
Abstract
This case study describes the experience of the German Permanent Working Group of Competence and Treatment Centers for High Consequence Infectious Diseases, known as STAKOB (Ständiger Arbeitskreis der Kompetenz- und Behandlungszentren für Krankheiten durch hochpathogene Erreger). STAKOB brings together public health authorities (competence centers) and high-level isolation units (treatment centers) to collaborate on the clinical management of high-consequence infectious diseases (HCIDs) and emerging infectious diseases. The network is coordinated by the Robert Koch Institute, Germany’s federal public health institute. The main tasks of STAKOB are to strengthen HCID clinical and public health management and increase expert knowledge on HCID and non-HCID emerging infectious diseases in Germany. STAKOB enables the exchange of knowledge and experiences; development of guidelines on infection prevention and control measures, clinical management, and therapy; and support for the World Health Organization and other outbreak responses internationally. The past years have shown how important the STAKOB network is for Germany—not only in providing critical care for HCID cases but also increasing capacity to support public health and clinical management of emerging infectious disease cases. However, maintaining several high-level isolation units in Germany requires a high commitment of financial, material, and human resources. Due to the rarity of HCID and emerging infectious disease events, maintaining the appropriate level of preparedness and ensuring sufficient investments is an ongoing struggle. Nevertheless, it is essential to have a network ready to react to HCID and non-HCID emerging infectious diseases in times of a changing biosecurity and infectious landscape.
Introduction
T
The collaboration between German high-level isolation units (HLIUs) started in 1999, initially on an informal level, when the clinical care of a patient infected with yellow fever was discussed and shared between clinical experts from German treatment centers. The informal network further evolved in 2003 when the clinical experts were joined by representatives from relevant public health authorities. Joint learning experiences during infectious diseases outbreaks, most recently the COVID-19 pandemic and mpox multicountry outbreak, emphasize the importance of interfaces between clinical management teams and the public health sector.
STAKOB was formally established in 2014 as a permanent working group at the Robert Koch Institute (RKI), Germany’s federal public health institute. Today, STAKOB includes preparedness and response experts from 8 public health authorities (competence centers) and clinical experts from 7 HLIUs (treatment centers), as well as specialists from other institutions (eg, the Federal Institute for Vaccines and Biomedicines [also known as the Paul-Ehrlich-Institut], the Federal Institute for Drugs and Medical Devices [also known as the Bundesinstitut für Arzneimittel und Medizinprodukte], the medical service of the German Federal Foreign Office, and the medical service of the German Armed Forces). These network members work together to support STAKOB activities and address challenges related to HCIDs and non-HCID EIDs.
RKI supports and coordinates the network by holding meetings on different topics at least once a year with international participants. Previous disease topics included Crimean-Congo hemorrhagic fever, Middle East respiratory syndrome, Lassa fever, Ebola virus disease, COVID-19, mpox, and Nipah virus disease. In addition, structural or organizational topics, such as medication stockpiling, staff exchange possibilities, temporary shutdowns of HLIUs, and construction of new HLIUs or training programs, have been discussed.
Emergency support for the network is maintained 24 hours a day/7 days a week by RKI. Within 2 hours of an event, response ad hoc meetings can be organized, which may include the discussion of an individual patient, advice on postexposure prophylaxis, or a response to a public health threat or crisis situation. Low-threshold direct communication—easily accessible collaboration between professionals without bureaucratic barriers—is established between the teams of the participating centers and is commonly used for ad hoc support.
To ensure comprehensive care for suspected or confirmed HCID or non-HCID EID cases in Germany, STAKOB forms a strategically structured network, ensuring that patients from anywhere in Germany can receive highly specialized care within a few hours in 1 of the 7 HLIU treatment centers (Figure) across Germany.
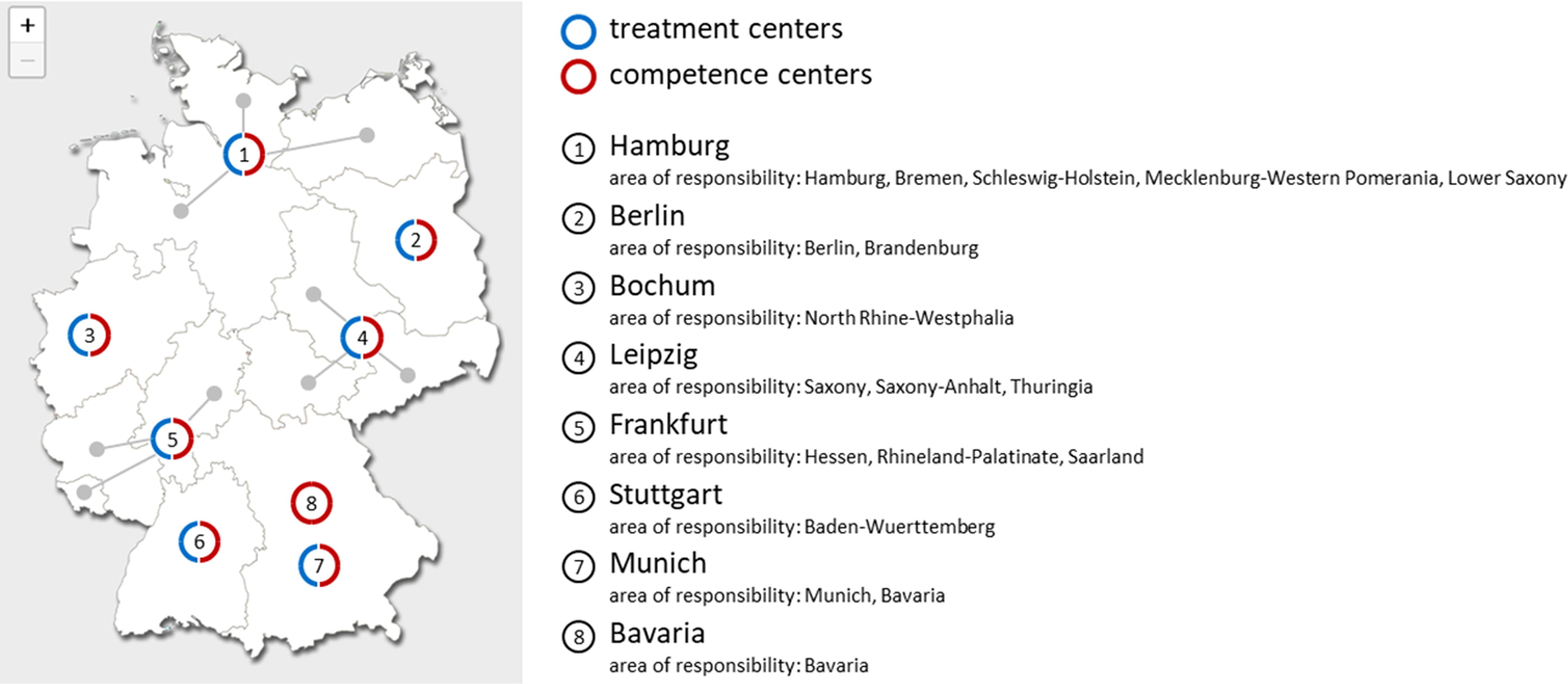
Distribution and responsibilities of STAKOB centers in Germany. 1
Regulatory Framework and HLIUs in Germany
In Germany, responsibility for health protection rests at the state level, and therefore responsibilities vary slightly between the states. Hospital financing is based on the principle of “dual financing,” in which the operating costs of hospitals (ie, all costs incurred for treatment of patients) are financed by health insurance, whereas investment costs are usually financed by states. As a result, the states make decisions on building, expanding, or closing hospitals, as well as financial investment measures. There are no nationwide specifications as to how many hospitals are to be maintained at which level. However, as a result of resource constraints, states have reduced their obligatory commitment to financial investments in recent years.
The German Technical Rules for Biological Agents 2 state the requirements for deciding which patients infected by certain pathogens need to be treated in an HLIU and the necessary structural and organizational requirements. In general, patients with diseases caused by pathogens in Risk Group 4, such as the Ebola, Marburg, and Lassa viruses, and some pathogens in Risk Group 3, such as Yersinia pestis, are to be treated at an HLIU. Depending on the transmission route, an unknown pathogen, such as SARS-CoV-2 at the beginning of the pandemic, would also be classified as a high-risk pathogen.
Due to the geographical distribution of the 7 HLIUs in Germany and the shared responsibilities for each HLIU between states, accessibility to an HLIU from any part of Germany can be guaranteed within a few hours, 4 to 6 at the most.
The individual HLIUs differ in their structure and the ways in which they are normally used. Some HLIUs are used as normal wards on a day-to-day basis, and, as such, patients would need to be transferred in the event of an HLIU activation. Other units are used on a day-to-day basis purely as training sites. What all HLIUs have in common is the use of personal protective equipment (PPE) with positive pressure systems that recirculate air, such as ventilated full body suits. To ensure the same high-quality standard in HLIUs for patients at higher risk of severe outcomes, the relevant specialist disciplines are usually involved on a consultative basis and in regular training sessions.
The total planned bed capacity for the highest protection level of all HLIUs together is around 30 beds. In order to treat a significantly larger number of patients at the highest protection level, plans to expand the capacity for patient isolation for such emergency situations, including supplementary treatment facilities, are required and would need to be developed further.
Tasks of STAKOB
STAKOB’s main tasks are to strengthen the infrastructure of HCID management in Germany and increase expert knowledge on the management of HCIDs and non-HCID EIDs. Management includes not only clinical patient care but also public health interventions, such as enforcing infection prevention and control (IPC) measures and providing recommendations for preexposure or postexposure prophylaxis. STAKOB promotes the exchange of knowledge and experience among affected facilities and provides advice to RKI, public health authorities, and individual physicians.
STAKOB provides advice on the clinical application of rare or unusual vaccines (eg, consulting on postexposure prophylaxis vaccination after high-risk occupational exposure to Ebola virus) or medication (eg, tecovirimat for mpox) within 1 to 2 hours by coordinating an initial virtual meeting with network members. The working group is ideally positioned to respond to acute infectious disease emergencies, HCID and non-HCID EID, at both the patient and public health levels within a few hours, depending on the type of emergency. As such, it is an important pillar of pandemic preparedness in Germany.
Furthermore, STAKOB develops treatment guidance for HCIDs or non-HCID EIDs (eg, mpox, pneumonic plague, COVID-19, Ebola virus disease) and offers recommendations on the handling of suspect cases, IPC measures, and clinical management in the event of an unusual epidemic occurrence or in bioterrorist incidents. Easily accessible documents, including IPC and treatment recommendations, expert opinions, flow charts, interactive online tools, are published on the STAKOB website. 1
To inform healthcare professionals, STAKOB conducts regular videoconferences involving external national and international experts (eg, virologists and microbiologists from relevant reference laboratories for diagnostic questions or international clinical experts) to discuss current outbreaks (eg, Monkeypox Working Group), as well as public webinars on HCIDs and non-HCID EIDs (eg, COVID-19) in the recent past. Under the coordination of RKI, STAKOB offers advice and training for hospitals on initial measures for patients with HCIDs, general practitioners in the case of an initial presentation, emergency rooms or hospitals without HLIUs, and corresponding expertise.
Competence Centers
According to the German Infection Protection Act, 3 HCID cases are legally required to be reported to local public health authorities, which are responsible for advancing the notification to respective state authorities that will involve RKI, the responsible federal agency. The 8 competence centers of the STAKOB advise local public health authorities on the management of HCID or non-HCID EID cases and public health measures. They operate within the German Public Health Service, with 3 located at a state ministry of health, 2 at a state health office, and 3 at a local health department. Five competence centers have an international airport within their area of responsibility, according to provisions outlined in the International Health Regulations (2005). 4
The expertise of competence centers is enhanced by infectious disease and IPC specialists, hygiene inspectors, and other professionals from a range of institutions, including local and state public health authorities, research institutions, rescue services, and the German armed forces.
Competence centers coordinate responses in the case of an HCID or non-HCID EID outbreak. These may include decisions on isolation or quarantine, postexposure prophylaxis, decontamination, waste disposal, autopsies and burials, and contact tracing (either by telephone or onsite support). They also provide decisionmaking assistance onsite and logistical support regarding diagnostics, referral, or the safe transfer to treatment centers for patients suspected of HCIDs or non-HCID EIDs.
Depending on their legal and geographical regulations, expert consultants advise and support the respective public health authority, with a focus on HCID infection protection on a local or regional scale. The competence centers also ensure implementation of IPC measures (eg, quarantine or isolation of suspected cases), resulting in appropriate control measures and successful situation management without further spread. 5
Treatment Centers
Germany has 7 HLIU treatment centers with well-trained staff specialized in the management of HCIDs and non-HCID EIDs. In each HLIU, patients with HCIDs can be treated according to biocontainment standards and receive specific diagnostics and advanced levels of care (including critical care). Training of providers on the proper use of PPE and safe procedures in clinical patient care is conducted in regular intervals. 6 Quality standards have been developed to ensure that necessary requirements for technical equipment and staff training are applied in all centers.
The treatment of HCID patients requires not only specialized knowledge of uncommon infectious diseases but also the ability to deliver intensive care treatment under high-level isolation conditions, given that most HCIDs carry a risk of deteriorating to multiorgan failure. This type of treatment is highly resource-consuming, especially considering the number of trained staff required for patient care.6,7 Prolonged care of HCID patients can easily overwhelm the staffing capacity of a single treatment center and may require the transfer of trained staff from other STAKOB treatment centers.
STAKOBanagement of HCIDs and Non -HCID EIDs
Over the past decade, STAKOB has managed several HCID cases in Germany, including SARS-CoV-1, Ebola virus disease, and Lassa fever. Most patients arrived in Germany by medical evacuation. In the following examples, we describe STAKOB’s management of single HCID cases in Germany and non-HCID EIDs across multiple countries.
Ebola Virus Disease in Germany in 2014
During the 2014-2016 West African Ebola virus disease outbreak, infections among healthcare workers were frequent. Three healthcare workers were evacuated to Germany in 2014 for further treatment, 2 of whom survived. The patients most likely benefited from the supportive intensive care treatment. Maintenance of IPC measures and use of ventilated full-body suits as PPE by staff providing care to patients prevented the spread of infections and protected medical staff. No secondary infection occurred.8‐10 Public health authorities made tremendous efforts to enhance emergency preparedness during the outbreak. In November 2014, a medical evacuation aircraft was assembled for performing comprehensive intensive care measures aboard, in cooperation with the Federal Foreign Office, RKI, Lufthansa, and members of STAKOB. It was eventually dismantled in 2015 due to decreasing case numbers of Ebola virus disease and high maintenance costs.11,12
Lassa Fever in Germany in 2016
The first recorded transmission of Lassa virus infection in Germany occurred in March 2016. A 46-year-old expatriate healthcare worker in critical condition was medically evacuated from Togo to Germany and died shortly after hospital admission in Cologne. The patient had been previously treated in Togo for malaria. The first postmortem examination did not reveal an underlying infectious cause, but a histologic examination suggested a viral disease. The subsequently conducted polymerase chain reaction of liver tissue confirmed Lassa virus infection. Sixty-two contacts to the index case were monitored in the states of North-Rhine-Westphalia, Rhineland-Palatinate, and Hesse, coordinated by the responsible competence centers. The contacts were categorized as being at high risk (zero), increased risk (33), moderate risk (17), or low risk (12). Domestic quarantine, twice daily temperature monitoring at home, and regular contact with the local public health department were implemented as public health measures. Six people developed mild symptoms consistent with a mild Lassa virus infection and were subsequently isolated. Ultimately, all 6 tested negative for Lassa virus. However, a mortician who handled the body of the primary case was infected with Lassa virus and admitted to the HLIU in Frankfurt, where he was treated successfully.13‐15
This example highlights the need for rapid diagnosis of HCIDs. Including HCIDs in the differential diagnosis was shown to be very important if a patient originates from an area where a certain HCID is endemic. To reduce the risk of further spreading, it is strongly advised to ensure proper IPC measures, such as the use of PPE whenever HCIDs cannot be ruled out. This Lassa fever case reveals the importance of early interagency communication and the imperative of a central coordinating body.
Multicountry COVID-19 Pandemic and Mpox Outbreak
While STAKOB’s focus was originally on HCIDs, the expert network has played an increasingly important role in emergency preparedness and response to non-HCID EIDs in recent years—including COVID-19 and mpox. In Germany, STAKOB was pivotal during the COVID-19 pandemic. Globally, a high degree of uncertainty characterized the initial public health response and clinical management of COVID-19 patients due to limited knowledge and lack of experience with the pathogen. During the early phase of the pandemic, the STAKOB expert network met regularly and exchanged knowledge with international partners, such as the National Emerging Special Pathogens Training and Education Center. The first COVID-19 patients in Germany were treated in STAKOB treatment centers. The centers participated in the first clinical trials on remdesivir and other new therapeutic approaches available in the country. STAKOB published the first COVID-19 clinical guidance for Germany, 16 shortly after the start of the pandemic in April 2020, based on its clinical experience, expertise in the management of EIDs, involvement in international partnerships, and a comprehensive literature review. Members of STAKOB participated regularly in the development of WHO global guidelines 17 and shared their expertise with peers at diverse healthcare settings in Germany through a series of virtual seminars.
During the mpox outbreak in Germany, STAKOB members served in leading roles to establish national clinical management standards for severe cases and provide guidance on IPC. STAKOB competence centers provided advice on aspects of the unclear infectiousness of the recent mpox strain, including the infectious period and classification of contact persons, as well as related issues such as the length of quarantine. The centers supported contact tracing at the local health department level and by assessing secondary cases and incubation times. 18
FUTURE CHALLENGES
While the STAKOB network established its relevance for Germany by providing expertise and guidance for HCID, it soon became recognized as an essential network providing specific guidance to support public health and clinical management of newly emerging pathogens. Its role is crucial given that outbreaks caused by highly pathogenic or new emerging pathogens are expected to occur in the future, although the frequency of these events cannot be predicted. 19
As the COVID-19 pandemic has shown, diseases with human-to-human transmission have the potential to spread rapidly in densely populated areas. The ongoing human expansion into wildlife habitats and other factors—such as urbanization, increased mobility of populations (travel, migration, displacement), and climate change—increase the risk of infectious disease occurrences outside of endemic areas.20‐22 In addition, the intentional release of highly pathogenic contagions in a bioterrorist attempt, for example, could lead to a large number of patients requiring treatment under isolation. Developing appropriate preparedness strategies to address such a scenario will require the expertise of a highly specialized network like STAKOB.
With the occurrence of HCIDs and outbreaks of non-HCID EIDs, public investments are required to maintain the appropriate level of preparedness and provide expertise and guidance. STAKOB treatment and competence centers face challenges related to the increasing difficulty of securing necessary funding for equipment and staffing of HLIUs in Germany. With increasing financial pressure on hospitals and a countrywide shortage of nursing staff, it is increasingly difficult to meet the requirements of regular training and exercises with external partners (fire departments, emergency medical services, police, airports, public health departments), which are needed to maintain Germany’s HLIU capacity. Urgently needed renovations and replacement of old facilities have been delayed due to a lack of funding. The maintenance of HLIU capabilities in Germany is currently endangered, at a crucial time when international networking is increasingly necessary and other countries are enhancing their HLIU capacities.
Conclusion
In recent years, the occurrence of HCIDs and outbreaks of non-HCID EIDs, such as COVID-19 or mpox, have demonstrated the essential role STAKOB plays in a public health response, particularly one aimed at mitigating special pathogens. This role is especially crucial in a changing global health landscape, with increasing threats conferred by, for example, climate change and the anticipation of emerging diseases.