
Abstract
The Sudan virus disease outbreak in 2022 prompted the Denver Health High-Risk Infection Team (HITeam) to evaluate and implement novel strategies to respond to viral hemorrhagic fever (VHF) events. To improve the VHF response, HITeam members developed a virtual assessment model (VAM) for at-home evaluation of individuals who are suspected of having a VHF. The VAM incorporates aspects of care that would normally be rendered in a high-level isolation unit—including assessment and monitoring, specimen collection, provider consultation, patient and family teaching, and pharmaceutical intervention—into a mobile framework in which team members respond to a suspected case at the individual’s home. Building this capability allows for more thorough assessment of a suspect case in the field, as well as the postponement of a decision about activation of the high-level isolation unit until more information is available. Development, testing, and implementation of the VAM required input from an interdisciplinary group of partners that demonstrated the ability of nurses, physicians, laboratorians, paramedics, emergency medical technicians, and public health personnel to integrate into 1 cohesive care team. The resulting model recenters VHF care on the patient by allowing the care team to gather critical information in an environment that is more comfortable for the suspect case while keeping communities safe and lowering exposure risks. The VAM has long-term sustainability implications for global VHF programs and provides solutions for broader challenges in healthcare by modeling cost-effective, patient-centered care within the highly nuanced subspecialty of special pathogen care.
Introduction
I
There is currently no universally agreed upon list of pathogens for which admission to an HLIU would be recommended. Determination of admission of a confirmed or suspected special pathogen case to an HLIU is based on hazard (as measured by morbidity and mortality), infectiousness (as measured by ID50), communicability (as measured by R0), 4 and the limited availability or lack of approved medical countermeasures for the pathogen (Figure 1). When considering available resources, recommendations may vary between institutions and countries.
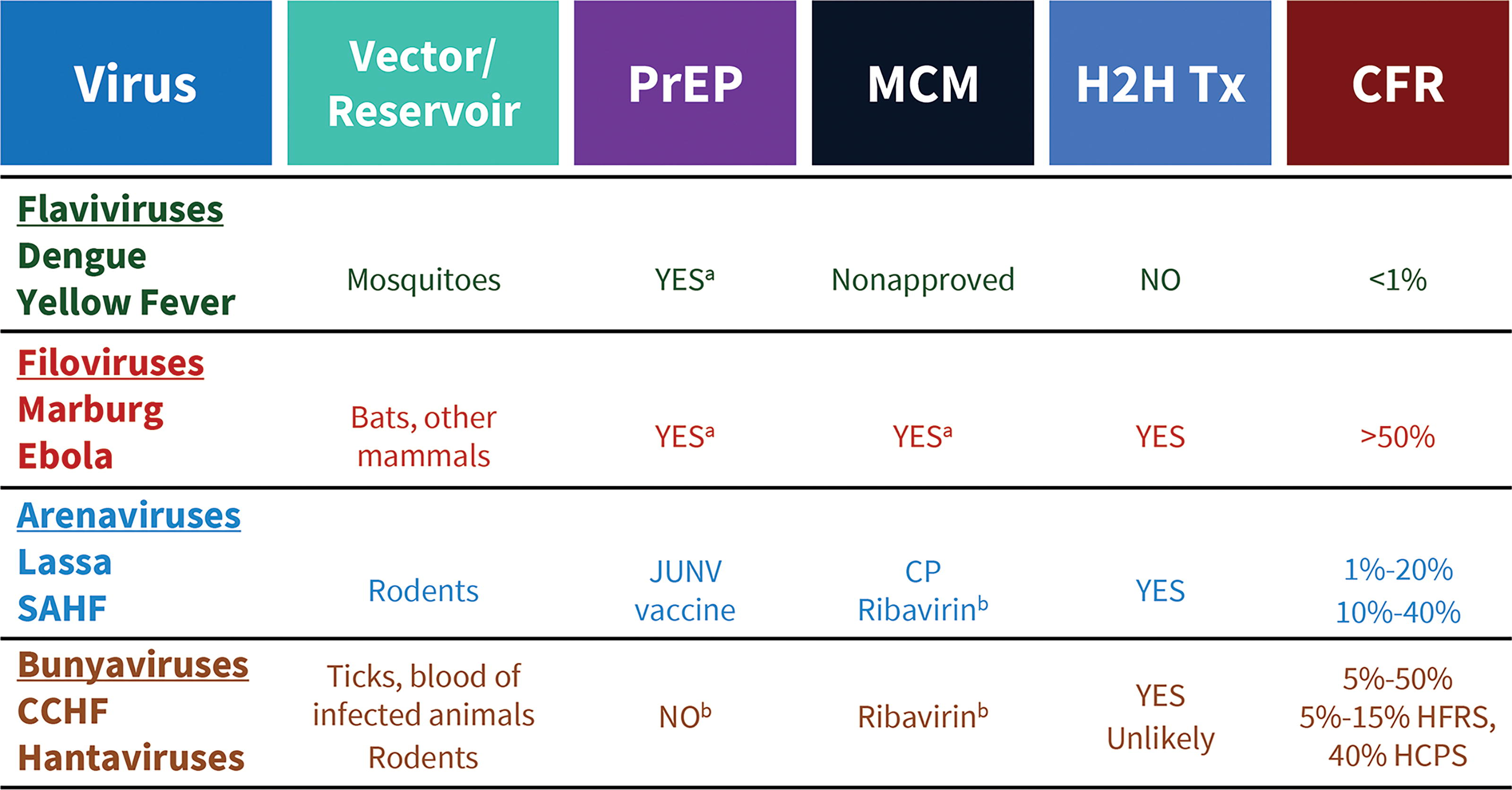
Sample of pathogens that cause common viral hemorrhagic fevers and high-level isolation needs. For each underlined virus family, examples of viruses in that family are included, along with associated vectors, the availability of preexposure prophylaxis and medical countermeasures, the possibility of human-to-human transmission, the need for HLIU activation, and estimated case fatality rates. Currently, patients infected with flaviviruses would not be admitted to an HLIU. aFor some cases. bNot approved by the US Food and Drug Administration. Abbreviations: CCHF, Crimean-Congo hemorrhagic fever; CFR, case fatality rate; H2H Tx, human-to-human transmission; HLIU, high-level isolation unit; MCM, medical countermeasure; PrEP, preexposure prophylaxis; SAHF, South American hemorrhagic fever.
The US Centers for Disease Control and Prevention (CDC) has developed and regularly updates guidelines for monitoring travelers returning to the United States from areas with VHF outbreaks. 5 When a returning traveler is identified as having a high-risk exposure but is asymptomatic, a 21-day quarantine is mandated. For asymptomatic travelers with non-high-risk exposures, a 21-day self-monitoring plan is implemented. These non-high-risk exposures fall into 3 distinct categories, each requiring a self-monitoring plan. If any of these returning travelers develop symptoms within 21 days following exposure, a suspect case status is designated, either by the CDC for individuals in quarantine or by local public health agencies for those with non-high-risk exposures. 6
A suspect case for a VHF is defined as someone with signs and symptoms that are consistent with or concerning for a VHF and who had an epidemiological risk factor within 21 days before symptom onset. The relevant VHF symptoms are a fever (100.4°F/38.0°C or higher) AND at least 1 dry (aches and pains, such as severe headache and muscle and/or joint pain; weakness and fatigue; odynophagia; anorexia; red eyes; skin rash; hiccups) or wet (gastrointestinal symptoms, including abdominal pain, diarrhea, and vomiting; unexplained hemorrhaging, bleeding, or bruising) symptom. It is important to note that the early symptoms of these diseases are often nonspecific. If laboratory confirmation of a VHF is obtained, the suspect case becomes a confirmed case. 6 Notably, most VHF suspect cases are eventually ruled out. During the third and fourth quarter of 2014, and amid the EVD outbreak in West Africa, the CDC addressed approximately 650 clinical inquiries, 118 of which met EVD suspect case criteria. Of those suspect cases, 61 were tested and 4 people were diagnosed with EVD (less than 4% of suspect cases). 7 This underscores how crucial it is to assess suspect cases consistently and comprehensively.
Traditionally, suspect cases have been admitted to HLIUs until VHF is ruled out or diagnosis is confirmed. Until a diagnosis is confirmed or ruled out, the suspect case must remain in isolation, occupying a single room with a dedicated bathroom. Standard contact and droplet precautions must be followed, along with the use of appropriate personal protective equipment (PPE), by all healthcare professionals caring for the individual. 8 A detailed epidemiological history is essential, with specific attention to locations visited, leisure and work-related activities, animal exposure, consumption of untreated water or undercooked meals, vaccination status, prophylactic measures for endemic diseases, living arrangements, and attendance at burials; current local and seasonal epidemiological factors should also be considered. 9
The Denver Health High-Risk Infection Team
Denver Health and Hospital Authority (DHHA) is a Regional Emerging Special Pathogen Treatment Center (RESPTC). The Denver Health Paramedic Division (DHPD) is based at the institution along with the Denver 911 system. Additionally, the Public Health Institute at Denver Health operates public health clinics and the Denver Prevention Training Center. 10 DHHA’s unique structure provides the high-risk infection team (HITeam) the opportunity to collaboratively and seamlessly train on, innovate, develop, and implement interdisciplinary procedures. 11
The Sudan virus disease outbreak in the fall of 2022 served as a catalyst for the HITeam to pioneer groundbreaking strategies for responding to VHF events. In their quest to enhance both flexibility and efficiency in addressing such pathogens as the Sudan virus, HITeam members conceived and developed a game-changing innovation: the Virtual Assessment Model (VAM), designed for remote evaluation of VHF suspect cases.
The VAM integrates components of care typically provided within HLIUs—encompassing physical assessments, continuous vital signs monitoring, specimen collection, expert consultations, patient and family education, and targeted pharmaceutical interventions—into a mobile response framework that dispatches special pathogen clinicians directly to the individual’s residence (Figure 2). Establishing this mobile response capability equips the HITeam with the capacity to conduct comprehensive assessments in the field while deferring the decision on HLIU activation until additional information becomes available.
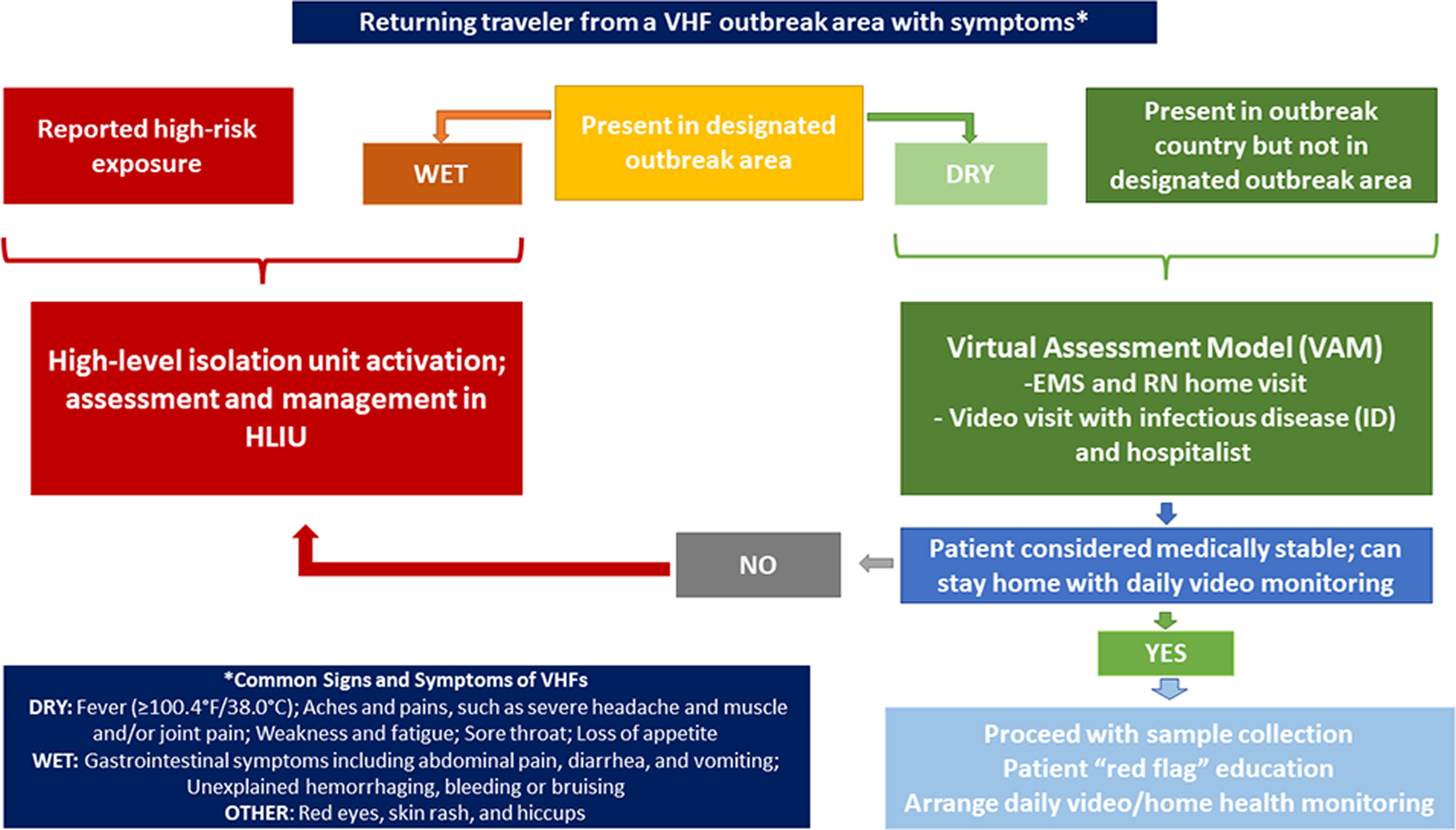
Assessment and response algorithm for SCs of VHF. SCs that exhibit “wet” symptoms or who are deemed high risk based on their exposure history would be ideal candidates for management in an HLIU. Individuals only exhibiting “dry” symptoms who do not have any reported high-risk exposures would be considered for at-home evaluation via the VAM. Depending on the results of the clinical at-home assessment, SCs may be transported to an HLIU or managed at home by a combined healthcare/public health team. Abbreviations: EMT, emergency medical technician; HLIU, high-level isolation unit; RN, registered nurse; SC, suspect cases; VAM, Virtual Assessment Model; VHF, viral hemorrhagic fever.
Virtual Assessment Model
A series of steps must be taken to trigger the VAM for each individual case, beginning with initial assessment of the situation and gathering of pertinent information. Typically, a healthcare facility will receive notification of a suspect case from a public health agency, prompting a discussion about the individual’s epidemiological factors, reported symptoms, and monitoring history. Following this contact with the public health agency, the institution housing the HLIU, in conjunction with public health partners, will arrange an initial call to bring together all relevant parties and determine whether HLIU or VAM activation is needed. If any activation decision is made, a second call will follow and will involve necessary parties to activate the HLIU or implement the VAM. Suspect case contact information and any unique requirements, such as the need for interpreters, will be obtained through the public health agency, which will also inform the suspect case of next steps.
If the decision is made to implement the VAM following collection of pertinent information, the next step—mobilization of resources—begins immediately. A registration officer or transfer center personnel will facilitate the creation of a patient virtual encounter record in which to document visits and print patient labels before the response team departs for the suspect case’s home. Prior to implementing the VAM, involved parties will rehearse the activation and implementation process to ensure their competency in all required steps (Table) and to identify potential challenges that may arise during the response. Simultaneously, a separate group of team members will begin preparing for suspect case admission to the HLIU. Some of these tasks include incumbent patient movement out of the designated HLIU room, initiation of the staffing plan, room setup, and gathering of unit-specific supplies. These steps ensure the HLIU’s readiness if the suspect case is admitted. The remaining steps in VAM activation revolve around the execution of protocols to deliver an assessment and necessary interventions in the suspect case’s home. These protocols can be described from 2 perspectives: the setting perspective—which includes the coordinating area, home of the suspect case, and virtual visit space—and the staffing perspective.
Considerations for At-Home Assessment of Suspect Cases of Viral Hemorrhagic Fever
Abbreviations: DHHA, Denver Health and Hospital Authority; EMR, electronic medical record; EMT, emergency medical technician; NP, nasopharyngeal; OP, oropharyngeal; PMH, past medical history; PPE, personal protective equipment; PSH, past surgical history; SH, social history; VAM, Virtual Assessment Model; VHF, viral hemorrhagic fever.
State and local public health partners participate in the development, testing, and exercising of the VAM with DHHA and in the decision to activate either the VAM or the HLIU. Public health agencies also provide support during the in-home assessment and monitoring and follow-up after the visit.
Setting
The coordinating area will be located at the responding institution and will involve a multidisciplinary team consisting of emergency management personnel; public health agency representatives; registration professionals; informatics liaisons; discipline leaders from nursing, paramedics, laboratory, and medical staff; and other subject matter experts as needed. This team will coordinate communications with key stakeholders, activate the VAM response framework, facilitate encounter creation and virtual visit appointments, collaborate with public health and security agencies as necessary, monitor VAM progress, and prepare the HLIU for activation. Candidacy for a virtual assessment of a suspect case will be determined using all available information; ideal candidates will exhibit dry symptoms and will be determined to have had a non-high-risk exposure to a VHF (Figure 2).
Once criteria to activate the VAM are met, a home visit team will be assembled. This team will travel as a convoy of at least 3 vehicles, including at least 1 ambulance. Responding personnel will include at least 2 paramedics, 1 registered nurse, and 1 laboratory technician, all trained in managing VHF patients and high-level isolation. The target response time for this team is 4 hours from notification but may fluctuate depending on the suspect case’s location. The Table provides a step-by-step description of tasks, including PPE donning, clinical assessment, sample collection, PPE doffing, and the roles to be filled by all members of the home visit team. As clinical tasks are being performed at the suspect case’s domicile, responding team members will initiate a virtual provider visit to inform final call disposition (ie, a decision for at-home quarantine of the suspect case or transport to the HLIU).
Team members responding to the suspect case’s home will remain present throughout the virtual assessment in case transfer to the HLIU becomes necessary. The video call will be conducted in the suspect case’s home using a facility-provided tablet device, such as an iPad, that has Wi-Fi connectivity, a built-in camera, audio that can be placed on speaker mode, and the necessary application(s) for a virtual visit. Both a hospitalist and an infectious disease physician will join the video call with the suspect case. During this visit, comprehensive epidemiological, immunization, and medical histories will be collected, including history of present illness, symptoms, and prophylaxis used during travel. Education on what to expect and a follow-up plan will be provided to the suspect case. A visit template and order set will be available via the electronic medical record for visit standardization. The virtual assessment will also include an assessment of the environment in which the suspect case resides and impacts on family members or others who may be affected by a decision not to transport.
Staffing
Successful implementation of the VAM requires engagement from many healthcare professionals and partners. When DHHA received the RESPTC designation, it established a fully voluntary, multidisciplinary HITeam with specialized training in PPE donning and doffing and HLIU protocols. Members participate in mandatory drills every 6 weeks to practice team dynamics and dexterity while wearing PPE. They also take part in regular exercises to simulate and prepare for real-world VHF response scenarios. HITeam members are considered subject matter experts in the field of special pathogens and work to continually enhance their knowledge through participation in regional and national educational opportunities.
The DHPD High-Risk Infection Transport Team leads prehospital evaluation and transport of VHF patients. The DHPD consists of paramedics, emergency medical technicians, communications specialists, vehicle service technicians, and command staff. Upon activation of the VAM, the paramedic team will prepare the vehicles and supplies needed for the in-home evaluation. Preparation of the convoy will also include resources necessary for transport to a hospital if required. At a minimum, the convoy will include 1 ambulance prepared for transport and 2 chase vehicles. In addition to vehicles and supplies, convoy preparation includes coordination with the Denver 911 Communications Center to ensure open and monitored communication throughout the operation. For the DHHA’s VAM, response radius is determined on a case-by-case basis and is limited to the DHPD’s standard response area.
The VAM activation structure will include additional HLIU staff—namely, registered nurses and laboratorians—in DHPD’s typical mobile response structure. These team members will assist the at-home response portion of the activation and provide support to the DHPD as needed. Setting-specific training and familiarization for hospital-based staff occur as part of the standard training package for HITeam members; these include topics such as patient handoff and specimen collection. However, each team member’s duties during the VAM response will be limited to their preestablished scope of work. Members are also encouraged to ride along with the DHPD to become acquainted with the prehospital setting.
The virtual component of the VAM will be fulfilled by HLIU medical staff, who will complete the suspect case assessment and provide recommendations for next steps in the care journey. Since 2018, the medical staff of Denver Health’s HLIU has comprised 2 interdisciplinary groups led by hospital medicine physicians as the primary managing service. The first group of physicians, responsible for providing direct primary care to patients, includes 10 specially selected and trained hospitalists, a small team of pediatricians, and consultants from emergency medicine, critical care, and infectious diseases. The second group consists of consultants in various specialties, such as nephrology, anesthesia, general surgery, radiology, and gynecology. Just-in-time training is available for these consultants as needed, and the expertise of all team members is leveraged to ensure a comprehensive and well-rounded approach to caring for biocontained patients. 11
Implementation
Upon departing DHHA following VAM activation, the paramedics, registered nurse, and laboratorian will don PPE. In the field, paramedics will assess scene safety, initiate suspect case contact, and lead clinical evaluation of the suspect case. Additional public safety personnel may be recruited to secure the scene from outside the residence. If on-scene conditions render the VAM unworkable for any reason, transport of the suspect case to the HLIU will proceed. The paramedic team will divide into specific roles to ensure the safety of responding team members and reduce the risk of specimen or equipment contamination. The driving paramedic, not fully donned in PPE, will remain outside the residence with the laboratory team member and will assist with the movement of equipment and collected specimens. The attending paramedic team and registered nurse will enter the primary residence to assess vital signs, perform a physical examination, and facilitate a virtual assessment with a provider.
Prior to dispatch, the HLIU registered nurse will be responsible for gathering needed testing supplies and will join paramedics in donning PPE. The registered nurse’s most critical role during execution of VAM protocols is as a trained observer. In this capacity, the registered nurse will monitor responding personnel and the suspect case to minimize risk of exposure. The registered nurse will focus on monitoring the environment and will set up the virtual visit. They will communicate interventions and coordinate provider orders and specimen collection. Specimen collection and other at-home interventions will be performed by team members according to scope of practice. After the visit, the registered nurse will assist with the transport of specimens and waste, observe PPE doffing, and continue to advocate for ongoing patient care needs.
The high-risk pathogen laboratory (HRPL) will designate 1 laboratory team member (packager) to don appropriate PPE and participate in the VAM home visit. A second designated lab team member will ready the HRPL for testing, including running quality control on all analyzers and ensuring the necessary reagents and supplies are ready for use. At the suspect case’s home, the paramedic or registered nurse (the collector) will follow the specimen collection protocol, which includes placing blood collection supplies in a predesignated zone. Once the specimens have been collected, they will be placed in a separate zone. The specimens collected will include blood cultures and tubes for hematology, chemistry, serology, and coagulation testing. In addition, a urine specimen, a nasopharyngeal swab, and a stool specimen may also be collected. The collector will be responsible for affixing patient labels to specimens, triple-bagging them, and applying appropriate disinfection techniques at each step of the collection process. The lab team member (the packager) will receive the triple-bagged specimens into the appropriate shipping container just outside of the collection area. The packager will finish packing samples in a Category A shipping container, which must include a leakproof primary receptacle, a leakproof secondary receptacle, and rigid outer packaging. At this point, the specimen box is considered safe to handle and transport without PPE. The shipping box will be loaded into a convoy vehicle and transported back to the responding institution for analysis in the HRPL. If needed, the HRPL staff will repackage any specimens to be sent to the state health laboratory or the CDC for confirmatory testing of a suspected VHF.
For VAM video visits, both infectious disease and hospital medicine physicians will be involved, each offering a unique perspective on patient care and needs. Infectious disease specialists will focus on differential diagnosis and the management of suspect cases, and hospital medicine physicians will concentrate on clinical patient management and determination of the appropriate level of care. During the virtual visit, recommendations for a workup and sample collection will be made based on the suspect case’s history and examination findings.
Responding team members will consider prevalent and seasonal diseases in the suspect case’s current and originating location, considering factors such as respiratory virus season, vaccine-preventable diseases based on the suspect case’s immunization status, and local endemic or seasonal infections like tick-borne encephalitis, Lyme disease, hantavirus infection, and endemic mycosis. Special attention will be given to diseases endemic or prevalent in the area the suspect case has recently returned from, such as malaria, VHFs, yellow fever, dengue, or other diseases depending on the geographic area visited. Occupational exposures and other infectious diseases, such as pneumonia, meningitis, and typhoid fever, will also be considered.
VAM activation will result in 2 possible outcomes: either the suspect case will be deemed not appropriate for ongoing virtual monitoring and will be transported to an HLIU, or they will be considered appropriate for ongoing virtual monitoring with frequent disposition reassessments and specimens will be transported to the HRPL. Once the visit is concluded, the driving paramedic will assist the laboratory team member in packaging laboratory samples and any waste accumulated during the visit. The paramedic team will facilitate the safe transportation of healthcare professionals and any specimens collected back to the responding institution. Doffing of PPE for the entire prehospital team will be completed according to the existing standard operating procedures. Current DHHA standard operating procedures indicate that healthcare professional doffing will take place in a predesignated space within the coordinating area, where waste can be safely handled and healthcare professionals have access to a shower. In certain scenarios, considering factors such as team safety and exposure risk, doffing in the field could be considered acceptable. Decontamination of the ambulance will occur according to existing standard operating procedures, regardless of whether a suspect case was transported or not. The paramedic team will remain in a state of readiness should the suspect case’s condition change and transport become necessary.
Discussion
A prime motivating factor for development of at-home assessment and testing models for VHF suspect cases is to refocus care on the consumers of healthcare, as opposed to healthcare systems. Under traditional frameworks for VHF response, suspect cases must be admitted to healthcare facilities equipped to evaluate and test such cases. Currently, there are 13 RESPTCs within the United States, each covering large, multistate geographic areas. Depending on the suspect case’s location and the local jurisdiction’s comfort level with responding to VHF events, access to needed care could be delayed by hours or even days while the suspect case waits for responding agencies to coordinate their efforts. Importantly, many of these suspect cases will eventually be ruled out for VHFs 7 but may still need care for differential diagnoses, such as malaria, where timely access to treatment is paramount.
The use of innovative models for patient care delivery aligns with new initiatives at the federal level, including by the US Department of Health and Human Services. 12 Leveraging improvements in telehealth and other novel care approaches via the VAM allows for quicker assessment, diagnosis, and treatment of individuals and subsequently shorter wait times to definitive care. The VAM also allows individuals to receive care in their home, thus enhancing comfort for the individual being assessed and reducing the risk of community and healthcare professional exposure that is associated with admitting suspect cases to an RESPTC or similar facility.
The ability of the VAM to leverage these technologies not only decreases risk of spread of infection, but it also reduces the burden on healthcare facilities. Activation of an HLIU is costly, and more costs are incurred as the duration of stay in the HLIU is extended. Although published literature detailing HLIU activation costs eluded us, our internal cost analysis suggests that the VAM may result in cost saving compared with traditional HLIU activation, though this conjecture warrants further exploration. Additionally, standard hospital and prehospital workflows are often greatly interrupted by HLIU activation. The process of readying an HLIU is time-consuming, and reallocating staff can prove challenging. These cost and staffing challenges can create ripples across healthcare facility enterprises, as partners may be forced to step up to fill gaps, thus negatively impacting local and regional patient care.
The VAM could alleviate the resource strain on healthcare facilities responding to VHF events by delivering necessary care directly to the suspect case while offering an opportunity for responders to gather more information about the nature of the event. Although just-in-time training programs can familiarize staff with VHF response frameworks, untrained healthcare professionals may experience anxiety while caring for VHF suspect cases. Allowing a clinically stable suspect case to stay home enhances the suspect case’s comfort while minimizing untrained healthcare professional exposure and limiting impact on standard workflows. Furthermore, even though VAM candidates are expected to be low risk for VHF and hemodynamically stable with dry symptoms only, the VAM maintains the capability to escalate a response to a complex situation, including transport of the suspect case to an HLIU or redeployment of a transport team if clinically necessary. Thus, the level of care can be tailored to the unique needs of the suspect case rather than taking a one-size-fits-all approach.
To be sure, this model has limitations. Most aspects of the mobile response require specialized training. Scope of practice for each profession dictates who can perform which interventions, and some team members may find themselves in an unfamiliar environment, such as an individual’s home. Our model was designed to be implemented at our institution, where all team members are DHHA employees. Even though we believe the VAM could be modified to meet other institutions’ needs, adapting a mobile response framework will require careful evaluation of the existing resource capacity and policy, procedure, and partner needs of each jurisdiction to determine local and regional model feasibility.
The ability of the VAM to assemble a diverse, interdisciplinary group of healthcare professionals cannot be understated. Collaboration throughout the planning and execution phases of this model allowed leaders in public health, transport, hospital care, and other functional areas to provide and access critical information to optimize special pathogen response endeavors. Planning efforts highlighted cross-disciplinary collaboration on assessing and caring for VHF cases in the United States. Considerations such as threshold for VHF testing, risk stratification of return travelers, and VHF response capabilities of frontline facilities are best addressed by interdisciplinary teams to ensure all parties have a voice in developing the VHF response framework of tomorrow.
Conclusion
In response to the 2022 Sudan virus disease outbreak, the HITeam developed and tested the VAM, a remote evaluation tool for individuals potentially infected with serious pathogens. The VAM extends assessment from HLIUs to suspect cases’ homes, allowing for in-field physical assessments, monitoring, and interventions. It enables HITeam responders to make informed decisions on hospitalization needs based on detailed onsite evaluations, thus enhancing patient comfort while reducing healthcare professional exposure risk.
The VAM is built to enhance the National Special Pathogen System capacity by ensuring appropriate resource allocation, addressing surge capacity concerns, limiting impact to hospital operations, and delivering patient-centered care while reducing healthcare professional safety concerns. Healthcare delivery models must be dynamic. Healthcare facilities, with abundant or limited resources, should evaluate if a VAM could be a viable care model in their settings. Awareness of current special pathogen preparedness, development of interdisciplinary internal and external relationships, leveraging of existing operational resources, and in-depth knowledge of local and regional regulations are cardinal to the success of innovative care models. Our proposed VAM provides an effective and sustainable model, potentially marking a significant stride in patient-centric and cost-effective care for VHFs globally.
Footnotes
Acknowledgments
The authors would like to acknowledge all of the partners who were instrumental in developing, exercising, and formalizing this protocol, without whom this project would not be possible, including: HITeam members Heather Escudero, RN; Nicole Burnet, RN; Hanna Bayacal, RN; Clayton Robertson, RN; Benjamin Comden, RN; Brittani Handley, RN; Nikki Chapas, RN; Teresa Tomlinson, RN; and Matt Ramsey, RN; DHPD High-Risk Infection Transport Team members Deputy Chief Brent Stevenson, Lt. Erik Harris, EMT-P; Lt. Will Hargreaves, EMT-P; Lt. Eric Dailey, EMT-P; Kayla Anderson, EMT-P; Damion English, EMT-P; Vernita Lewis, EMT-P; Austin Lindemann, EMT-P; Todd Petrassi, EMT-P; Eric Sheffey, EMT-P; and Frank A. Warren, NREMT-P; high-risk pathogen laboratorian Jenna Rocker, MLS; infection prevention/infectious disease consultants Deborah Aragon, MSPH, CIC; and Heather Young, MD; emergency management consultants Emma Paras, MPH CEM, CHEP, MEP, and Bill Neville, MA; and the countless professionals from state and local public health departments, information technology services, and other RESPTCs who shared their insights and expertise and continue to be invaluable to planning and preparedness efforts. The Region 8 RESPTC at Denver Health is funded by the US Department of Health and Human Services’ Administration for Strategic Preparedness and Response (award number 5 U3REP220684-02-00).