
Abstract
Rwanda is a country in East Africa, a region characterized by highly mobile populations and outbreaks of high-consequence infectious diseases occurring on a regular basis. To increase the level of outbreak preparedness in the region, the Rwandan government and the German Ministry of Health signed a joint agreement to construct a new high-level isolation unit in Rwanda, the first in East Africa, and implement a training program for Rwandan healthcare workers to equip them with the necessary skills and knowledge for medical management of patients under high-level isolation conditions, including intensive care treatment. To better understand the scope and format of the planned training program, a needs assessment was performed based on findings from a standardized survey of 4 intensive care units in Rwanda as well as observations from 2 members of a German high-level isolation unit who completed clinical internships at Rwandan hospitals. In this case study, we describe the necessary steps to promote the sustainability and capabilities of the new high-level isolation unit in Kigali and ensure the successful implementation of the training program.
Introduction
R
High-consequence infectious diseases (HCIDs) pose significant risks for healthcare systems and public health safety (Table). Although no cases of HCIDs have been reported directly from Rwanda, the country is surrounded by recent outbreaks in its neighboring countries (Figure 1). The most recent outbreak of Ebola virus disease was reported in Uganda (Sudan strain) in September 2022. 7 In the DRC, the latest outbreak of Ebola virus disease (Zaire strain) was recorded in the months following April 2022, 8 making it the most recent in a string of 14 outbreaks since 1976. Marburg virus disease, which caused an outbreak in Tanzania in March 2023, 9 was responsible for 3 outbreaks in Uganda in 2012, 2014, and 2017 10 and 1 outbreak in the DRC in 1999. 11
List of High-Consequence Infectious Diseases 5
Abbreviation: HCID, high-consequence infectious disease.

Map of Rwanda and its neighboring countries with country-specific HCID risk. 6
These HCID outbreaks involved diseases generally classified as having high case fatality rates and limited or no specific treatment options, as well as posing a risk to contacts, healthcare workers, and the general population. Therefore, it was deemed necessary to equip the Rwandan healthcare system with the appropriate capability to treat such diseases as effectively and safely as possible.
Cooperation Between Germany and Rwanda
Because Rwanda is surrounded by countries with outbreaks of HCIDs and located in an area with heavy cross-border movement of people, the Rwandan government recognized the need to increase its level of public health preparedness. 12
In 2018, in response to the Ebola virus disease outbreak in the DRC, a series of train-the-trainer courses for infection prevention and control (IPC) began. The Efficiency by Edification (EFFO) project training program (EFFO-I), was implemented by the Robert Koch Institute (the federal public health institution of Germany) in cooperation with its Rwandan counterpart, the Rwanda Biomedical Center. 13 EFFO-I was followed by a project focusing on healthcare facilities (EFFO-HCF) in 2019, that had the task of constructing 2 units for temporary isolation of patients with HCIDs. The isolation facilities were originally planned for use as Ebola treatment centers, but in 2020, at the beginning of the pandemic, they were repurposed for the isolation of COVID-19 patients by the Rwandan government. 14
In October 2019, the ministers of health of Rwanda and Germany signed a joint declaration of intent outlining the intended collaboration between key public health institutions in both countries regarding the training of Rwandan healthcare workers in HCID management and the construction of the first high-level isolation unit (HLIU) in East Africa.
15
The new project, which created a center of excellence (EFFO-COE), was funded by the German Ministry of Health and started in November 2021. The project includes 2 main components:
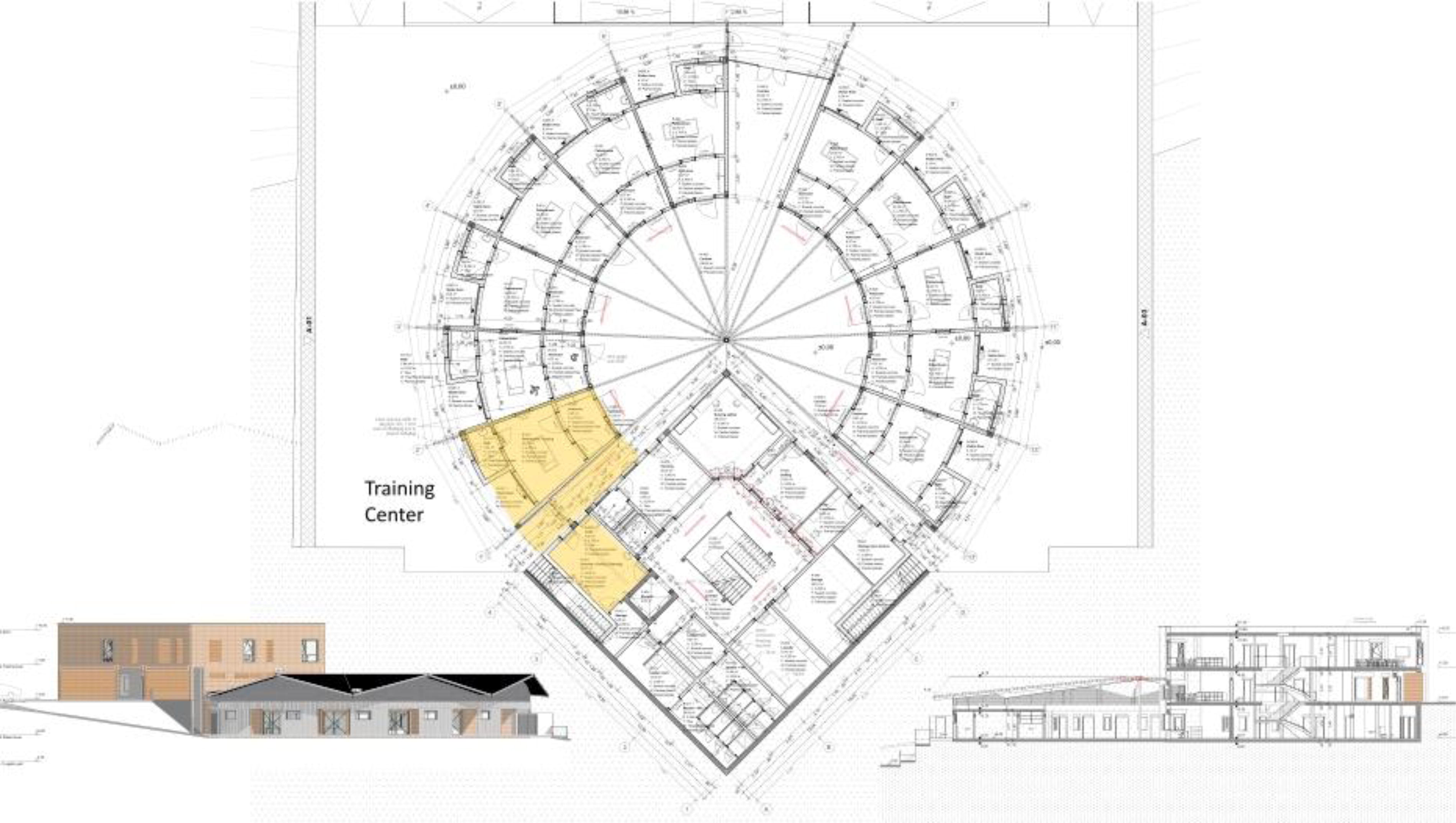
Architect’s drawing of the Kigali high-level isolation unit and training center.
The Rwanda National Action Plan for Health Security 2020-2024 16 primarily addresses the public health aspects of the International Health Regulations (2005) 17 and focuses on epidemic events, but it does not explicitly mention the project of establishing an HLIU. Nevertheless, when the construction of the HLIU has been completed and routine training in the medical management of HCID patients has been established, we expect the HLIU to serve as a key component of enhancing national preparedness through the training of healthcare workers. Since the project was agreed upon between Rwanda and Germany in 2019, it was not mentioned in the Rwanda Joint External Evaluation Assessment of 2018.
Planned Level of Care in HLIUetting
After the decision was made to build an HLIU in East Africa, plans for its capacity and treatment capabilities were considered, given that HCIDs carry a high risk of deterioration to severe illness with multisystem organ dysfunction. A major finding of the 2014-2016 Ebola virus disease outbreak in West Africa was the effectiveness of supportive intensive care during a time when no proven virus-specific treatment was available. The case fatality rate of patients who were medically evacuated to HLIU in Europe and North America was 20% 18 compared with the rate of 63% in Guinea, Liberia, and Sierra Leone (with no HLIUs) at that time. 19 Several reports have shown the feasibility of intensive care treatment under high-level isolation conditions in Europe and North America.20–24 However, few reports address the provision of critical care for Ebola virus disease patients in resource-limited settings, but they again indicate the feasibility of enhanced clinical management of patients with HCIDs.25,26
First, it was necessary to determine the feasibility of establishing an HLIU with advanced medical management of HCID patients without compromising intensive care provision for the Rwandan population. To address this question, we needed to assess current intensive care capabilities in Rwanda, including the number of intensive care units (ICUs) and beds, as well as the structural characteristics of the ICUs (eg, number, training, and qualifications of ICU staff, availability of medical equipment for intensive care, availability of medications and medical supplies).
At the beginning of the project, we conducted a scoping survey that consisted of visiting 3 ICUs in the capital city, Kigali, and 1 rural ICU at the university hospital in Butare, all of which were operational at the time. Using a standardized checklist (Box), we evaluated the capacities and structural features of staffing, equipment, and logistics for medications and medical supplies. Special attention was given to the training and qualifications of staff and the methods of continuous medical education for the professional groups involved. Finally, the ICUs were assessed based on quality indicators used by the German Interdisciplinary Society of Intensive Care Medicine in their peer review process. 27 This approach aimed to determine whether advanced medical management of HCID patients in Rwanda could be achieved at a level comparable to the German HLIU standard. Our assessment of the ICUs followed the methods described in the literature for low- and middle-income countries.28–31
Box. Items on Standardized ICU Checklist for Scoping Visits
Capacity
Staffing
Distribution of tasks to different vocations in the unit’s workforce
Patient-to-nurse ratio
Level of care (regarding organ support treatment)
Medical equipment
Logistics of medical consumables and medications
Scope and organization of diagnostic procedures
Professional training and continuing medical education of healthcare workers
10 quality indicators from the German Interdisciplinary Society of Intensive Care Medicine and Emergency Medicine (DIVI) 27
Daily multiprofessional and interdisciplinary clinical visits with documentation of daily goals
Management of sedation, analgesia, and delirium
Patient-adapted ventilation
Early weaning from invasive ventilation
Monitoring of infection prevention measures
Infection management measures
Early enteral nutrition
Documentation of structured patient and family communications
Early mobilization
Direction of the intensive care unit
The aim of the scoping survey was to determine whether the organizational structure of Rwandan intensive care medicine could support advanced medical management of HCID patients under the conditions of an HLIU and to estimate the system’s capacity once the Kigali HLIU is operational. The scoping survey did not examine whether the existing ICUs in Rwanda are sufficient for the population size.
All visited ICUs had comparable structures in terms of spatial and staffing arrangements. For example, all units are staffed and led by anesthesiologists. The shift system ensures the presence of a senior anesthesiologist who is solely responsible for the ICU for 12 hours during the day and provides nighttime coverage on an on-call basis. Additionally, an anesthesiology resident is on duty in the ICU for 12 hours, with no other responsibilities besides ICU care, and is supported by trainees from internal medicine and emergency medicine or by general practitioners. ICU nursing care is provided, with a patient-to-nurse ratio of 1:1, and is overseen by a nursing supervisor who is also exclusively dedicated to the ICU and, unlike the other ICU nurses, has an academic background in ICU nursing care. The medical expertise observed during the scoping survey was generally at the level of a high-income country. However, the availability of medical equipment, medications, and medical supplies was less extensive, although each ICU bed had typical equipment and the necessary medications were available to provide intensive care for a patient with organ failure. There were differences in the supply of medical consumables and medications compared to European and American ICUs, however, both in terms of quantity and variety available. The range of available diagnostics was significantly more limited compared with a high-income country and was not always available 24 hours a day/7 days a week.
The fact that all ICUs are operated in public hospitals indicates Rwanda’s political will to ensure comprehensive care for its population. 31 This model also forms the basis of the future operation of an HLIU with advanced medical management of HCID patients. In the event of an HLIU activation, there is no risk of reducing the personnel pool due to retaining staff for nonpublic hospitals.
The issue of transporting HCID patients was not within the scope of this project and review. However, given the manageable transport distances within Rwanda, an HCID case identified within the primary healthcare system would be transported to the capital city, Kigali, where most referral hospitals and healthcare workers are located. Therefore, establishing an HLIU in Kigali with connections to the University Teaching Hospital of Kigali made sense.
Training Needs Assessment
HLIUs are specifically designed to safely isolate patients with HCIDs from the surrounding population while providing them with the most comprehensive treatment possible to improve outcomes for diseases that currently have limited or no treatment options. Although such diseases can reach epidemic proportions, they generally occur infrequently, resulting in limited evidence on the medical management of HCIDs. 32 Approaches such as those used by the Joint Mobile Emerging Disease Clinical Capability (JMEDICC) 33 and the Infectious Diseases Isolation and Research Unit in Fort Portal, Uganda, 34 are viable methods to ensure efficient control of HCID outbreaks and to gather the necessary scientific data for future evidence-based HCID management. Thus, by establishing another HLIU in the East African region with similar goals, the Kigali HLIU should help accelerate both practical and scientific knowledge regarding HCID management.
Similar to HCID management, the field of HLIUs itself is still developing. Recommendations for physical infrastructure, IPC measures, personnel management, and training operations primarily stem from regional consensus efforts in Europe 35 and the United States 36 from the mid-2000s. Subsequently, new HLIUs have been established in the United States and worldwide, and the US National Emerging Special Pathogens Training and Education Center (NETEC), through its International Partnership Program, has facilitated global workshops and webinars (NETEC Global Rounds) for HLIUs to share experiences and network. Lukowski et al 37 recently compiled a narrative review of the literature on HLIU experiences, best practices, and persisting challenges over the past 2 decades.
Because this project is a collaboration between Rwanda and Germany, the experiences of German HLIUs, which have significantly contributed to European consensus recommendations, 35 form the basis for the joint planning of the Kigali HLIU in Rwanda. German HLIUs, although they regularly exchange ideas within a permanent working group, differ in terms of their physical infrastructure, usage (dedicated versus flexible use), and specific training methods. Therefore, at the project’s outset, a delegation from the Rwanda Biomedical Center, including an internal medicine specialist and an emergency physician, was invited to Germany to visit 3 representative HLIUs and consider their respective advantages and disadvantages. Special emphasis was placed on the different training concepts to identify the most suitable HLIU training approach for the future Kigali HLIU. There was a consensus that the format of the training program at the Berlin HLIU was the most appropriate.
In 2017, the HLIU at the Charité – Universitätsmedizin Berlin fundamentally changed its training approach to a team-based model in which all involved professional groups train together. This team-based training occurs monthly as a full-day event and brings together general nurses, ICU nurses, respiratory therapists, infectious disease specialists, and intensive care physicians to practice a team approach to managing an HCID patient, as they would during an actual HLIU activation. The training also includes mandatory safety guidelines for working in an HLIU in Germany, an introduction to the specific standard operating procedures of the HLIU, and a lecture on a selected HCID that staff might encounter while working in the HLIU. The practical training is organized into various modules covering donning and doffing of personal protective equipment (PPE), working in the point-of-care laboratory of the HLIU, invasive procedures (eg, insertion of vascular catheters, airway management, thoracocentesis), and emergency situations (eg, PPE breach, needle stick injuries, loss of consciousness in PPE). These training modules can be flexibly combined depending on the size of the training group and the trainees’ experience, but they are usually embedded in a case-based scenario involving an HCID patient using patient simulators and manikins. The case-based scenario allows team members to immerse themselves in real-life situations. Typical examples include admitting a patient to the HLIU when PPE complicates history-taking and physical examination or recognizing and managing an HCID patient whose condition deteriorates during the scenario. The training concludes with a short debriefing, providing an opportunity for participant feedback. The results of the debriefing allow for continuous adjustment of the training to meet the evolving needs of the trainees. 38
Based on the information about continuing medical education for healthcare workers gained from the ICU scoping visits, scenario-based multiprofessional training, including all members of the ICU team, represents a major change. Until now, ICU nurses and physicians were trained separately, except for training in cardiopulmonary resuscitation. Rwanda accepted the challenge of establishing a new team-based training and did not consider it an obstacle.
To further refine the training needs assessment of our project, a series of stakeholder interviews and a formal knowledge, attitude, and practice (KAP) survey were conducted among all ICU staff in Rwanda’s continuously operating ICUs. Findings from the interviews and the KAP survey also contributed to assessing the needs of the training program at the Kigali HLIU, to ultimately enable successful team-based training. Details about the conduct and results of the stakeholder interviews and the KAP survey will be published separately.
To obtain a more precise picture of the training needs for the future Kigali HLIU, a workshop was conducted in Kigali in November 2022 with participants including staff from the Rwanda Biomedical Center and the University of Rwanda, ICU nurses and physicians from the referral hospitals that run ICUs, IPC specialists, and a representative from the Rwanda WHO Country Office. During the workshop, the participants identified gaps in the healthcare system and challenges regarding the scope of planned HLIU training.
To date, there has been no formal academic training specifically for intensive care medicine in Rwanda. Intensive care is provided by anesthesiologists who rotate between operating theaters and ICUs, while nurses represent the permanent staff of ICUs. Intensive care training for physicians is integrated into academic training in the field of anesthesiology, while ICU nurses are recruited from general wards and are then trained on the job. Certain knowledge gaps among ICU nurses and physicians were identified, which makes it necessary to plan for a critical care refresher within HLIU training. At the request of the University of Rwanda and the Rwanda Biomedical Center, this critical care refresher is to be integrated into the future curriculum for intensive care subspecialization, which is already underway.academic training. There is no formal academic training specifically for infectious diseases in Rwanda. Against the backdrop of a growing problem related to antimicrobial resistance and the high risk of bacterial superinfection during prolonged supportive care of patients with HCIDs, it is necessary to integrate specific infectious disease content into the training program, which should be part of a future infectious disease curriculum for subspecialization. In September 2023, a workshop on antimicrobial resistance, antimicrobial stewardship, and IPC was conducted in cooperation with the German Corporation for International Cooperation and Robert Koch Institute, with funding from the German Federal Ministry for Economic Cooperation and Development. Rwanda has a limited number of IPC specialists who are exceptionally well trained and possess significant knowledge and experience. Due to their limited numbers, the dissemination of this knowledge across the entire Rwandan healthcare system appears to be insufficient. Certain knowledge gaps were observed in daily work during the scoping visits and subsequent internships at Rwandan ICUs. Additionally, the frequency of IPC knowledge refreshment seems inadequate, as evidenced during a refresher training for the original master trainers of the EFFO-I project. Besides routine donning and doffing drills, which can ultimately be conducted in classroom activities, the integration of IPC measures into patient care by interprofessional teams needs further development.
To determine the best approach to training and optimally address the specific needs of ICU nurses and physicians in Rwanda, a German ICU nurse and an intensivist from the Berlin HLIU conducted 2-week internships in Rwandan ICUs in the last quarter of 2023. During these internships, it became clear that Rwandan healthcare workers showed a distinct preference for workshop-based training with the opportunity to interact directly with lecturers during case discussions and practical training sessions. The option of a blended learning format, with online self-learning combined with interactive webinars and no additional bedside training, was clearly perceived to be less appealing and less likely to reach the necessary adherence of the audience.
The requirements for training gradually change with each training session and the team from Germany has limited opportunities to be consistently onsite in Kigali, which meant that some online learning was necessary and a compromise had to be reached. This compromise resulted in a training approach that consists of web-based self-learning units, interactive webinars on intensive care and HCID-specific topics, and practical workshops onsite. The practical workshops offer the opportunity to integrate IPC measures and medical management up to intensive care under HLIU conditions, which is needed for the escalation of medical care for a deteriorating patient, based on consensus-based recommendations. 39 The first training workshop was successfully conducted in March 2024 and provided the German trainers with their first opportunity to meet the future core team of the Kigali HLIU.
Outlook
Even after the construction of the Kigali HLIU is completed in the first quarter of 2025 and the core team of the HLIU staff will have received their initial training, some outstanding issues will remain.
High-level isolation care for patients with HCIDs carries a risk to involved healthcare workers. Therefore, a specialized set of standard operating procedures for HLIUs is necessary to ensure the safety of patient care. These standard operating procedures can only be developed after the construction of the Kigali HLIU is finished and a final decision regarding the composition of the HLIU workforce has been made.
German HLIUs have the benefit of being members of a nationwide permanent working group, which supports single units with peer review by the other units and with the ability to call in ad hoc consultations by other experts. Thus, all units can share their experiences with the training and actual care for patients with HCIDs. Because the Kigali HLIU will be one of only a few units in the East African region capable of managing HCID patients, it is vitally important to connect it to the German network of HLIUs.
Training for the management of HCID patients will ultimately become a routine practice for the Kigali HLIU. However, when this unit admits its first HCID patient, it would be helpful for the unit to be connected with a functioning telemedicine network, such as the Telemedicine Hub of the Department of Anaesthesiology and Intensive Care Medicine run by Charité – Universitätsmedizin Berlin outside the field of high-level isolation medical care.40-42 A telemedicine connection would allow for real-time support when caring for patients with HCIDs.
With financial assistance from the European Union, a new building for the National Health Laboratory Services is set to be constructed, which will also house a biosafety level 3 and 4 laboratory capable of handling highly infectious materials.
Installing an HLIU in a region where many HCIDs are endemic, combined with access to a BSL 3 and 4 laboratory nearby, provides an opportunity to advance the science of HCIDs. This will make the Kigali HLIU an interesting partner for scientific collaboration in the future.
Early in the project, the idea was expressed by the Rwandan team that the Kigali HLIU should develop into a training hub for the East African region, particularly in the areas of IPC, barrier nursing, and HCID patient care. Therefore, it would be advantageous to seek future exchanges with institutions in the region that were established in response to the COVID-19 pandemic or to manage HCID epidemics in Rwanda’s neighboring countries. Similar to how the German HLIUs have formed a permanent working group and continue to benefit from the routine exchange of experiences regarding training, education, and patient treatment, it is hoped that a similar network of institutions focused on HCID can be established in the East African region.
Ensuring that the Rwandan healthcare system has the capability to treat HCIDs effectively and safely is necessary to protect the health of the people in the country and East African region. The construction of the first HLIU in East Africa and the establishment of a robust training program for Rwandan healthcare workers in HCID management will contribute to addressing the region’s health security needs. In addition, increasing scientific collaboration with the new HLIU and strengthening the healthcare system in the region with its highly mobile population will further contribute to global health security.