
Abstract
In response to the growing number of outbreaks of emerging infectious diseases, the US Administration for Strategic Preparedness and Response (ASPR) has embarked on a plan to improve and expand special pathogen patient care capabilities. To achieve this, ASPR is developing a coordinated network of Regional Emerging Special Pathogen Treatment Centers (RESPTCs) to serve as state-of-the-art facilities staffed by a highly trained workforce to care for and manage special pathogen patients across the lifespan. The RESPTC network represents the operational arm of a broader US National Special Pathogen System of care to prevent and prepare for the next infectious disease outbreak. RESPTCs are strategically located in every region across the country and form a network linking local and regional healthcare partners to enhance national preparedness through training in best practices for detection, isolation, and treatment of individuals suspected of or known to be infected with a special pathogen. This local, regional, and national network is also designed to lead a coordinated response that includes the dissemination of accurate and trustworthy information to responders and the public. The overarching goal of the RESPTCs is to serve as a valuable resource for clinical care, training, and material support to meet current and future major infectious diseases challenges. In this case study, 2 new RESPTCs, MedStar Washington Hospital Center and the University of North Carolina, describe their experiences related to designing a biocontainment unit, creating clinical teams, building staff resiliency, receiving mentoring from regional RESPTC partners, and developing opportunities for innovation.
Introduction
I
Unit Design and Location
Space is a critical consideration related to the safe care of patients with special pathogens. A number of existing RESPTCs have standalone BCUs that are used only during the care of a special pathogen patient. Both MWHC and UNC have developed dual use space for daily patient care, along with key features that allow them to be converted during an activation to enable the safe care of special pathogen patients.
MedStar Washington Hospital Center and MedStar Health
Starting in 2014 with the West Africa Ebola outbreak, MWHC became a designated treatment center for special pathogens serving the District of Columbia and Maryland. Upon activation for a patient with a special pathogen, care space was created by converting one-third of the emergency department (ED) into a separate standalone unit. Following the experience of multiple activations resulting in significant reduction in ED capacity, the hospital and health system leadership prioritized creating a designated unit for special pathogen care (Figure 1). In designing the unit, the MedStar Health team leaned on the advice and experience of existing BCU programs and an outside architecture firm with prior BCU project experience to design a new purpose-built unit.
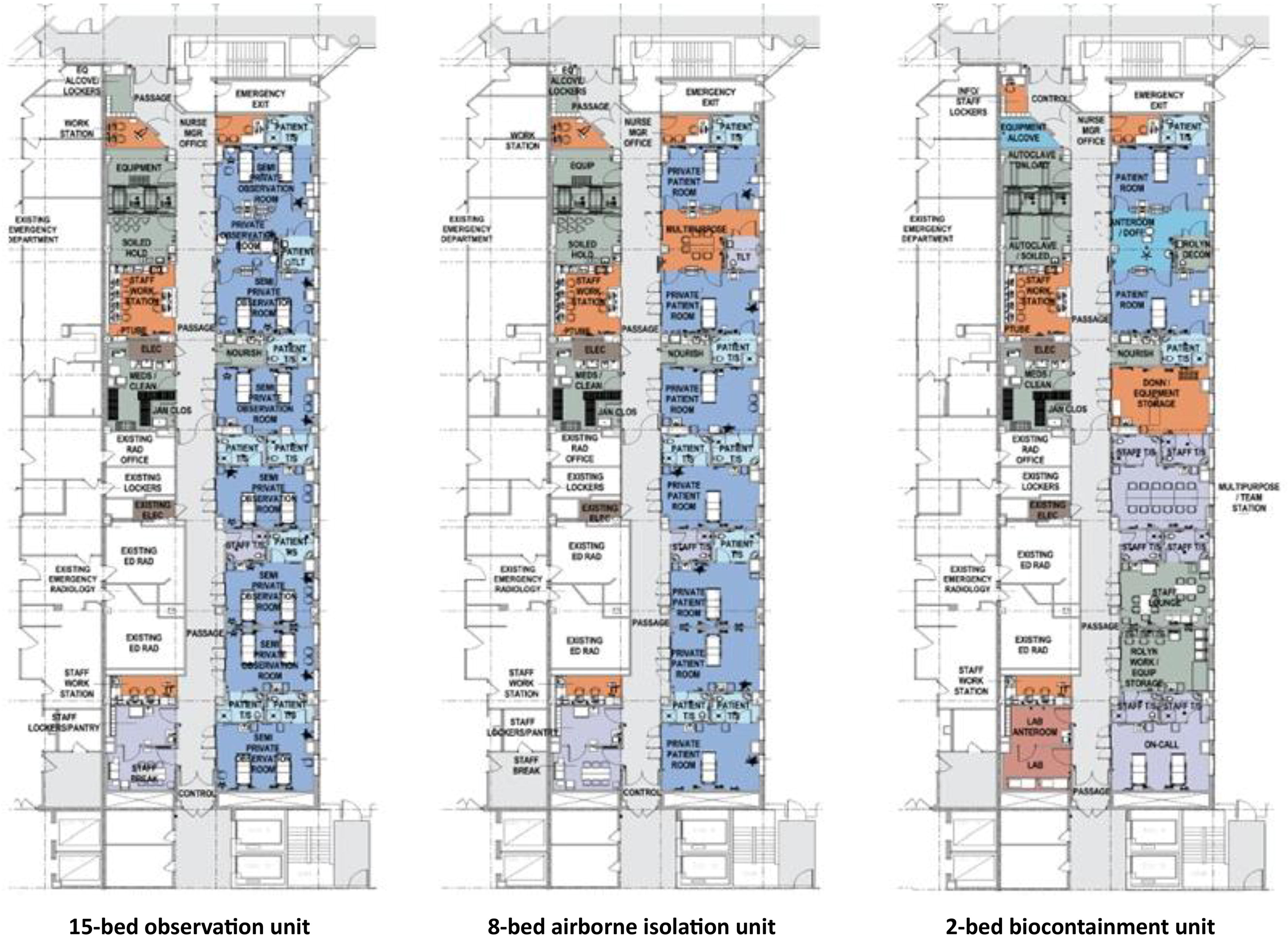
MedStar Health Biocontainment Unit.
The 6,800-square-foot negative pressure BCU is located on the first floor of the hospital and is adjacent to the ED and trauma unit. This location allows for more direct access to the unit from designated entrances in the trauma unit and the ED, and for direct patient arrival via emergency medical services transport or from the ED without the need to travel longer distances through public areas of the hospital. The unit is structured to function in 3 modes of care: 15-bed patient observation unit, 8-bed airborne isolation unit, and 2-bed patient BCU.
During routine use, the unit serves as an ED observation unit for moderate to low-acuity patients who require treatment or additional testing but are expected to be discharged within 24 hours from the hospital. Keeping the unit in daily use allows for routine maintenance of the unit’s equipment and facilities. During an activation, new admissions are stopped for the observation unit and existing patients are relocated to alternative units or discharged if their care needs have been met.
If the unit is faced with a surge of respiratory illness patients requiring negative pressure isolation, the 8 rooms (7 with 2-bed capacity and 1 with single-bed capacity) can accommodate 8 or 15 patients (for a respiratory viral pathogen, we would cohort 2 to each 2-bed capacity room). All patient care rooms are negative pressure equipped with a dedicated heating, ventilation, and air conditioning system and a high efficiency particulate air (HEPA) filtration system.
During an activation for a special pathogen patient requiring full precautions, the unit can accommodate 2 patients in individual rooms with a shared anteroom between the 2 rooms. These patient care rooms have a negative pressure pass-through window with HEPA filtration, private bathrooms, 2 additional doors into the patient room to allow for a separate entrance and exit for unidirectional flow, and fully transparent glass doors that allow for safe observation of patient care. They are equipped to provide the full spectrum of intensive care interventions and have operating room and labor and delivery capabilities. The remaining rooms on the unit are converted to meet designated special pathogen care needs to include a donning room, equipment storage, staff conference room, staff lounge, and vendor support room. Cameras in the special pathogen rooms and anteroom provide a live feed to the adjacent staff workstation.
The unit includes the added feature of its own laboratory with 2 hoods and an anteroom for laboratory staff doffing, 2 autoclaves for waste management, and a visitor waiting space. Access to the unit is controlled electronically upon BCU activation to limit traffic to essential team personnel only.
While there are benefits to the unit being in use on a routine basis, there are also challenges that come with relocating the ED observation patients to other units during an activation. The routine use of the unit for ED observation provides much-needed hospital capacity and reduces ED boarding times by allowing for rapid patient disposition. By halting this service line to activate the BCU, hospital capacity decreases and ED patients may experience increased boarding time. While the ED observation unit was made possible by the creation of the BCU, hospital operations are now positively impacted by the routine use of the unit, which must be weighed against the needs of the BCU. Since this impacts the availability of the unit for BCU training purposes, the ED observation unit team and BCU team work collaboratively to schedule unit-specific training at times that have the least impact on routine patient care.
The University of North Carolina
The UNC special pathogen care unit (Figure 2) was designed by incorporating key principles of biosecurity into existing clinical care spaces to make them pluripotential (ie, capable of dual use) and thus able to care for special pathogen patients while maintaining routine healthcare delivery concurrently. This design incorporated 3 key lessons learned from responses to emerging special pathogen outbreaks and caring for patients with SARS-CoV-1, Ebola virus disease, Lassa fever, and SARS-CoV-2: (1) supportive care is the foundation of care for all severe infections and delays between symptom onset and care increase mortality2,3; (2) special pathogen treatment units with enhanced infection control integrated into existing healthcare infrastructures ensures access to the full complement of care available at a quaternary care hospital, enables the ability to scale up quickly, and improves infection control throughout the hospital; and (3) scalability is critical for both suspect and confirmed patients. As a result, UNC Medical Center (UNCMC) created a special pathogen care plan incorporating preparedness into daily clinical care. This enables safe special pathogen patient care in an existing clinical space, which can be effectively separated from routine care and can be increased or decreased in size depending on the needs of the outbreak and the hospital. By adding negative pressure capacity (with HEPA-filtered, externally exhausted air) to an additional 4 contiguous medical intensive care unit (MICU) beds, the capacity to care for patients who require aerosol isolation, including special pathogen patients, expands to 10 beds in the same unit. The use of portable walls, modeled after those built by Massachusetts General Hospital’s
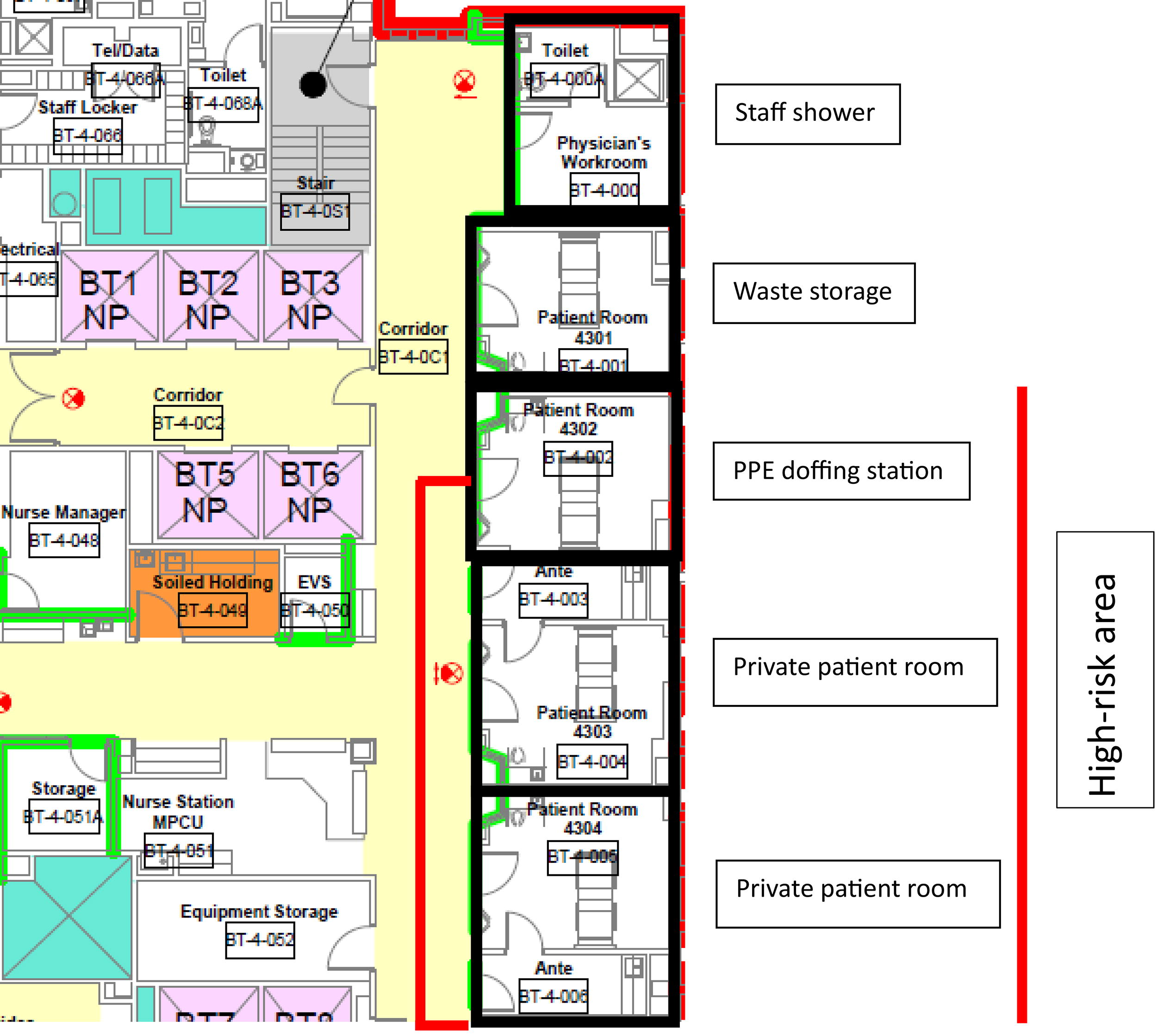
University of North Carolina Medical Center Special Pathogen Care Unit. Abbreviation: PPE, personal protective equipment.
The 4 rooms with designated beds for special pathogen patients are outfitted with telecommunications capabilities to facilitate virtual care and close patient monitoring. These rooms will be used as regular negative pressure rooms for the MICU when the Special pathogen patients have access to the same level of care as routine patients including the full complement of subspeciality expertise such as pulmonary and critical care medicine, infectious diseases, nephrology, obstetrics and gynecology for pregnant persons, surgery, and psychiatry for wellness support across the entire life spectrum. Clinical space can be quickly transformed from routine health service delivery to a high-containment space; either can be scaled up or down depending on patient care needs. Providers on the special pathogen care team are familiar with the space and location of resources. This model is replicable and can be extended to additional clinical areas in response to a surge of special pathogen patients that outstrips a traditional 2- or 4-bed BCU capacity. In contrast to a separate unit dedicated only to special pathogen patients, an integrated unit can benefit from economies of scale, including the benefits of materials as well as personnel who can respond to high- and low-risk patients when needed. Units dedicated for special pathogen patients could be challenging to establish and sustain in hospitals that seek to generate revenue from all available space.
Key activities supporting patient care are done within or adjacent to the MICU. Donning is conducted at the single entrance between the low- and high-risk zones under the supervision of personnel trained in infection prevention and control. 4 Movement of staff incorporates a unidirectional flow moving from suspect to confirmed special pathogen patients. Doffing, one of the highest-risk activities performed by staff caring for such patients, occurs in a separate negative pressure room under the supervision of trained personnel. 5 The special pathogen laboratory is located in 2 airborne isolation rooms with HEPA-filtered, externally exhausted air, separate from the MICU, and contains 2 A2 biosafety hoods for the safe processing and testing of samples. Additionally, investment in the hospital’s existing waste management strategy includes the ability to decontaminate category A waste as well as routine regulated medical waste.
This integrated model of special pathogen care delivery has been implemented successfully. In response to the COVID-19 pandemic, UNC designed and implemented a flexible and rapid restructuring of a portion of the UNCMC MICU into a high-containment unit that allowed isolation of suspect and confirmed COVID-19 patients and incorporated key infection prevention principles including separate entrances and exits, monitored donning and doffing by personnel trained in infection prevention and control, unidirectional movement from suspect to confirmed patients, airborne isolation for patients, and safe movement of laboratory samples and waste. 6 The result was the provision of comprehensive care without nosocomial transmission to providers or other patients.
While intensive care providers are familiar with providing care in this space, a key challenge is limited access for training or renovation due to high demand for intensive care space in a busy quaternary care hospital. Staffing can help mitigate this challenge by ensuring that intensive care providers who work in this space daily are recruited to the special pathogen response team and at least 1 provider is scheduled for each shift. However, renovations require shutting down the room for patient care for the duration of the renovation. Additionally, careful consideration must be given to patient transportation to, and movement of category A waste out of, the special care unit without environmental contamination or nosocomial transmission.
Staffing Model Approach
In addition to designing a safe space for special pathogen care, staffing also needs to be considered, along with stuff (equipment and supplies) and systems (strategy of care). The challenge is to merge specialty clinical expertise with rigorous infection prevention training in a coordinated fashion to ensure safe clinical care from admission to discharge for all patients.
MedStar Washington Hospital Center and MedStar Health
Leadership Team Model
The BCU at MWHC is a part of the hospital’s Institute for Public Health and Emergency Readiness, which has direct lines of communication with senior hospital leadership, reflecting how the hospital and the larger health system, MedStar Health, have prioritized the BCU program. This support from senior leadership of our health system had been a key component of and vital to our program’s success. The BCU leadership team consists of the medical director for the BCU who directly oversees the BCU program director, associate medical directors, and Children’s National Hospital site director (Figure 3). The nursing operations/training and education coordinator and the administrative coordinator report to the BCU program director, while specialty lead clinicians from key clinical departments report to the medical director through the associate medical directors.
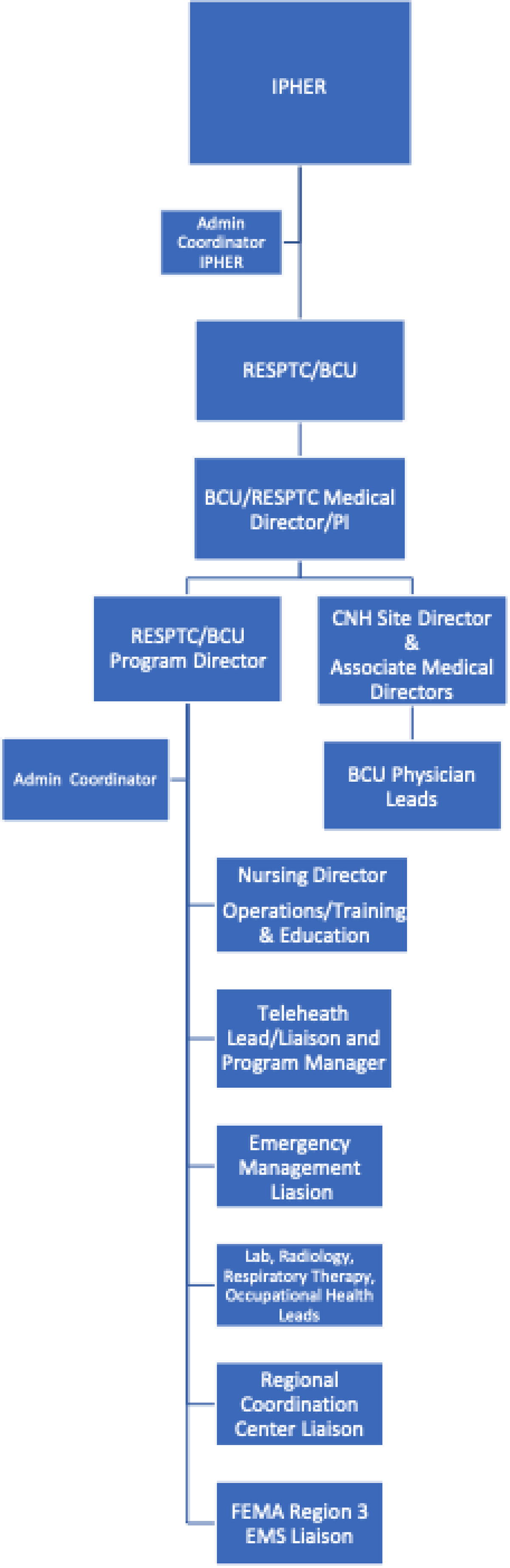
MedStar Washington Hospital Center Biocontainment Unit leadership structure. Abbreviations: BCU, biocontainment unit; CNH, Children’s National Hospital; EMS, emergency medical services; FEMA, US Federal Emergency Management Agency; IPHER, Institute for Public Health Emergency Readiness; PI, principal investigator; RESPTC, Regional Emerging Special Pathogen Treatment Center.
While the clinician team is coordinated primarily by the medical director pillar and ancillary services are managed by the program director pillar, there is significant emphasis on cross-disciplinary collaboration and teamwork. Our operational model includes multiple committees and workgroups to organize and direct efforts.
Clinical Staffing
Because critical care intensivists are capable of caring for patients across the spectrum of acuity levels, a team of critical care physicians and advance practice providers comprise the primary MWHC BCU care team. This team consists of 15 critical care attending physicians and 15 critical care advance practice providers specially trained in BCU protocols and care to ensure 24-hour staffing with minimal notice. Strategic service lines that are considered essential to the care of a special pathogen patient were also identified: general surgery, obstetrics and gynecology, neonatology, infectious disease, anesthesia, and emergency medicine. Each of the strategic specialties has a lead clinician with dedicated full-time equivalent (FTE) support; in turn, they are responsible for their service line’s readiness by determining the number of staff who need to be trained, recruiting staff in their service line, and creating protocols related to their specialty as it pertains to special pathogen care. The lead clinicians weigh the on-call needs of each specialty and the likelihood of emergent patient care needs for that specialty to determine the target number of clinicians to be trained. For the critical care primary team, there are 4 lead clinicians to manage the primary team, on-call schedules, activation plan, scheduling in an activation, and creation of clinical plans to include supplies needed, clinical guidance documents, and care plans. As an adult care facility, MWHC has partnered with Children’s National Hospital for pediatric special pathogens care, which resulted in the creation of a pediatric team consisting of hospitalist, intensivist, and infectious disease clinicians at their institution.
Nursing Staffing
As with all MWHC BCU staff, nurses join the team on a voluntary basis. Nurses are recruited from numerous departments and service lines throughout the hospital, with the majority (16 of 21) coming from the critical care division. Similar to how physicians and advanced practice provider team members are recruited, nurses are also recruited from the critical care division by design to ensure adequate nursing staff to care for special pathogen patients who require all levels of care. Additionally, the care team includes 3 mother/baby nurses and 2 hemodialysis nurses. Year-round recruiting is an administrative priority.
Upon activation, nurses are reassigned from their primary units to work in the BCU. The staffing matrix for nurses in the BCU requires 4 to 12 nurses per shift depending on patient acuity. Decisions on staffing are assessed continuously and adjusted as needed to meet patient care needs.
Ancillary Staffing
In addition to the nursing and clinician team members, the BCU has trained and rostered team members from MedStar transportation, laboratory, respiratory therapy, and radiology, for a total of 112 team members trained in donning and doffing of personal protective equipment (PPE). Team members also include personnel from the ethics department, occupational health, infection prevention, telehealth, and sterile processing.
The University of North Carolina
Leadership Team Model
The UNC Special Pathogen Response Center (SPARC) team represents a collaboration between UNC’s Institute for Global Health and Infectious Disease and UNCMC. The team is led by 2
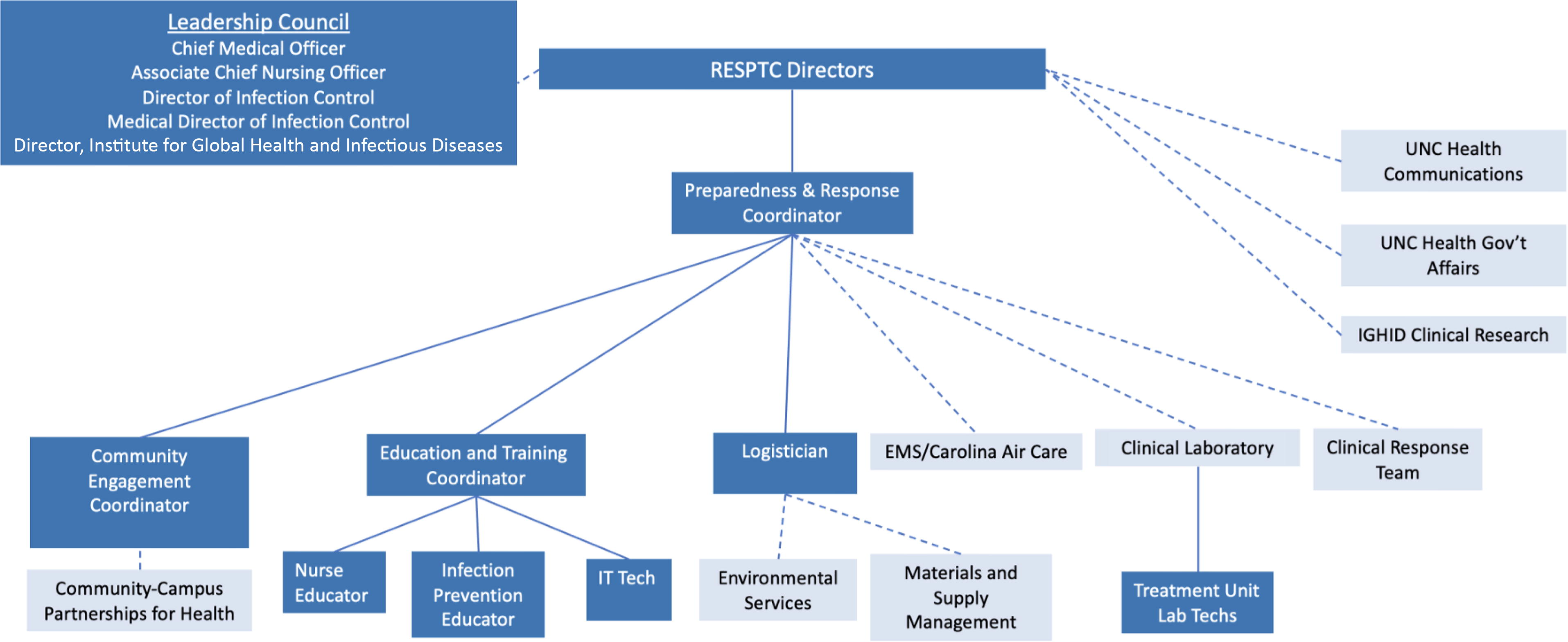
The University of North Carolina at Chapel Hill RESPTC leadership structure. Abbreviations: EMS, emergency medical services; IGHID, Institute for Global Health and Infectious Diseases; IT, information technology; RESPTC, Regional Emerging Special Pathogen Treatment Center; UNC, University of North Carolina.
Clinical Staffing
To ensure the ability to provide the same clinical care for all patients with special pathogens, UNC has created a SPARC team composed of nurses, advance practice providers, and physicians from adult and pediatric inpatient units with subspecialty expertise in critical care, emergency medicine, infectious diseases, surgery, pediatrics, obstetrics and gynecology, and medical transport. These providers have been recruited as specialty teams including 2 physician co-leads with dedicated FTE support with 5 to 10 nurses per specialty. This approach achieves 3 important goals: the recruitment of staff with diverse clinical skills; the ability of specialty teams to develop specialty-specific standard operating procedures; and the avoidance of exhausting any clinical area upon activation. The first 2 goals ensure that special pathogens patients receive the same care as nonspecial pathogen patients, and that the delivery of that care occurs in an enhanced infection prevention and control environment. The latter goal reflects the staff-intensive nature of special pathogen care and ensures that the delivery of care does not interfere with the care provided to nonspecial pathogen patients.
The UNC staffing model will be, in large part, dependent on patient acuity; however, any activation will require a staffing minimum to support direct patient care, infection prevention and control support and monitoring, logistics support, communications, security, and emergency operations oversight. Upon activation, nurses would be assigned to the UNC Special Pathogen Treatment Unit for 1 week at a time. At a minimum, 3 nurses, 1 physician, and 1 advance practice provider will be activated to provide care for 1 patient during a 12-hour segment. This expanded ratio of providers to patients is a direct response to address the increased work-related stress associated with special pathogen care, the restrictive nature of PPE, and roles and responsibilities in both the high- and low-risk zones with limited mobility between them.
Promoting Staff Resiliency and Retention
MedStar Washington Hospital Center and MedStar Health
As a health system that treated some of the largest numbers of COVID patients in the region throughout the COVID-19 pandemic and now as a
At the forefront of MedStar Health’s programmatic development is the mantra of staff safety as the highest priority in the mission. This manifests in constant attention to identifying safety risks, PPE breeches, and rethinking processes to address safety. In creating a culture of safety, the MWHC BCU leadership consistently seeks feedback from staff after each training session in the form of an in-person debrief and follow-up evaluations. Additional platforms for sharing feedback include a biannual survey and frequent personal check-ins with the team to address concerns as they arise. The goal is for staff to feel valued and that their safety is a priority for the program.
Creating a team dynamic through personal connection with team members is an essential tenet to the MWHC teambuilding process. Group training sessions are designed for 8 to 15 staff members to ensure they are small enough for individuals to get to know each other and large enough to expose staff to their fellow team members. Training sessions are designed for cross-disciplinary interaction.
Instilling a sense of pride in the team by emphasizing a higher purpose and highlighting the unique group they have created further cultivates team cohesion. Engaging team members to share their creativity and ideas while building care plans and protocols further demonstrates that the program values their expertise and dedication to the project. Lead clinicians are given specific clinical scenarios and are asked to lend their domain-specific expertise to answer these special pathogen-related clinical questions. This engagement creates better informed protocols while fostering dedicated staff. Personal connection remains the top recruitment strategy for the team.
Other practical strategies that support staff retention include flexibility in training opportunities (eg, multiple dates and times and levels of involvement), monetary compensation and continuing medical education credit for training participation, compensation for the lead clinicians with salary offset support, provision of branded uniform materials in the form of jackets and head coverings, and hosted team social events to allow staff to connect with team members outside of training sessions.
The University of North Carolina
Over the past decade, much has been learned about moral injury in the course of medical care, particularly during the care of emerging or high-consequence infectious diseases in public health emergencies. Deployments of healthcare workers to outbreaks are rarely followed by a “check-in” to ensure the individual is coping with the stress following a response. The UNC team believes there is a better way—which begins with prevention rather than response and focuses on building resiliency and wellness before an outbreak.
The COVID-19 pandemic has made evident that working in a high-risk, high-stress environment takes a toll on healthcare providers, leading to increased rates of distress and burnout.
7
Importantly, UNC Health leaders recognized that pandemic-related stressors impacted not only frontline healthcare workers treating patients with COVID-19, but also employees across the entire health system. The system response was designed to address the needs of employees with both direct and indirect exposure to patients (ie, clinicians and support personnel). Building on earlier work, UNC has developed a multipronged approach to support healthcare workers, patients, and their families, which begins before an activation and continues after a special pathogen patient is discharged. Prior to an activation, efforts focus on preventive interventions to build resiliency and psychological preparedness and create a foundation for a trauma-informed workforce. During an activation, acute care resources are deployed including expanding mental health services to deliver trauma-informed stress first aid, establishing a support call-in hotline, and offering virtual interventions such as workshops, support groups, and webinars. For UNC’s
Collaboration With Established Highly Infectious Isolation Units
A mutual aim of enhancing overall regional readiness was launched through partnerships with established RESPTCs within each region, including the partnership between the Johns Hopkins BCU and MedStar Washington Hospital Center (MWHC) in HHS Region 3 and the partnership between Emory University Serious Communicable Diseases Program (SCDP) and the University of North Carolina at Chapel Hill in HHS Region 4.8,9
The Region 3 and Region 4
After the designation of the new RESPTCs in 2022, standing meetings were scheduled to bring together program counterparts from administrative, medical, nursing, operational, pediatric, and emergency medical services roles. These meetings serve as open forums to discuss internal
The Johns Hopkins BCU team welcomed MWHC into several established activities including the Special Pathogen Training and Education Program (STEP), which provides in-person workshops at frontline healthcare facilities. 10 This grassroots approach to special pathogens training and program development organically builds a network of preparedness stakeholders including infection control personnel, emergency management, and public health officials. By presenting a unified team across both RESPTCs in STEP, facilities have the ability to consult with experts who have a greater range of knowledge and experience. Similar to the partnership between the Johns Hopkins BCU and MWHC, the Emory SCDP invited UNC to participate in several preparedness activities, such as 1-day courses on special pathogens for hospital and emergency medical services held in each state across Region 4. These courses allow the Region 4 RESPTCs to collaborate with state health departments and provide training for frontline facility staff on special pathogens, infection prevention and control principles, the identify–isolate–inform mantra, PPE, and hands-on skill sessions.
Collaboration between RESPTCs has brought forth more than shared best practices and experiences; it has also capitalized on synergized efforts that demonstrate a collegial and beneficial approach to future
Opportunities for Innovation Within the Field
MedStar Washington Hospital Center and MedStar Health
Telemedicine
MedStar Health’s telemedicine program expanded significantly to accommodate patient needs during the COVID-19 pandemic. Talent and resources from the program were applied to the functionality of the BCU through the design of several avenues for telemedicine use in special pathogen care. MedStar Health has established an electronic PPE program, which relies on telemedicine tools to reduce direct bedside time for providers within the unit, enabling multiple and ongoing clinical assessments from our primary clinical team and consultants during a shift. Telemedicine is also being developed for the ED triage intake for persons under special pathogen investigation, which enables infectious disease experts to interview patients remotely during triage. The telehealth team is also designing a remote patient monitoring program that incorporates the spectrum of care including an at-home e-visit with expert consultation, home testing, and ongoing patient monitoring. This technology serves as a scalable resource for the community and region in the event of a larger outbreak by providing additional virtual surge capacity.
Ethics
The John J. Lynch, MD Center for Ethics is a dedicated ethics department at MWHC that is actively engaged and integrated into the MedStar Health's BCU team. An ethics consult is a standard component of and included in the initial admission orders placed for a patient in the BCU. The ethics team assists in navigating the complex patient scenarios where staff risk, resource allocation, appropriate treatment modalities, and patient care interventions must be carefully weighed for each unique patient presentation. Engaging the ethics team in the design of patient care protocols at the beginning of team development has been a priority. The ethics team is also working to address these important questions and considerations including the equitable use of crisis standards of care at national and international levels.
The University of North Carolina
Community Engagement
Recent outbreaks of Ebola virus disease, COVID-19, and mpox have revealed the importance of accurate public communication on public health measures. The effects of misinformation regarding mitigation strategies and medical countermeasures are most acute for those at a higher risk of infection and severe outcomes. Because pathogens of consequence are likely to emerge and reemerge, the period between responses is when strong ties can be established with key stakeholders who are seen as sources of truth and trusted as conduits for sharing accurate health information. A key initiative started by the UNC
Research
During special pathogen outbreaks, clinical research is essential to advance the understanding of clinical signs and symptoms to inform case definitions, disease epidemiology to understand transmission routes and identify those at highest risk of infection and worse outcomes, clinical complications of infection to improve supportive care approaches, and safety and efficacy of novel pathogen-specific vaccines and therapeutics to improve prevention and outcomes. Thus, a key opportunity for innovation is the establishment of a highly coordinated clinical research platform. Building on the platform established by the Special Pathogen Research Network, the UNC
Simulation
Leveraging the simulation programs of UNC and MedStar Health has augmented team training opportunities by transforming simple PPE donning and doffing sessions into advanced care scenarios. These simulation programs enable team members to practice tangible skills including adult resuscitation, central line insertion, airway management, perimortem C-section, maternal resuscitation, and neonatal resuscitation while in PPE. Such scenarios also allow for team building, delivery of multidisciplinary care, and communication practice while in PPE in high-fidelity environments akin to real-world activations. These simulation opportunities are a critical component of the quarterly training programs at both institutions.
Conclusion
In response to the growing threat of emerging high-consequence pathogens, and particularly the unprecedented global crisis caused by the COVID-19 pandemic, the US National Special Pathogen System was created to coordinate a more effective, equitable, and sustainable response. The operational arm of this effort includes the establishment of RESPTCs to provide direct patient care and strengthen regional preparedness to identify, isolate, and treat patients with special pathogens. Basic principles apply to establishing a new BCU, although complete uniformity is impractical across all BCUs due to institutional differences. Seeking mentorship and collaboration with existing BCUs has provided guidance on how to meet universal challenges. Approaching programmatic challenges by building on each program’s strengths and ensuring safety as the key principle has helped both new RESPTCs navigate the establishment of a new unit and program. Their experiences may serve to inform future new BCUs in finding their path.