
Abstract
Patients with high-consequence infectious diseases (HCIDs) require high-quality care by specially trained staff in a high-level isolation unit (HLIU) that follows strict infection prevention and control (IPC) measures. Caring for patients with (suspected) HCID is challenging, mainly because of the strict personal protective equipment (PPE) and IPC protocols healthcare workers (HCW) must adhere to for protection. The Radboud University Medical Center, located in Nijmegen, the Netherlands, has been a dedicated HLIU facility since 2008. A newly built HLIU opened in May 2022, and encouraged us to review the existing PPE selection, IPC protocols, and HCID training program to improve safety and comfort for HCWs working in the HLIU. Based on a systematic search through (inter)national HCID PPE guidelines and semistructured interviews with end users, we selected an improved, more comfortable set of PPE. Additionally, we developed a more concise and easier-to-use patient care process flow and implemented a new teaching strategy. The new way of working was tested in October 2022 when the first 2 patients with suspected HCID were admitted to our unit. We used surveys to evaluate the experiences of HCWs involved in this care to further improve the workflow of the unit. When optimizing safety and comfort for HCWs, it is important to consider (inter)national guidelines as well as user preferences. By systematically evaluating recent experiences of patient admission to the HLIU and then adjusting protocols and training, we can ensure that the quality of provided healthcare and the safety of HCWs working in the HLIU remains high.
Introduction
P
Strict IPC protocols and standards for PPE are essential to protect HCWs from exposure to highly infectious bodily fluids. Although standards have been developed to ensure that PPE is of sufficient quality to protect against HCIDs, 4 PPE have limiting factors, such as discomfort, reduced mobility, heat stress and dehydration, and communication barriers, that can affect routine use. 5 Also, strict IPC protocols often differ from those used in everyday settings, requiring HCWs to adapt to new PPE and practices. Additionally, HLIUs require HCWs who do not normally work together to immediately form an optimally cooperating team that can provide highly complex and safe care under very difficult circumstances. The risk of transmission of HCIDs to HCWs is considered very low if HCWs are properly trained in correct use of PPE, IPC procedures, and interdisciplinary collaboration.6-8 However, most training programs for HCWs involved in HCID care focus solely on procedures for donning and doffing PPE. The focus should shift from PPE use alone to include specific IPC procedures 9 and complex medical management of patients in critical conditions as well as collaboration with an interprofessional team.8,10
The Radboud University Medical Center (Radboudumc) is 1 of 5 designated HCID treatment and training centers in the Netherlands (Figure 1). Radboudumc has been taking care of patients with (suspected) HCID for more than 15 years, in a dedicated isolation room on the regular infectious diseases ward. Radboudumc HCWs involved in HCID care described their PPE as extremely warm and uncomfortable. Twice a year, they followed a training for donning and doffing of PPE, waste management, and cleaning and disinfection, but they were not optimally trained for specific HCID scenario skills or interprofessional collaboration. Also, the protocols guiding every step of a patient with a (suspected) HCID, from hospitalization to hospital discharge or death, were not always easy to navigate, especially when many different HCWs with different roles could be looking for different topics.
Map of the Netherlands. The Netherlands has 5 HLIUs (dark blue dots), 1 reference laboratory for HCID diagnostics (gray dot), and 3 dedicated ambulance teams for transport of patients with (suspected) HCID (black ambulances). Abbreviations: HCID, high-consequence infectious disease; HLIU, high-level isolation unit; MC, medical center; UMC, university medical center.
In 2021, Radboudumc built a new, separate HLIU designed to provide safe and high-quality care for patients with (suspected) HCID (Figure 2) and to serve as a training facility. The new HLIU has 2 ICU-equipped patient rooms and can be expanded with 2 additional patient rooms for non-ICU HCID care. Each patient room has 2 separate anterooms to allow for unidirectional flow: a clean anteroom for entering and a possibly contaminated anteroom for doffing and exiting. The new HLIU also has a point-of-care laboratory, where laboratory technicians can perform basic diagnostic tests in order to reduce the time it takes for results to become available. The HLIU has a dedicated ambulance entrance to facilitate easy transport to the patient rooms and to ensure that regular emergency care is not delayed when a patient with (suspected) HCID arrives. The lines on the floor of the anterooms visually indicate clean (green), possibly contaminated (orange), and contaminated (red) areas to clarify which PPE should be worn. Additionally, all protocols are depicted on multiple touchscreens in various rooms of the HLIU, giving HCWs easy access to all protocols, supported with pictures, to minimize the chance of errors. The units are also designed so that materials can be passed from one room to another through hatches to minimize walking movements and the number of exposed HCWs. To increase accountability and reduce error, a video assistant referee (VAR)—responsible for continuous video surveillance and communication from a central control room—was added to the HLIU team.
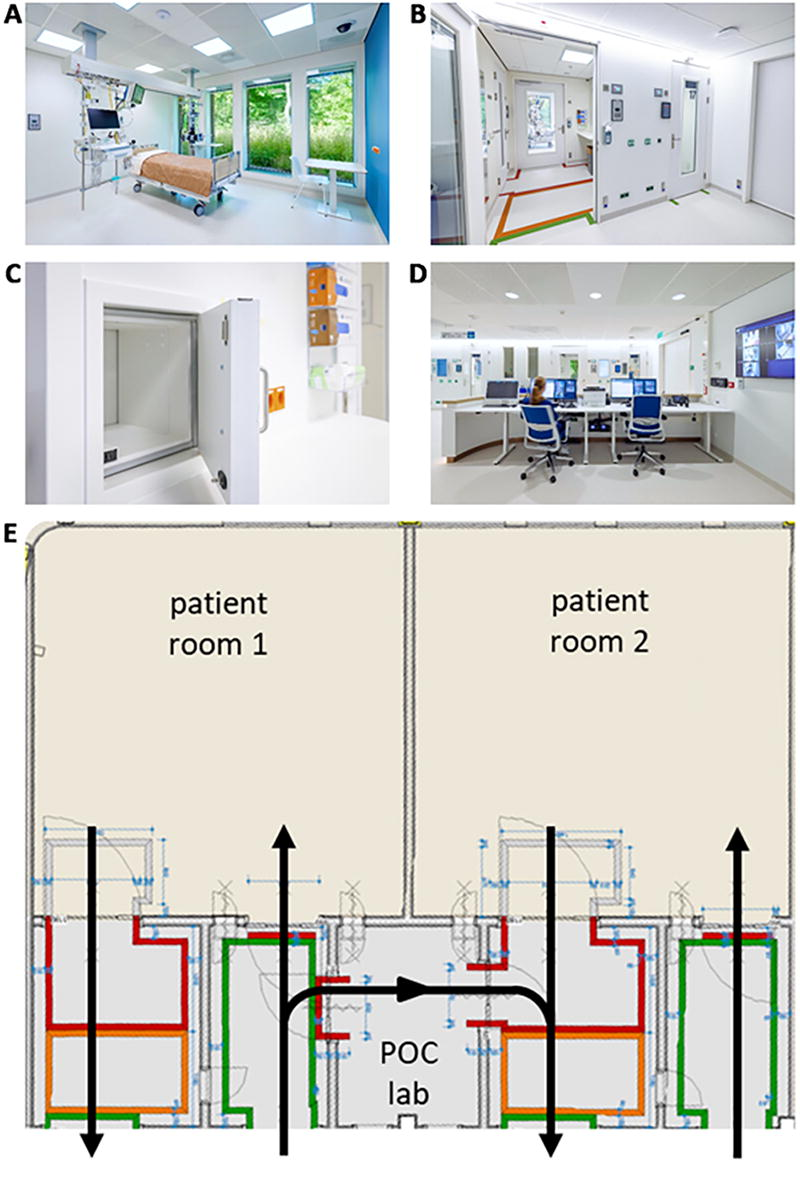
Images of the newly built Radboudumc HLIU. (A) One of the 2 ICU-equipped patient rooms; (B) outgoing anteroom with colored lines representing clean (green), possibly contaminated (orange), and contaminated (red) areas; (C) hatch that connects ingoing anteroom with patient room to pass materials; (D) control room for video surveillance and remote communication; and (E) map of the 2 patient rooms, point-of-care laboratory, and anterooms with unidirectional flow marked by colored lines on the floor indicating clean (green), possibly contaminated (orange), and contaminated (red) areas. Abbreviations: HLIU, high-level isolation unit; ICU, intensive care unit; POC, point of care.
The opening of the new HLIU in May 2022 encouraged us to revise (1) the current selection of PPE, to offer HCWs as safe and as comfortable a set of PPE as possible; (2) the IPC, diagnostic, treatment, and logistical protocols, to develop a more concise, easier-to-use patient care process flow; and (3) the training program, to adequately prepare HCWs for working in the HLIU. In October 2022, less than 6 months after the HLIU opening, the first 2 patients with suspected HCID were admitted, providing us with a unique opportunity to evaluate the updated HLIU practices.
Protocol and Training Program Revision
In preparation for opening the new HLIU, a team of professionals from the departments of internal medicine, medical microbiology, and IPC, and the Radboudumc Health Academy started to revise the existing work procedures and training program for HCWs who care for patients with (suspected) HCIDs.
Personal Protective Equipment
Over the course of 1 year, from February 2020 to February 2021, we systematically screened the guidelines for HCID PPE standards from the World Health Organization, 11 the European Centre for Disease Prevention and Control, 12 the Working Group on Infection Prevention of the Dutch National Institute for Public Health and the Environment, 13 and the Dutch Centre for Infectious Disease Control of the Dutch National Institute for Public Health and the Environment.14-16
To assess the preferences of HCWs regarding PPE, we conducted semistructured interviews from April to June 2020 with HCWs from the HLIU team—including doctors, nurses, and IPC experts—using open-ended and multiple-choice questions to collect feedback on the current selection of PPE and preferences for a new set of PPE.
In response to that feedback, we created a list of potentially suitable and available PPE that could be tested by our HCWs. From February through April 2021, we conducted a systematic search in catalogs from PPE suppliers, and requested that these suppliers collect all currently available PPE complying with the (inter)national HCID guidelines. Taking into account the feedback from the HLIU HCWs, we ordered a selection of PPE to be shipped to Radboudumc for testing.
At the end of April 2021, we organized 2 PPE fitting sessions. HLIU HCWs tested all of the available PPE and completed a structured survey with statements on comfort, safety, and time needed for donning and doffing. They assigned a number from 1 (completely disagree) to 10 (completely agree) to each of the survey’s statements. The results were analyzed descriptively.
Based on the survey results and the shelf life of the materials, we made a final selection of PPE for optimal safety and comfort. This new set of PPE was included in the revised PPE protocols for the new HLIU location.
Patient Care Protocols
Over the course of 14 months, from September 2020 to December 2021, tasks and actions were defined for each step of the HCID patient care work procedure for all involved HCWs and other hospital employees. The definitions were based on Radboudumc HCID protocols and brainstorming sessions with the HLIU management team, which consisted of an infectious diseases specialist, nurse, IPC expert, and researcher. Tasks were clearly identified for the following HCWs: doctors, nurses, radiographers, IPC experts, laboratory technicians, cleaning personnel, logistics employees, morgue attendants, and security personnel. Feedback from these HCWs on their tasks was requested, and, based on the feedback, a final process flow for care of patients with a (suspected) HCID was developed. The process flow was defined in close collaboration with the Radboudumc hospital document committee, which facilitates the development and actualization of hospital and patient-centered documents.
Training Program
In collaboration with the Radboudumc Health Academy, which is the Radboudumc education and training institute, the IPC unit and the department of internal medicine developed a new training program for HCID care.
The request of the IPC unit and the department of internal medicine for an improved training program was analyzed by 2 learning and development advisors at the Radboudumc Health Academy, using the following 2 methods: (1) Kessels’ “eight fields instrument,” 17 which is an analysis framework for examining learning processes in organizations; and (2) the “seven basic principles of learning in organizations,” 18 which facilitate a search within the broad field of learning theory to achieve a better match between an organization’s requests and appropriate development strategies. The learning and development advisors attended current HCID trainings and conducted semistructured interviews with HCWs from the HLIU team to define the current and desired competencies. Based on the analyses, observations, and semistructured interviews, a new training program was developed.
Evaluation of First Patients Admitted to the New HLIU
Two patients with suspected viral hemorrhagic fever were admitted to the new HLIU on October 9 and 10, 2022. Both patients eventually tested negative for pathogens causing viral hemorrhagic fever. The following month, HCWs involved in the care of these 2 patients received an invitation to fill out an online survey covering the following topics: (1) comfort and safety of the new set of PPE, (2) innovative aspects of the newly built HLIU, (3) perceived safety regarding IPC, (4) communication between HCWs, and (5) comparison of the new HLIU to the former ward (only for HCWs who had worked in the previous HLIU). All survey topics included statements that were graded on a scale from 1 (completely disagree) to 10 (completely agree). Data were analyzed descriptively. Comments from the open text fields were summarized.
Findings
PPE Fitting Sessions
Table 1 depicts the results of the systematic search through international HCID PPE guidelines, the semistructured interviews on PPE preferences with the HLIU deployment team, and the final selection of PPE. We interviewed 16 HLIU end users: 3 doctors, 9 nurses, 2 members of the cleaning department, 1 member of the purchasing department, and 1 IPC expert. Overall, the HCWs interviewed preferred PPE that feels less warm and a donning and doffing procedure with as few actions as possible, to minimize the chance of errors.
Minimal Requirements for HCID PPE Based on International Guidelines and Semistructured Interviews With End Users and Final PPE Selection by Radboudumc
Abbreviations: CID, Dutch Centre for Infectious Disease Control; ECDC, European Centre for Disease Prevention and Control; EN, European Norm; HCID, high-consequence infectious disease; HLIU, high-level isolation unit; ISO, International Organization for Standardization; NEN, Nederlandse Norm (Dutch norm); PAPR, powered air purifying respirator; PPE, personal protective equipment; WHO, World Health Organization; WIP, Dutch Working Group on Infection Prevention.
We then invited 23 end users to PPE fitting sessions. Of these, 11 (47.8%) participated and evaluated the PPE: 1 doctor, 6 nurses, 2 members of the cleaning department, and 2 radiographers. The findings from these fitting sessions follow.
Coveralls and Cover Boots
During the fitting sessions, 3 types of coveralls were tested: the currently used 3M Protective Coverall 4565 and the Dupont Tyvek 500 Labo and Tyvek 600 Plus, of which the latter 2 have integrated boots. Although the fabric of the Tyvek coveralls scored higher for comfort compared with the 3M coverall, the integrated boots did not have the expected effect of decreased donning and doffing time compared with the separate 3M cover boot. Additionally, the Tyvek boots were slippery on a smooth surface, which increased the risk of falling (Figures 3A and 3B). The 3M Protective Coverall 4565 was thus retained in the new set of PPE.
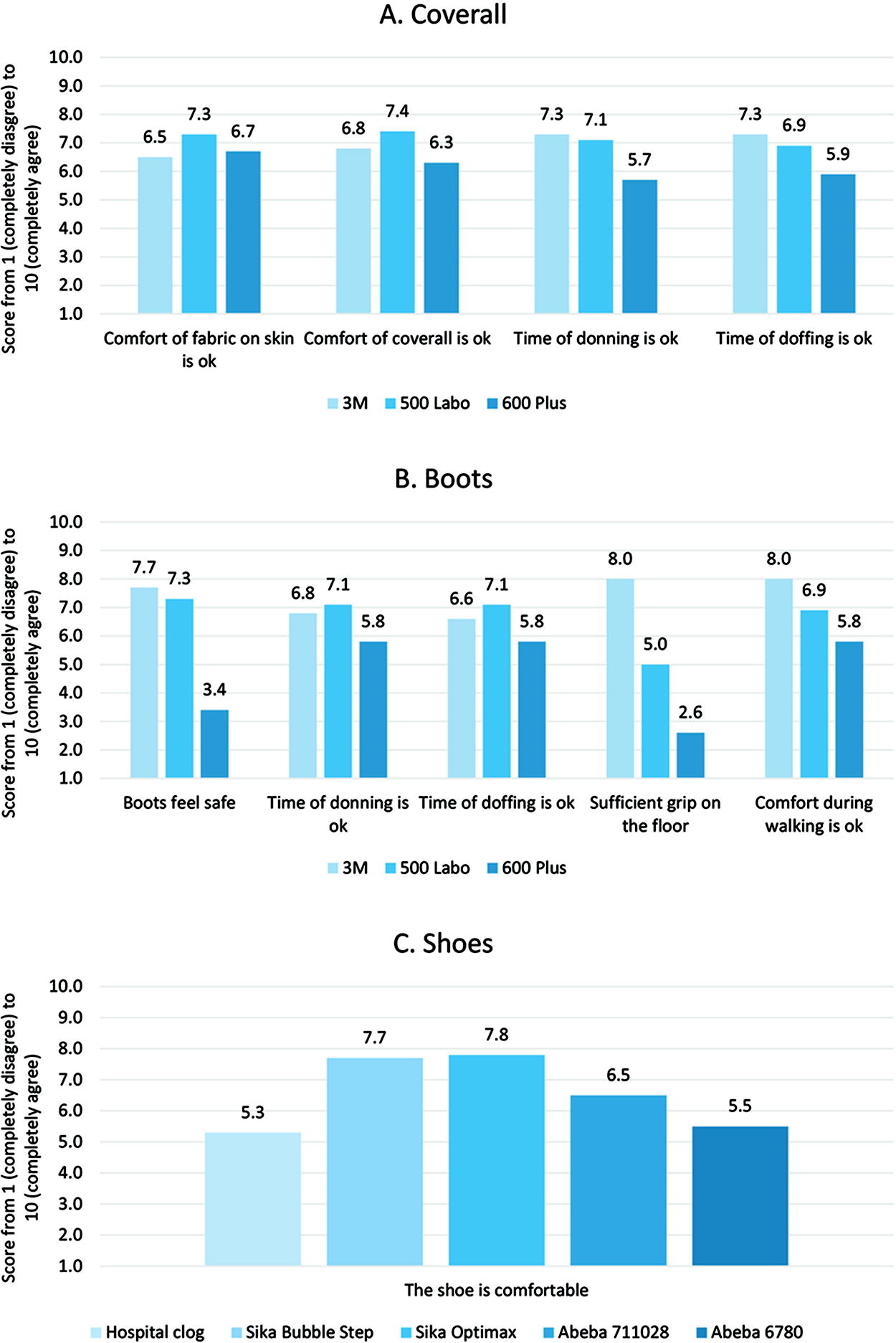
Mean scores (N=11) for comfort and safety of (A) coveralls, (B) boots, and (C) shoes during the PPE fitting session. Statements were graded on a scale from 1 (completely disagree) to 10 (completely agree). Abbreviation: PPE, personal protective equipment.
Shoes
Five different shoes were tested: the currently used hospital clogs, Sika Bubble Step, Sika Optimax, Abeba 6780, and Abeba 711028. Clogs were not preferred by either the HCWs or the IPC experts, because some HCWs lose their clogs in their coverall and are put at risk of falling. Both the Sika shoes scored higher than both Abeba shoes regarding experienced comfort (Figure 3C). The Sika Bubble Step is a lace-up shoe and the Sika Optimax is a slip-on shoe, and 5 HCWs had experienced losing the heel of the shoe of the Sika Optimax while walking. Therefore, the Sika Bubble Step was chosen for the new set of PPE.
Tape Test
During a tape test, the bottom layer of gloves was not taped to the coverall, in contrast to current practice (which aims to prevent exposure of the wrist). Not taping the bottom layer of gloves resulted in exposure of the naked skin of the wrist when changing the top layer of gloves.
Cooling Vest
One cooling vest (the INUTEQ PCM CoolOver 21C) was tested during the fitting session. This cooling vest was already used by Radboudumc employees for care of large numbers of patients with COVID-19. Although some end users experienced the cooling vest as too cold during the first few minutes after donning, they could imagine it would help against heat stress when working in the PPE for a longer period of time.
Isolation Gown
No alternative isolation gown was found that was both water resistant and nonsterile, and therefore the currently used isolation gown was retained.
Powered Air Purifying Respirator
We reviewed different powered air purifying respirators (PAPRs) online. However, PAPRs are costly, and because Radboudumc already owns 11 of them, the decision was made to wait to change to new PAPRs. Meanwhile, no cheaper hood was found that was both compatible with the currently used 3M PAPR and complied with the international standards for HCID. The current PAPR makes a lot of noise, which hampers communication. Therefore, a specially designed headset with communication device (Entropia Critical Concepts NV, Belgium) was developed to enable HCWs in the same room to communicate with each other as well as with the VAR, without being disturbed by conversations in the anterooms or the laboratory. Using this communication system, the VAR, who performs camera surveillance from a distance, can listen and talk to all HCWs in the patient rooms, point-of-care laboratory, and anterooms.
Revised PPE Set
The final set of PPE (Figure 4) was selected based on national and international guidelines and our interviews and fitting sessions with end users. The employees working in this set of PPE are HCWs who work in the HLIU patient rooms and laboratory technicians who work in the point-of-care laboratory. The HCWs are assisted in donning and doffing the PPE by specifically trained buddies who also wear appropriate protection.
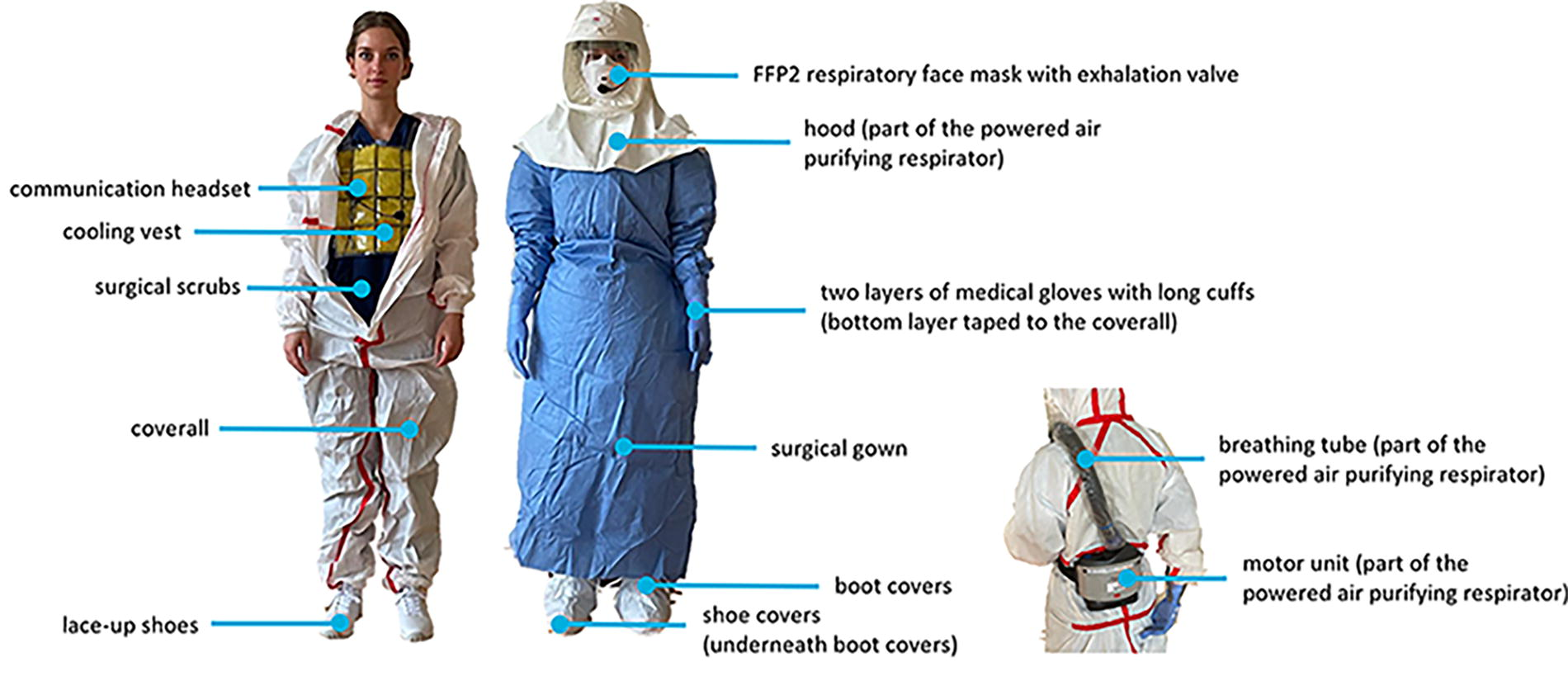
Final selection of PPE for HCWs entering Radboudumc HLIU patient rooms or working in the point-of-care laboratory room. Abbreviations: FFP, filtering facepiece particle; HCWs, healthcare workers; PPE, personal protective equipment.
Patient Care Protocols
The brainstorming sessions with the HLIU management team resulted in the following requirements: protocols should be (1) in chronological order, (2) stratified per role, and (3) easily accessible. In collaboration with the hospital document committee, this resulted in a newly developed HCID process flow that describes every step of HCID care chronologically, from hospitalization of a patient with (suspected) HCID to hospital discharge or death (for flow map detail see Figure 5; for the full process flow map, see Supplementary Figure S1, www.liebertpub.com/doi/suppl/10.1089/hs.2023.0147). Each step involves tasks that are clearly assigned to 1 or more HCWs specifically. Each profession and/or department is assigned a unique color, which makes it easy for end users to recognize when and where in the process they are involved. The steps in the process flow are linked to specific protocols. Based on the HCWs’ feedback, unique “function cards” were developed for each role, in which the personal tasks for the HCW in that role are described in chronological order. The newly developed HCID process flow is accessible to all employees through Radboudumc’s internal document system using Zenya software (Infoland BV, the Netherlands).
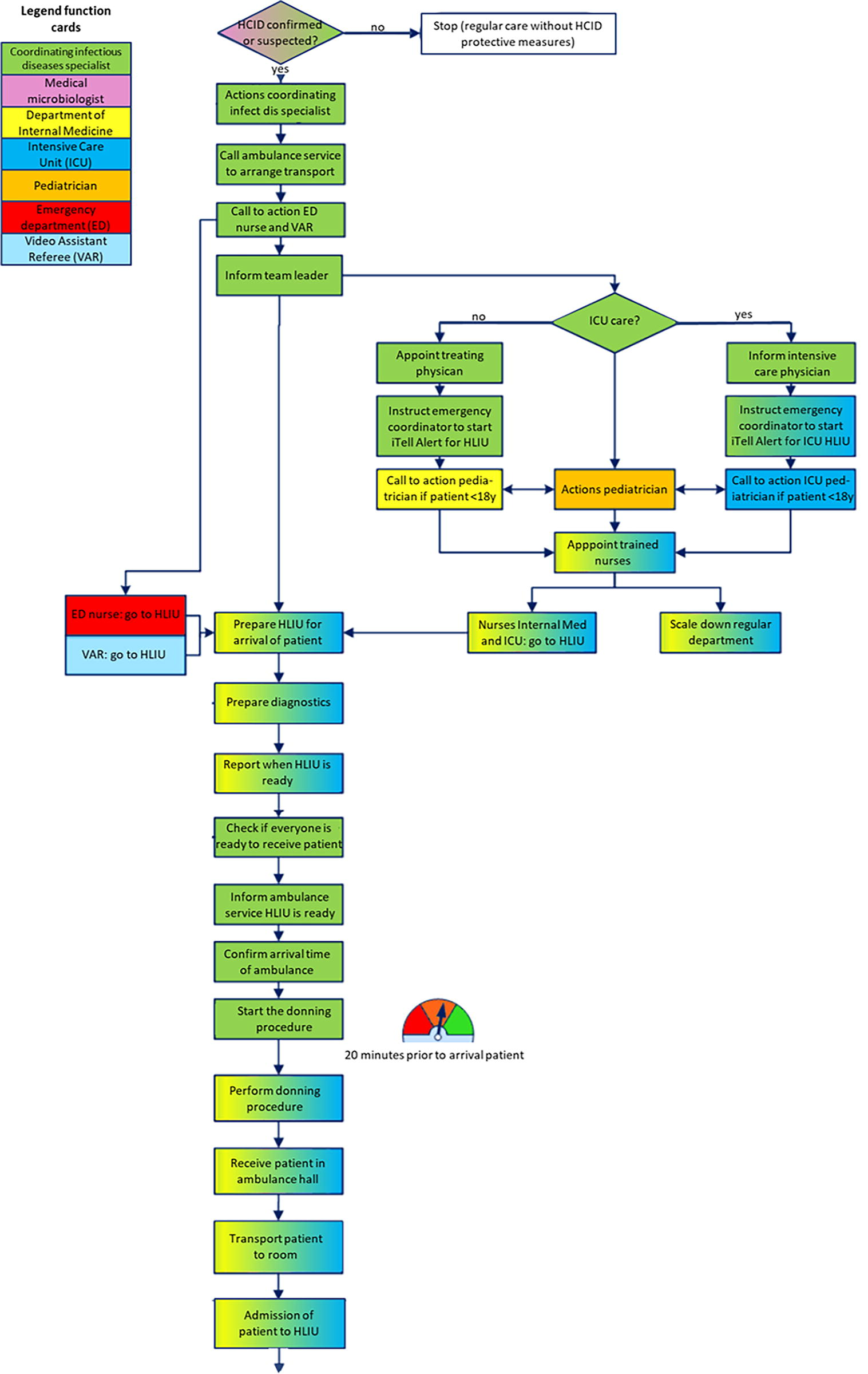
Highlighted section of the revised process flow for care of patients with (suspected) HCID. This section shows an overview of all actions that need to be taken to prepare the HLIU for admission of the patient. Each action is colored according to the responsible department and/or profession. The full image of the process flow, showing all actions that need to be taken with a patient with (suspected) HCID from hospitalization through hospital discharge or death is available as a Supplementary Figure S1 (www.liebertpub.com/doi/suppl/10.1089/hs.2023.0147).
Training Program
The 2 methods of analysis resulted in the following preferences for the new training program: (1) training in interprofessional collaboration; (2) just-in-time training that includes easy, accessible job aids, tools, and information; and (3) training options for working with a dedicated team, that is trained regularly, and for working on a flexible team, that is trained on the spot if necessary. In total, we interviewed 7 HCWs (2 doctors, 3 nurses, 1 member of the cleaning department, and 1 radiographer). Based on the semistructured interviews, we formulated competencies that would need to be acquired, such as skills for how to safely work in and follow the procedures of the new HLIU, don and doff the PPE, use the IPC procedures, and communicate efficiently. Interdisciplinary team, e-learning, specific skills, ambulance, and just-in-time trainings were added to the final training program (Table 2). This new training program is continuously evaluated and improved according to the plan-do-check-act cycle. 17
Current Required Training and Learning for HCW on the HLIU Team
Abbreviations: HCID, high-consequence infectious disease; HLIU, high-level isolation unit; HCW, healthcare workers; IPC, infection prevention and control; PPE, personal protective equipment; VAR, video assistant referee.
Evaluation of First Patients Admitted to the New HLIU
On October 9, 2022, 2 patients who had recently traveled to Uganda were suspected of Ebola virus disease or Crimean-Congo hemorrhagic fever and admitted to our unit. The dedicated team was called in via the iTel Alert system for the first 8-hour shift. HCWs for subsequent shifts were scheduled by the planner as depicted in Supplementary Material (www.liebertpub.com/doi/suppl/10.1089/hs.2023.0147). During a single shift, nurses alternately fulfilled different roles in the following fixed order: (1) caring for the patient in full PPE, (2) buddy for doffing, and (3) buddy for donning. After working in full PPE, it is obligatory to rest before working as a buddy. After negative polymerase chain reaction tests were received from the national reference laboratory, both patients were discharged. A survey was sent afterward to all 35 staff involved in the care of these 2 patients, of whom 23 (65.7%) responded: 4 doctors, 13 nurses, 2 VARs, 2 IPC experts, 1 laboratory technician, and 1 member of the cleaning team. The respondents used a scale (from 1 for completely disagree to 10 for completely agree) to respond to the survey statements. The mean results are shown in Table 3.
Mean Survey Responses From HCWs Who Cared for the First 2 Patients in the New HLIU (N=23)
The mean score was graded on a scale from 1 (completely disagree) to 10 (completely agree).
Response from only 1 laboratory technician working in the point-of-care lab.
Nearly half (n=11, 47.8%) of the HCWs had worked at the former infectious diseases ward.
Abbreviations: HCW, healthcare worker; HCID, high-consequence infectious diseases; HLIU, high-level isolation unit; IPC, infection prevention and control; POC, point-of-care; PPE, personal protective equipment; VAR, video assistant referee.
The HCWs felt safe in the new set of PPE, and scored the comfort of the PPE at 6.0. The cooling vest contributed cto experiencing less heat stress. Most of the innovative aspects of the new building were considered user-friendly and as contributing to a safer working environment. The hatches scored lowest (7.9) because the procedure for using them was not clear to all HCWs. The perceived safety regarding IPC was high overall; it received the lowest rating from the laboratory technician (n=1), whose buddy once deviated from the doffing protocol. (The laboratory technician remarked that he “was not scared to be contaminated, but would have felt safer if the buddy followed the protocol.”) The new communication devices, under the control of the VAR, improved communication, although the clarity of communication could still be improved. The average score when comparing the HLIU with the former infectious diseases ward was 8.7, suggesting that HCWs agreed that the new HLIU is safer and more pleasant than the former ward for patients with (suspected) HCID.
Discussion
In this study, we have evaluated the work procedures and training program of our newly built HLIU. PPE materials were selected upon considering (inter)national HCID guidelines and the preferences of end users. Our HCWs preferred a coverall with integrated boots to reduce donning and doffing time, but we did not find a proper coverall with integrated boots. During the PPE fitting, these coveralls either had a longer donning and doffing procedure than the current coverall with separate boot covers or were slippery on the floor. Therefore, the currently used 3M boot covers were kept. Hall et al 19 had previously found that separate boot covers are a frequent cause of cross-contamination and carry an unacceptable risk during doffing when HCWs use scissors to remove them. During our doffing procedure, however, the boot cover is removed without scissors, and not by the HCW themself but by a buddy who wears protective clothing. We did not use fluorescent solution to assess the risk of self-contamination of HCWs during PPE removal.20,21
The European Centre for Disease Prevention and Control mentions that no sharp objects are allowed to remove tape. When taping gloves to the coverall linearly, and not circularly, sharp objects are not needed for doffing, and the wrists remain protected. Although a cooling vest was integrated into the new set of PPE, working in the PPE can still cause heat stress and fatigue. Little is known about the maximal time in which a HCW can wear PPE, safely provide care for a patient, then safely perform the doffing procedure. 22 We recommend conducting a local risk assessment 23 and implementing a maximal time in which HCWs are allowed to work in the PPE.
Structuring multidisciplinary care protocols in the HLIU setting is important, because in the event of an unexpected patient, professionals who do not normally work together must immediately form an optimally performing team and provide highly complex and safe care under very difficult circumstances. We were able to structure numerous protocols in a patient care process flow. Such protocols should be assessed frequently to identify deviations and improve performance and compliance. 24 Our process flow focuses mainly on work procedures inside our hospital, and collaboration with first responders and public health can be further improved. 25 We recommend designing a process flow in collaboration with dedicated ambulance services and public health services.
The Radboudumc training program was revised to include specific IPC procedures along with collaboration and communication in multidisciplinary teams. Training is time- and resource-intensive, and it was difficult to balance the available time and resources of our HCWs with the requirements for adequate preparation, which is a known problem among other HLIUs.26,27 We plan to assess the impact of the trainings with pretraining and posttraining surveys 10 ; until then, we cannot yet conclude whether the new training program improves preparedness and competence.
Based on the evaluation of the admission of 2 patients with suspected HCID, we conclude that the patient care provided was safe and of high quality and that the risk of contamination was negligible. Some points of improvement were identified. Not all HCWs knew how to safely work with the unidirectional flow of the hatches, and this increases the chance of deviation from procedure and potential contamination of the anteroom. 28 The way HCWs communicated via the communication devices was not always optimal. Communication using the specially designed system demands high discipline. 10 We recommend paying extra attention to adherence to IPC protocols and communication discipline in trainings. Additionally, some protocols were adjusted and improved after the evaluation.
A strength of this study is the systematic evaluation of multiple work procedures that included all important stakeholders. Additionally, the expertise of a hospital document committee and a learning and development advisor is a prerequisite for complex protocol revision and training development, respectively. The admission of the first 2 patients provided a unique opportunity to evaluate and further improve work procedures soon after opening our new HLIU.
Our study had several limitations. The COVID-19 pandemic limited our PPE fitting sessions. We were able to receive only a limited selection of PPE from suppliers due to worldwide PPE shortages, and there was a relatively low response rate to the fitting sessions because HCWs had to work in COVID-19 care instead. We did not assess the risk of self-contamination of the new set of PPE. The response rate for the evaluation of the care of the 2 patients with suspected HCID was good (66%), but it could have been higher if the survey had been shared sooner after discharge of the patients (eg, within 1 week rather than 1 month). We therefore recommend having a standard evaluation survey ready for distribution. In addition, the fact that both patients tested negative for viral hemorrhagic fever might have affected the HCWs perceived safety afterward.
Healthcare systems and facilities vary between and even within countries, and HLIU operational policies and work procedures cannot be completely standardized. This approach is therefore not directly transferable from 1 HLIU to another, but it offers tips and tools for others to use. Other challenges in HCID care remain but are not discussed here, such as staffing, safe patient transport, possible interventions such as surgery, and admission of special groups like children. Developments in HCID care continue, and an (inter)national platform is needed to share best practices and discuss future challenges.
Conclusion
Taking care of patients with (suspected) HCID is challenging, and HLIUs are responsible for being prepared to provide high-quality care. Being optimally prepared as an HLIU is a continuous process, and future challenges will arise: increased international travel contributes to more outbreaks of HCIDs or potentially new, yet-unknown pathogens. When optimizing safety and comfort for HCWs caring for patients with HCIDs, it is important to take account of (inter)national guidelines as well as HCWs’ preferences. By systematically evaluating recent experiences of admission of patients to the HLIU, followed by adjustment of protocols and trainings, the quality of provided healthcare and safety of HCWs working in the HLIU will remain high.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.