Pilot focused on initial planning by establishing field implementation teams at each site, developing site-specific and cross-site plans for improving the NDMS’s medical surge capacity, and conducting more targeted research studies addressing operational concerns raised during the initial study phase. Year 2 efforts focused on operationalizing the improvements suggested in Year 1 through projects led by field implementation teams and local stakeholders, conducting further targeted research that addressed system-wide issues in the NDMS, and establishing the NDMS Pilot evaluation plan to assess the impact and effectiveness of the resultant activities.
Operational Translation of Interoperability Study Findings
The initial study phase of the NDMS Pilot, the Military–Civilian NDMS Interoperability Study (MCNIS), was completed in September 2021. This study was designed to inform the NDMS Pilot’s implementation by providing an assessment of the NDMS’s current capabilities for providing definitive medical care for large numbers of combat casualties.5,12 As described elsewhere, a thematic analysis of facilitated discussions with NDMS stakeholders identified 6 primary themes of suggested improvements: (1) coordination, collaboration, and communication; (2) funding; (3) staffing; (4) surge capacity; (5) training, education, and exercises; and (6) metrics, benchmarks, and modeling. 5 These qualitatively defined themes and related issues were subsequently refined, validated, and prioritized through a web-based quantitative survey administered to 87 NDMS stakeholders. 12 As a result of this study, the NDMS Pilot identified specific opportunities for interventions prior to its implementation phase, with a focus on improving coordination, collaboration, and communication between federal, state, and local governments and private sector healthcare entities.
To ensure the NDMS Pilot’s implementation efforts would align with stakeholder priorities, a multidisciplinary working group meeting of 107 key military, federal interagency, and civilian NDMS stakeholders was held on September 30, 2021. The meeting objective was to solicit suggestions for the NDMS Pilot’s initial implementation efforts in light of the MCNIS findings. Participating stakeholders were selected using purposive sampling methods that prioritized senior leaders in NDMS-participating federal agencies, personnel from civilian and private healthcare facilities, and emergency managers from NDMS Federal Coordinating Centers (FCCs). An FCC is defined as a DOD or VA federal facility or patient movement capability “located in a metropolitan area of the United States, responsible for day-to-day coordination of planning, training, and operations in one or more assigned geographic NDMS Patient Reception Areas.” 13 The mission of the FCC is “to receive, assess, stage, track, and transport patients, affected by a disaster or national emergency, to a participating [NDMS] medical facility capable of providing the required definitive care.” The stakeholder sample ensured responses captured a holistic range of expertise in clinical, financial, operational, and administrative aspects of the NDMS. Attendees were asked to rank-order specific opportunities and weaknesses identified across the 6 MCNIS improvement themes from highest to lowest priority using the audience response system, Poll Everywhere (Poll Everywhere, San Francisco, CA). The Poll Everywhere results identified 54 total recommended interventions across themes and stakeholder types, which included 35 distinct opportunities and 19 distinct weaknesses within the NDMS (additional information on the opportunities and weaknesses that emerged from MCNIS have been reported elsewhere5,12). A plurality of 43% (n=23) of recommended interventions related to coordination, collaboration, and communication.
Attendees then participated in a facilitated discussion to provide context to their ranking decisions. Discussions focused on issues of coordination, collaboration, and communication. Attendees reached consensus that the prevalence of interventions related to coordination, collaboration, and communication was due to the need for improved collaboration across military, federal interagency, and civilian NDMS hospital partners, especially regarding bed status reporting, patient tracking, and care coordination. Discussions also focused on the importance of addressing staffing issues and building surge capacity within the NDMS, with distinctions made between the priorities of the private sector versus those of federal NDMS partners. Considering the MCNIS findings, meeting attendees recommended that NDMS Pilot implementation efforts should consider regional and sector-specific (ie, military, federal interagency, private sector) differences among NDMS partners. Attendees further suggested these differences would be best addressed through an overall federal management plan to coordinate the continuum of care across all NDMS partners. Altogether, this further foundational research revealed it was most critical for NDMS Pilot implementation activities to address the limited deliberate interactions within and across military and civilian stakeholders to prepare the NDMS for a large-scale medical surge scenario.
Implementation Planning: Year 1 Activities
NDMS Pilot Site Field Implementation Teams
Guided by the MCNIS findings and stakeholder feedback to approach NDMS improvements from a region-specific perspective, NDMS Pilot leadership prioritized securing local stakeholder endorsement of implementation activities. To achieve this, the NDMS Pilot created and staffed field implementation teams at each of the 5 sites. These teams aimed to (1) assemble coalitions of local leaders from healthcare, public health, and emergency management organizations; (2) refine and further develop site-specific opportunities for improving the NDMS; and (3) create operational plans that would address these site-specific opportunities over the remaining 4 years of the NDMS Pilot.
The next goal of the field implementation teams was to elicit qualitative input from local NDMS partners on discrete opportunities to strengthen the NDMS patient movement and definitive care capabilities, capacities, and interoperability at each site. At the beginning of Year 1, a survey was administered to assess each site’s baseline ability to handle a large-scale combat casualty surge. Survey participants included public and private sector NDMS stakeholders from each of the 5 sites. Specific capabilities addressed in surveys included connections to regional FCCs and healthcare coalitions, load-balancing and patient distribution capacity, medical surge readiness, and COVID-19 experience. Discussion forums were then held at each site, using survey responses to guide high-priority topics for discussion. Forums were held over 16 days and included nearly 300 stakeholders representing healthcare, public health, emergency management, and other emergency support organizations (Table 1). The opportunities identified by these forums were then prioritized by local NDMS partners and subsequently formed the basis for site-specific implementation plans. Following these steps, tabletop exercises were conducted at each NDMS Pilot site during the summer of 2022 to refine and validate opportunities and to identify additional operational issues relevant to the NDMS (Table 2). In total, over 240 participants across each region’s local public and private sectors took part in these exercises.
Participants in the Year 1 NDMS Pilot Site Peer Discussion Forums
aNumbers of participants are estimations as some of the forums were conducted virtually and attendance varied over the course of these multiday events.
Abbreviations: DOD, US Department of Defense; FCC, Federal Coordinating Center; HHS, US Department of Health and Human Services; NDMS, National Disaster Medical System; VA, US Department of Veterans Affairs.
Summary of the NDMS Pilot Year 1 Tabletop Exercises
Abbreviations: DOD, US Department of Defense; NDMS, National Disaster Medical System; TTX, tabletop exercise.
Site-Specific and Master Implementation Plans
Input from these forums were then prioritized by local NDMS partners and used to create 5 site-specific implementation plans. Each site implementation plan identified key opportunities that had the potential to enhance site-specific medical surge capacity, capability, and military–civilian interoperability. The 5 site-specific implementation plans contained a total of 95 opportunities prioritized by local stakeholders based on their importance and necessity at each respective site. The site implementation plans also included in-depth analyses of each site’s existing military and civilian healthcare landscape and important operational complexities that could impact implementation activities. These plans further defined steps for translating 20 of the highest-priority opportunities into distinct site-specific projects that would be prepared for immediate implementation by the NDMS Pilot’s field implementation teams (Table 3).
Twenty Prioritized Projects Identified in the Site Implementation Plans Conducted as Part of the NDMS Pilot Year 1 Activities
Abbreviations: FCC, Federal Coordinating Center; JPATS, Joint Patient Assessment and Tracking System; NDMS, National Disaster Medical System.
In addition, the NDMS Pilot developed a cross-site master implementation plan of strategic, national-level NDMS opportunities to enhance coordination and collaboration between the DOD and its federal, state, regional, and local partners. The plan identified several focus areas for improvement, which represented actionable opportunities and activities that the NDMS Pilot, in collaboration with state, regional, and local stakeholders, would be capable of executing in Year 2 and beyond. The 7 focus areas for improvement were: (1) staffing, (2) emergency medical services capacity, (3) regional patient regulation, (4) local–state integration, (5) training and education, (6) economic modeling, and (7) postacute care inclusion.
Peer-Reviewed Research: COVID-19 Surge Capacity Management
A chief concern identified from the NDMS Pilot’s foundational research was the NDMS’s inability to generate surge capacity in response to a large-scale combat operation. The COVID-19 pandemic provided an unprecedented opportunity for the NDMS Pilot to conduct more targeted research as part of its implementation activities to identify, analyze, and learn the strategies that NDMS-partnering healthcare facilities employed to increase their medical surge operations during an active public health emergency. To this end, the NDMS Pilot included questions in the Year 1 discussion forums to identify important innovations developed and executed by NDMS Pilot site hospitals to respond to patient surges during the first 2 years of the COVID-19 pandemic. Responses were coded based on a modified version of the 4-S framework of surge capacity (staff, stuff, space, systems) developed by Barbisch and Koenig 14 to categorize how hospitals managed patient surges. A total of 32 notable practices for managing COVID-19 surge capacity at the NDMS Pilot sites were identified. As reported elsewhere, 66% of the identified surge management practices primarily concerned innovations to surge capacity systems, and systems and staff were the only surge capacity domains referenced in at least 1 notable practice identified at all 5 NDMS Pilot sites. 15 This analysis gave insight into the empirical feasibility of suggested interventions for improving NDMS surge capacity. Additionally, it provided contextually relevant information on the operational capabilities of NDMS Pilot sites during real-world surge events.
NDMS Medical Surge Bed Capacity Estimation
To better characterize the surge capacity of the NDMS definitive care network, in Year 1 the NDMS Pilot began the process of developing a bed capacity estimator tool to quantify the baseline number and types of beds that would be available for use in NDMS hospitals during a large-scale combat-based medical surge scenario. To construct the tool, data were collected on the types of combat casualties traditionally sustained in battle based on statistics of injury occurrence in recent large-scale combat operations. 16 Specific parameters applied to the definitive care network included injury causality categories, further defined by required bed type, expected average occupancy days, and required clinical specialties. Data on facility metrics from the American Hospital Association and the US Department of Health and Human Services Administration for Strategic Preparedness and Response were used to determine which beds would be available at each site and the expected length of time the site could support a sustained surge of patients. In total, patients were segmented into 16 injury causality categories, of which 67% represented wounds sustained in combat action (eg, intracranial, burns, amputations) and the remaining 33% included both chronic and acute diseases and nonbattle injuries (eg, motor vehicle accident). 17
The tool estimates usable beds, which are defined as beds that are both appropriately licensed and staffed for use, while also employed for a definitive care function (see Table 4 for full definitions). This term was used in lieu of available beds to account for the reality that the majority of beds would be occupied at any given time by the local civilian population; therefore, while functionally usable, they would not necessarily be available for incoming casualties from a large-scale combat operation.
Bed Capacity Across the NDMS Definitive Care Network
Note: Most of the findings summarized in this table were originally presented at the 2022 Military Health System Research Symposium 19 in Kissimmee, Florida and at the 2023 Preparedness Summit 20 in Atlanta, Georgia.
aThe 5 Pilot sites are Denver, Colorado; Omaha, Nebraska; Sacramento, California; San Antonio, Texas; and the greater Washington, DC, metropolitan area (National Capital Region).
bIncludes only commercial hospitals and excludes children’s hospitals across the 5 NDMS Pilot sites.
Abbreviation: NDMS, National Disaster Medical System.
Preliminary results suggest that of the usable beds available within the NDMS, when accounting for standard public hospital occupancy rates of 90% to 95% during peacetime conditions, there would likely be a substantial gap in the NDMS’s capacity to meet the healthcare requirements of providing definitive care in the NDMS Pilot’s combat-based scenario (Table 4).18-21 This suggests that strategies to make additional beds available, such as early discharge through reverse triage measures, canceling elective procedures, or novel capacity-expansion methods, may be an integral component of ensuring the nation’s healthcare infrastructure can adequately provide care during a large-scale combat operation. As an initial effort to project hospital bed availability during the NDMS Pilot Program scenario, further work will be conducted to validate the bed capacity estimator tool and construct an enhanced model to more effectively regulate patients (ie, to arrange for the movement of patients through the roles of care and to match patients to a facility with the appropriate capabilities and bed space 22 ) at NDMS Pilot sites.
Implementation Execution: Year 2 Activities
Site-Specific Innovation Projects
In October 2022, 20 of the highest-priority innovation projects detailed in the site implementation plans were approved for execution by the NDMS Pilot field implementation teams as part of the initiation of Year 2 activities (Table 3). Although projects varied by location, all were designed to increase medical surge capacity within the specific NDMS Pilot site area. Furthermore, a funded solicitation for innovative project proposals was distributed to civilian healthcare and private sector NDMS partners. The aim was to promote locally led and tested NDMS innovations that address the master implementation plan’s 7 focus areas. By June 2023, selected proposals were awarded. As of April 2024, approximately 20 of these partner-led innovation projects were being conducted at their respective sites. Similar to the field implementation team-led projects, stakeholder-led projects vary by site and address operationally relevant topics specific to their local needs. Notably, site partner-led projects addressing issues of regional patient regulation and postacute care integration were approved for initiation at all 5 NDMS Pilot sites.
NDMS Targeted Studies: Health IT Systems and Participation Incentives
In Year 2, the NDMS Pilot pursued further targeted research aimed at informing strategic change across the NDMS. The MCNIS revealed that nonfederal civilian healthcare organizations had limited understanding of the incentives behind participation in the NDMS. Additionally, stakeholders had ongoing concerns about the sufficiency of existing electronic information-sharing systems for first respondents and emergency managers to coordinate with healthcare providers during large-scale medical surge events. The NDMS Pilot’s Year 1 implementation work further exposed the limited understanding many NDMS stakeholders have of the capabilities of existing information technology (IT) systems currently used in the United States for healthcare information sharing and coordination among multiple service sectors. 23 Consequently, Year 2 efforts involved the pursuit of several interconnected research studies to identify incentives for NDMS participation and improve the technological capabilities and interoperability of the IT systems used in the US healthcare industry during nationwide medical surge events.
As reported elsewhere, 23 the NDMS Pilot conducted a comprehensive landscape analysis of the health IT systems that would be used by the US government, state and local emergency management agencies, and hospitals and healthcare organizations during a full-scale, nationwide NDMS activation. This operational analysis assessed the feasibility of using these systems and their interoperability with other health IT systems, identifying both barriers and opportunities of each for improving regional healthcare information sharing during a large-scale medical surge event. 23 In addition, the NDMS Pilot began collaborations with the US government and local NDMS Pilot site stakeholders to develop a comprehensive NDMS health IT system concept of operations. This plan defines a shared vision in which the NDMS of the future employs an integrated network of health IT systems to efficiently track patient movement, record treatment of military patients, and accurately inform healthcare capacity and capability requirements. Finally, the NDMS Pilot began conducting an ongoing study on the requirements for a comprehensive NDMS health IT system that integrates relevant federal, regional, and local IT systems to support patient management, regulation, and tracking from point of injury to final disposition for a military patient wounded in an overseas conflict.
In addition to research on IT systems, the NDMS Pilot completed an analysis of the financial and nonfinancial incentives for civilian healthcare organization participation in the NDMS. Increasing civilian incentives is critical for the sustainability of the NDMS. Successful recruitment and retention of civilian healthcare organizations into the definitive care system build the requisite capacity needed to respond to a large-scale combat operation. Therefore, this research effort identified opportunities to enhance support incentives. This was accomplished through an extensive literature review, community of interest surveys, and subject matter expert interviews. The study team articulated a framework that identified 4 categories of incentives: financial, operational, legal, and intangible incentives. Within this framework, 42 specific recommendations for incentivizing NDMS participation were identified and ranked using a scoring matrix for suitability, feasibility, and acceptability. The highest-ranked support incentive was for awards or special designations to be provided to NDMS participants in public-facing events and communications.
NDMS Pilot Evaluation
Beginning in Year 2, the NDMS Pilot initiated an ongoing evaluation plan, designed to encompass all 5 years of the NDMS Pilot activities. The evaluation uses a mixed methods, preresearch and postresearch design to triangulate multiple data sources assessing the change in capacity, capability, and interoperability for an NDMS activation at each of the 5 NDMS Pilot sites. Surveys aimed at assessing progress toward the NDMS Pilot’s overall objectives were distributed to participants at each site in August 2023 during an additional NDMS Pilot tabletop exercise focused on increasing stakeholder understanding of their roles and responsibilities as part of the NDMS. Surveys were followed by focus groups with a purposive sample of NDMS stakeholders. This approach will provide a foundational assessment of the NDMS Pilot’s contributions to NDMS readiness at the sites and, thus, the overall effectiveness of the NDMS Pilot. Furthermore, the evaluation plan will monitor progress in individual NDMS Pilot site innovation projects to assess which can be recommended for broader adoption throughout the NDMS.
Discussion
Overall, the goal of the NDMS Pilot is to produce more effective, scalable, and interoperable solutions that can transform nationwide medical surge capability in the United States. While the need for improving the NDMS has been recognized for decades,3,24 additional efforts are needed to ensure the system will be operationally effective at scale. The NDMS Pilot’s formative research and early implementation activities have identified multiple ways to increase healthcare capabilities and capacities to more effectively respond to a large-scale surge of combat casualties returning from an overseas conflict. The NDMS Pilot represents a comprehensive and concrete effort to bring about meaningful system change.
The primary limitation of the NDMS Pilot’s early implementation efforts was that many findings were produced using operational research methods and design (eg, facilitated discussion, purposive sampling, qualitative analysis), constraining the ability to contribute to generalizable knowledge and program-level assessments. Despite this constraint, operational research techniques are ideal for efficient organizational decisionmaking and enabling contextually relevant improvements to be applied to the NDMS. As previously mentioned, the NDMS Pilot’s work in the coming years will address this gap by using program evaluation methods to more systematically examine the effectiveness and efficiency of suggested improvements.
Looking forward to its final 3 years, the NDMS Pilot will further execute implementation plans, iteratively test and measure the effectiveness of interventions, and conduct further targeted research that addresses system-wide improvements. The third and final expansion phase of the NDMS Pilot will aim to scale effective local projects as potential site-agnostic solutions for nationwide implementation. The NDMS Pilot will culminate in a final report of recommendations to Congress on expanding and making permanent the program’s achievements.
Conclusion
Strengthening military–civilian partnerships, which form the backbone of the NDMS, is essential for meeting the healthcare needs of casualties from large-scale wars or other catastrophes. It also increases the broader US healthcare system’s preparedness and resiliency for a variety of large-scale surge events. In the current international geopolitical environment, systems-wide improvements in coordinating patient movement and medical surge capabilities in the United States enhance the national security of the country and its allies. Ultimately, however, the true value of improving the NDMS is ensuring wounded US service members can receive the medical care they both expect and deserve.
Footnotes
Acknowledgments
The authors thank Ashley Peck, MPS, Gabriela Paszt, MPH, Victoria L. Klimczak, BS, William “Wills” L. Sizemore, MS, LTC USA (Retired), Michael Klemann, MHA, MPS, CDR MSC USN, Christopher C. Brown, Capt USN (Retired), Booz Allen Hamilton, and the NDMS Pilot Program field implementation teams from Deloitte Consulting LLP and the University of Nebraska Medical Center for their contributions in producing the source materials on which this work is based; Nicholas V. Cagliuso, Sr., PhD, MPH, and Kimberly B. Gill, PhD, for their scientific contributions to the design, execution, analysis, and interpretation of much of the research activities underlying this work; and Reena Sethi, DrPH, MHS, and Audrey Hurley, MBA, for their administrative and logistical support in the preparation of this work.
Funding for the project was provided by the Office of the Assistant Secretary of Defense for Health Affairs (Award No. HU00012120098) and administered by the Uniformed Services University of the Health Sciences (USUHS). This project is sponsored by USUHS; however, the information or the content and conclusions reported in this work do not necessarily represent the official position or policy of, nor should any official endorsement be inferred on the part of, USUHS, the US Department of Defense, the US government, or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc.