
Abstract
The public health workforce continues to experience staff shortages, which hampered the ability of US state, tribal, local, and territorial health departments to respond to the COVID-19 pandemic. In April 2020, the US Centers for Disease Control and Prevention (CDC) awarded $45 million to the CDC Foundation to provide field assignees to support these health departments. To expand these efforts, the CDC provided an additional $20 million in May 2021 for vaccination efforts and $200 million in June 2021 to support COVID-19 response and general infrastructure support. The CDC Foundation worked with jurisdictions across the United States to develop job descriptions based on need and recruit nationally for positions. This expanded project, called the Workforce/Vaccine Initiative, hired 3,014 staff in 91 jurisdictions, with 2,310 (77%) hired by January 2022. Most assignments were fully remote (55%) or hybrid (28%). The largest number of staff (n=720) supported COVID-19 response work in schools. Other common functions included contact tracing/case investigation (n=456), program coordination (n=330), epidemiology (n=297), data and surveillance (n=283), and administrative support (n=220). To advance health equity and improve response efforts, 79 health equity staff were assigned to 30 jurisdictions. To support the needs of tribes, 76 field staff supported 22 tribal entities. This project demonstrated the important role of a flexible, centralized approach to rapid placement of staff in public health departments during an emergency response. While the goal of the Workforce/Vaccine Initiative was to meet short-term staffing needs, lessons learned could provide insights for building a sustainable and scalable public health workforce.
Introduction
The public health response to the COVID-19 pandemic by US state, tribal, local, and territorial public health departments was challenged by a lack of sufficient public health infrastructure. 1 Causes for the declining infrastructure have been attributed to underfunding of health departments and departure of staff from the workforce.2,3 A survey by the Association of State and Territorial Health Officers reported that the number of public health workers in states had declined by 6,000 positions or 6.7% between 2016 and 2019. 4 Public health expenditures also fell between 2010 and 2018. 5 The pandemic increased demand for core response staff, particularly contact tracers, case investigators, epidemiologists, public health nurses, and communications staff. Many health departments met this demand by redirecting other governmental staff within their health department to response roles6,7; however, the prolonged nature of the pandemic made this solution problematic.
Many state, tribal, local, and territorial health jurisdictions faced hurdles in hiring new staff. 6 These hurdles included the inability to hire staff quickly through contracting mechanisms, lack of human resource capacity to recruit and hire staff, legislative barriers to hiring without prior approval, and inadequate budgets to hire additional staff. Public health departments also needed to recruit and hire staff with new or specialized skills who were often hard to find, 6 such as skilled specialists in informatics, laboratory science, advanced epidemiology, communications, public health nursing, and legal issues.
The CDC Foundation has many years of experience hiring field assignees for both privately and federally funded activities. In 2018, for instance, the US Centers for Disease Control and Prevention (CDC) supported the Foundation's recruitment and employment of 98 field assignees in 13 health departments to assist states' opioid crisis response. In April 2020, the CDC Foundation received funding from a private donor that supported 237 positions in 16 health departments for COVID-19 response work. In May 2020, the CDC Foundation received funding from the CDC that filled more than 800 field assignments in 84 jurisdictions to meet the demand for increased numbers of public health staff to respond to the COVID-19 pandemic. These opportunities provided the CDC Foundation with real-world experience in swift recruitment, hiring, and management of staff needed to support the COVID-19 response.
The CDC awarded additional funds to the CDC Foundation to support vaccination efforts ($20 million) in May 2021 and the ongoing COVID-19 response ($200 million) in June 2021. Each of these funding streams was for 1 year. This case study describes how the efforts from these 2 funding streams, called the Workforce/Vaccine Initiative, resulted in the hiring of more than 3,000 staff in state, local, tribal, and territorial jurisdictions, supported COVID-19 response efforts, and bridged workforce gaps.
Methods
Data for this case study were extracted from human resource datasets and supplemented with information from CDC Foundation field assignee managers. All data were managed in Microsoft Excel. After the hiring period ended in June 2022, we administered a questionnaire on field assignee work experience and feedback using Smartsheet in August 2022. All questionnaire data were maintained in Smartsheet. Participation was voluntary, and responses did not include identifying information. Respondents were asked to complete the questionnaire within 1 month. Jurisdictional points of contact provided feedback to CDC Foundation managers throughout the project and assimilated it into internal reports at the end of the project.
Project Description
Using the model developed for previous hiring efforts, the CDC Foundation recruited and hired staff who were assigned to public health jurisdictions nationwide. Public health jurisdictions included state, tribal, local, and territorial health departments and organizations. Initially, a core set of standardized positions were hired that were common to public health departments (eg, contact tracers, case investigators, public health nurses, epidemiologists, data and communication specialists) and needed for response activities. The initial staffing request from jurisdictions in the Workforce/Vaccine Initiative started as COVID-19 cases were rising, before the Omicron wave 8 and the approval of vaccines for children ages 5 to 11 years. 9 As the pandemic evolved, positions were customized to meet shifting needs, which included the creation of specific positions as required by jurisdictions. After vaccines were approved, specific positions were recruited for and filled to support the development and implementation of vaccination efforts in adult and pediatric populations, increase testing and case investigation in schools, and advance health equity for community support and education projects.
The CDC Foundation developed more than 200 job descriptions based on jurisdictional needs and recruited nationally for the positions, with the intention that most positions would be remote, meaning that all work could be done from home. Recruitment efforts were conducted using a tiered approach that involved advertising, networking and sourcing through multiple channels, focusing specifically on hard-to-fill positions, working with experienced and specialized recruiters, posting on social media, and using a national recruitment strategy that involved establishing a pool of candidates for certain core positions. The CDC Foundation compiled a list of 66 professional associations and job hosting sites for targeted recruitment of specific job categories (eg, public health nurse, epidemiologist, laboratory scientist, informatician and communication specialist).
CDC Foundation staff screened approximately 9,800 applications and interviewed more than 5,800 candidates. Staff from jurisdictions requesting an assignment participated in interviews and identified the candidates that best matched their needs.
All staff were hired as CDC Foundation employees and eligible for full benefits. Salaries were competitive and reflected the short-term nature of the assignment, which sometimes resulted in higher salaries for CDC Foundation field assignees than for permanent positions in health departments. The field assignees were assigned to a CDC Foundation manager and a jurisdictional point of contact. The CDC Foundation managers performed administrative functions, such as assuring equipment needs were met, signing timecards, approving requests for time off, and addressing performance issues. Jurisdictional points of contact provided guidance to the field assignees including work assignments, training specific to the job, and orientation to the public health organization or entity.
The CDC Foundation management team recruited, hired, and managed field assignees and provided project oversight. The team also hired 55 regional managers who served as a conduit between the Foundation and jurisdictions, working with local points of contact to ensure smooth transitions for the new field assignees into the local environment. In addition, 8 area managers supported the regional managers and provided an additional link to jurisdictional points of contact and public health leadership. Core CDC Foundation staff provided support in areas related to human resources, information technology (IT) and equipment, communications, legal issues, budgeting, finance, and compliance.
Project Results
Description of Staff
With the $220 million in CDC funding for the Workforce/Vaccine Initiative in 2021, a total of 3,014 staff were hired in 91 jurisdictions, with 2,310 (77%) hired by January 2022. Hiring ended in June 2022. As shown in Figure 1, staff were assigned to all 50 states, 15 local health departments, 4 territories, and 22 tribal entities. The number of staff hired for state, tribal, local, and territorial health jurisdictions ranged from 1 to 273 (Figure 2).
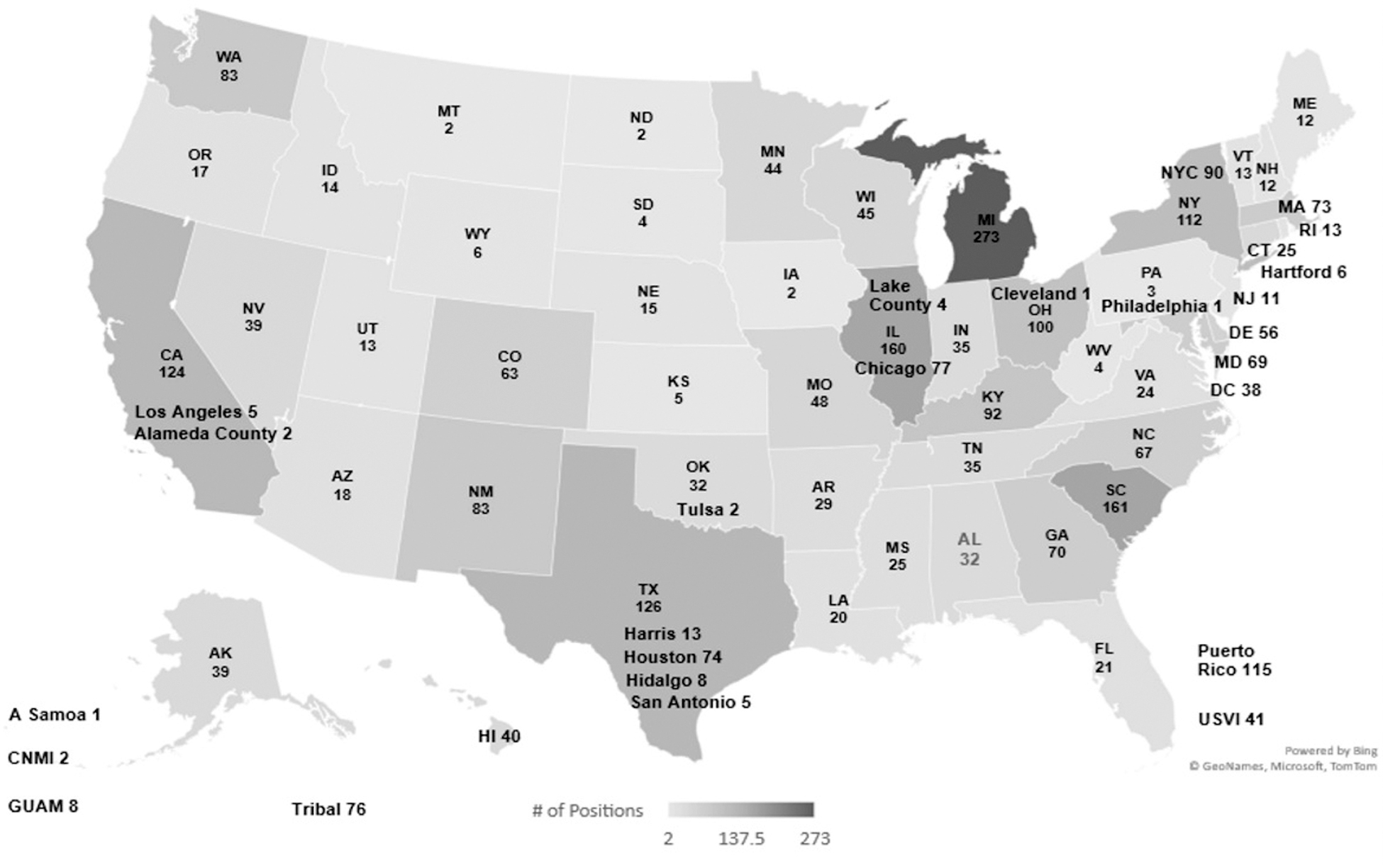
Allocation of 3,014 Workforce/Vaccine Initiative field assignees across US states, territories, and tribal entities.
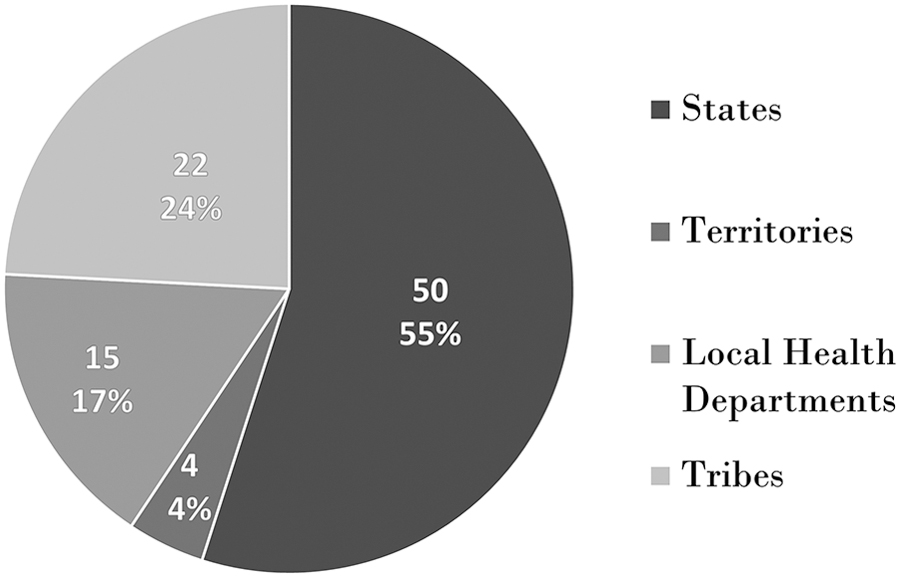
Distribution of Workforce/Vaccine Initiative field assignees among the 91 jurisdictions, by jurisdiction type.
Epidemiologists, nurses, and case investigators were essential for case investigation, response to outbreaks (including those in congregate care settings), infection control efforts, as well as data collection, analysis, and reporting. In addition to traditional public health staff, jurisdictions required administrative staffing for human and financial resources and legal support for contracts and other legal issues. Communications staff developed public facing materials for vaccines tailored to the local context. Table 1 shows the number of positions filled by category.
Categories of Workforce/Vaccine Project Field Assignee Positions (N=2,991)
Note: This table does not include 23 positions that lasted less than 1 week.
Health equity staff were needed for both outreach and mitigation interventions targeting specific at-risk communities. Data analysts, IT specialists, and others were hired to support data dashboards and build interfaces with healthcare facilities for transfer of health data as well as provide analytics for case investigations, vaccine registries, and overall surveillance needs.
The majority of assignments for the Workforce/Vaccine Initiative were fully remote (55%) or hybrid (28%) (ie, in the office 1 to 2 days per week). Only 522 (17%) were hired to work onsite at the assigned jurisdiction. Onsite positions usually had in-person responsibilities extending into the community (eg, community health workers, public health nurses, school liaisons).
Support of Focused Activities
We reached out to jurisdictions in October 2021 to gauge their interest in receiving field assignees to support public health efforts in schools—approximately 30 jurisdictions expressed an interest. In response, about 24% (n=720) of all field assignees were hired to work specifically with schools as school liaisons, public health nurses, and disease interventionists in 27 jurisdictions. School-based support included work in communications, COVID-19 testing and case investigations, support of vaccination programs, and development of school guidance and policies.
To support the needs of federally recognized American Indian/Alaska Native tribes, CDC Foundation staff met with tribal leaders, area Indian health boards, and tribal consortia to discuss the opportunity and to identify positions that would provide the most benefit to tribes. The ability to customize positions enabled the project to focus on the needs and challenges identified by tribes. Priority was given to applicants with tribal experience or tribal affiliation. Overall, 76 field assignees were assigned to 22 tribal entities, including 13 individual tribes, 7 area Indian health boards, and 2 tribal consortia (Table 2). The number of assignees per entity ranged from 1 to 19, with half of the entities (n=11) having 1 field assignee. The top 5 position types were case investigator (n=24), contact tracer (n=8), epidemiologist (n=5), communication specialist (n=5), and public health nurse (n=3).
Field Staff Assignments to Tribal Organizations
To advance health equity in public health, 79 positions were hired in 30 jurisdictions to build capacity to implement programs, services, and strategic actions to improve health disparities. In some jurisdictions, CDC Foundation assignees were the first staff hired to focus specifically on health equity, work with specific communities on COVID-19, and implement strategies to increase access to COVID-19 vaccines.
In August 2022, after the hiring period ended, project leadership reached out to field assignees and requested that they complete a questionnaire on their positions and provide feedback on their work experience. When the questionnaire was administered, a large percentage of field assignees (44%), including contact tracers, case investigators, and school staff, had completed their assignments and were no longer employed by the foundation. Of the 1,700 field assignees, 608 (35%) who were employed at that time responded. Of those who responded, 332 (55%) reported that it was their first experience working in governmental public health (Figure 3). Of these, 286 (86%) expressed an interest in continuing to work in this area.
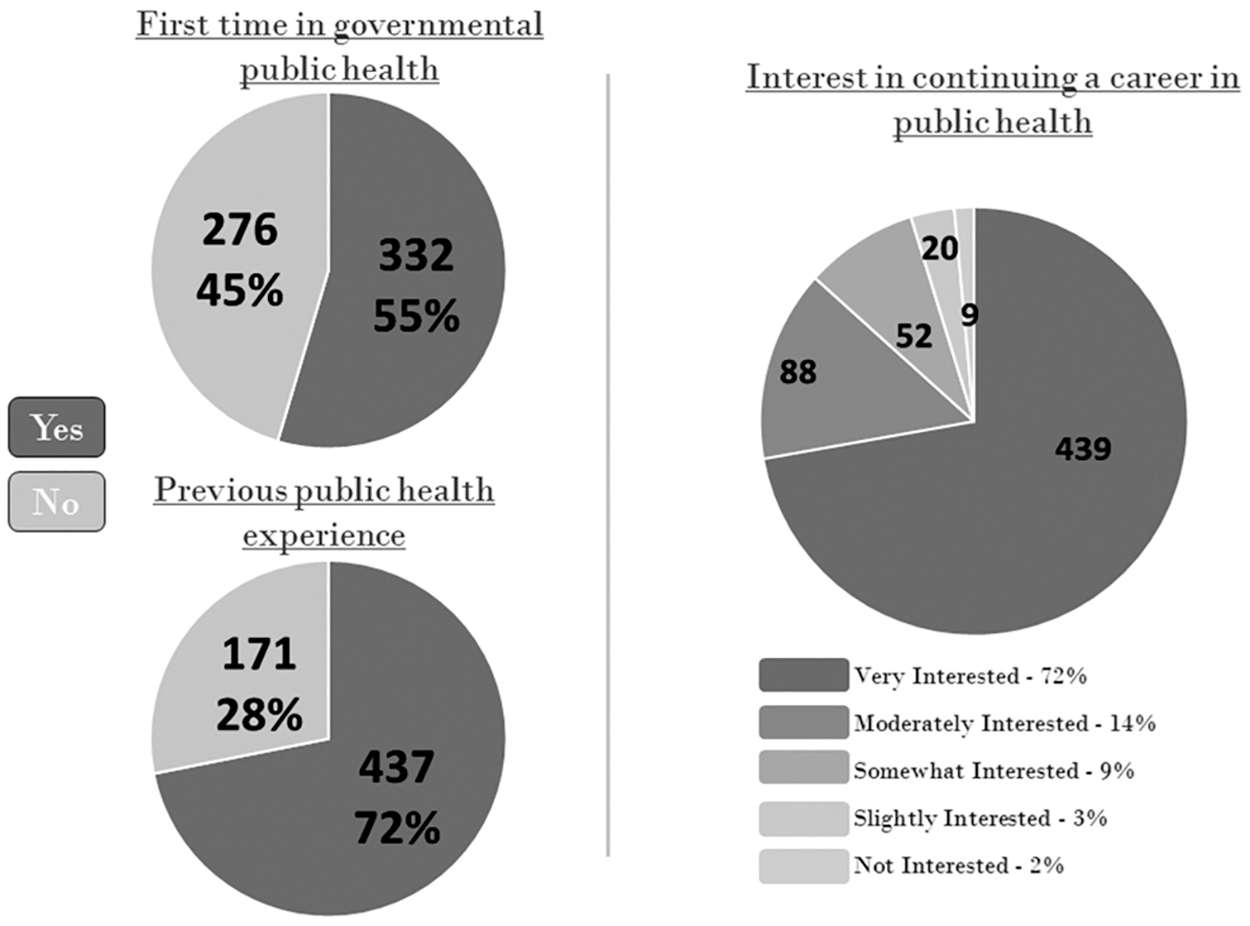
Public health experience and career interests of Workforce/Vaccine Initiative field assignees (N=608).
Impact of Field Assignees
Throughout the project, CDC Foundation managers received feedback from jurisdictional leadership on the impact of the project. Jurisdictions appreciated not having the administrative burden of recruiting and hiring staff. The foundation was also able to address other challenges facing jurisdictions, including difficulties related to crafting new positions for specific jobs needed for the response or limits in hiring retirees.
Many health departments noted the high caliber and strong technical expertise of field assignees. Qualified staff were especially important in positions that required specific skills, such as positions involving laboratory science, IT, epidemiology, nursing, communications, data analytics, legal issues, and health equity. The ability to hire retirees as field staff also was an important mechanism for filling some positions.
Many jurisdictions needed additional staff to meet the volume of response work that exceeded the capacity of existing staff in health departments. The CDC Foundation field assignees provided surge capacity in a range of public health response work including contact tracing, call centers, community outreach to at-risk populations for vaccines, work with schools, data entry and analysis, outbreak investigations, and infection control monitoring in healthcare facilities. Many jurisdictions had difficulty meeting the increased demand for administrative and operational support related to COVID-19 grants, contracts, and legal issues. Field assignees helped mitigate the administrative burden that occurred in many health departments.
The value of the positions and field assignees was highlighted by the retention of 19% of positions through alternative funding. In addition, a possible broader impact of this project on the public health workforce is that many field assignees were new to governmental public health work and expressed an interest in continuing this career path. While not a formal pipeline, bringing staff in for short-term response positions can raise awareness of governmental public health as a career.
The project also resulted in long-term improvements in health department capabilities. Examples include the establishment or improvement of data dashboards, creation of training materials and budget tools, and establishment or improvement of surveillance systems, including wastewater surveillance.
Impact of Focused Activities
The frontline field assignees in schools delivered accurate information about COVID-19 to the community, addressed vaccination hesitancy, and strengthened COVID-19 case reporting and monitoring. Some field staff helped address other important public health needs, including mental health and dental needs identified among students in the school.
Field assignees working to advance health equity enabled jurisdictions to reach out to communities at high risk for COVID-19 and develop stronger relationships that will continue beyond the response. In some jurisdictions, field assignees were the first staff hired specifically to work on health equity and the first to establish a focus for this work in the health department. Others improved processes to assure equity within the health department and strengthened ongoing work. Such community-driven outreach efforts can address cultural barriers and promote acceptance of public health interventions. In addition, existing partnerships and resources can assist with effective implementation of response activities. 10
The use of trusted messengers and strategies tailored to unique needs of communities can improve communication and address misinformation.10,11
Field assignees working with tribal entities supported the COVID-19 response to American Indians/Alaska Natives, a population that has been disproportionately impacted by COVID-19 in terms of disease incidence, 12 mortality,12,13 and life expectancy. 14 The field assignees brought much-needed expertise and skills to help address the COVID-19 response. They also brought a new or strengthened focus to public health that was missing in some tribal organizations, including the establishment of a new public health department. 15 As noted by a tribal contact, the CDC Foundation partnership provided knowledgeable staff who were needed to help the tribe survive and thrive.
Conclusion of the Project
The Workforce/Vaccine Initiative was implemented to meet jurisdictional COVID-19 response needs nationwide. Over time, certain positions were discontinued when they were no longer needed to support a jurisdiction's response efforts. A process to offboard all field assignees began in the spring of 2022. While there was no additional funding beyond the initial award, carryover funds enabled the project to continue beyond the originally planned end date of July 31, 2022. All field assignees and field assignee support through this funding stream concluded by April 15, 2023.
For jurisdictions that were interested in retaining the field assignees, the CDC Foundation provided a mechanism for field assignees to continue in their positions if the jurisdiction provided the Foundation with funding. In addition, some jurisdictions retained positions through direct hire or other mechanisms. Overall, jurisdictions retained 580 staff.
Discussion
Factors Contributing to Success
The Workforce/Vaccine Initiative resulted in hiring more than 3,000 field assignees, most of whom were onboarded in less than 6 months (August 2021 to January 2022), to support the COVID-19 public health response. The success of this project demonstrates that a third-party organization can play an important role in providing surge response staffing in state, tribal, local, and territorial health jurisdictions. In addition to rapid hiring, flexibility and agility were key aspects to ensuring project success. The CDC Foundation's ability to launch and maintain a large staffing effort was further refined throughout the project as the pandemic evolved and jurisdictional needs shifted. Processes were adjusted as needed to address the challenges and changes that arose. Throughout the hiring process and the assignment of staff, jurisdictions frequently remarked on the high caliber of the candidates, and many jurisdictions hired field assignees to be contractors or jurisdictional employees at the end of the initiative. Several jurisdictions appreciated the success in finding assignees for positions that had previously been difficult to fill because of the job location or required skill set.
One benefit of the strategy to hire primarily remote workers was the creation of a centralized talent pool, which allowed applicants to be considered for positions in jurisdictions where they did not reside. A centralized system can result in efficiencies (eg, applicants could be considered for similar positions if they did not match the one for which they initially applied). The hiring of remote workers helped fill positions in less populated areas or where specific expertise (eg, public health nursing, epidemiology, IT) were needed. The factors that likely contributed to this project's success could also be considered in hiring strategies for public health staff in nonemergency situations.
Project Challenges
In a surge staffing effort of this size, problems will arise. For instance, higher salaries offered by the CDC Foundation relative to jurisdictional salaries made some positions easier to fill, especially when combined with the ability to work remotely. However, in some jurisdictions, these higher salaries caused tensions between existing health department staff in similar job positions with lower salaries. The temporary nature of employment, which often requires higher salaries to attract short-term surge staff, helped mitigate concerns. Some jurisdictions noted that it was not feasible to offer higher salaries for full-time positions.
Recruiting highly skilled candidates in informatics and data architecture, epidemiology, public health nursing, and in particular, laboratory science, was challenging. Difficulties in filling technical positions might have resulted from a tight labor market and the short-term length of employment. The use of remote workers brought onboarding and management challenges, particularly in terms of jurisdiction-specific training and rapport building. The remote nature of their positions was new to many field assignees, coworkers, and managers. CDC Foundation managers and local jurisdictional points of contact worked together to meet field assignees' orientation and training needs. Regular contact with jurisdictions also ensured that CDC Foundation managers were aware of evolving staffing needs and potential challenges.
Not all of the requested positions were filled, primarily due to a lack of qualified candidates for positions in remote areas or positions with highly specialized qualifications (eg, laboratory science, informatics, public health nursing, medical epidemiology). The need for a larger pool of qualified candidates and pipelines to recruit technical positions in public health, which has been described elsewhere,16,17 could benefit from stronger pathways between academia and public health.7,16 The pandemic amplified this issue and plans have been proposed to address the shortfall, including reassessing public health roles, improving the recruitment process, investing in employees already working in public health and strengthening leaders, and promoting diversity, equity, and inclusion. 18
Limitations
This case study reports on the experience of a large-scale project to support jurisdictions during a public health emergency by providing additional staffing to improve surge capacity. This experience provides insights into the process of hiring a large number of public health staff to meet the wide-ranging response needs of jurisdictions across the United States and the value of these staff to the jurisdictions.
There are many unanswered questions that cannot be addressed with the project data. Because the project focused on staffing, metrics on project performance centered on data related to recruiting, hiring, and retaining field staff. The project did not integrate an assessment process into the work to allow a careful analysis of staff ability to meet jurisdictional needs, the suitability of staff for requested positions, or the work products of field staff. Short-term impacts are limited to anecdotes and reports from jurisdictions. Longer-term impacts, such as the sustainability of programs or processes established or improved by field staff, cannot be assessed. For example, the number of staff retained is likely an underestimate of the utility of this project for identifying qualified staff to continue as health department employees. The data collected were primarily related to field staff employed by the Foundation during the last several months of the project and do not include field staff who left their positions for permanent jobs at health departments during the response. Finally, it was beyond the scope of the project to assess the impact of remote workers on hiring practices of jurisdictions or the impact of higher salaries on the expectations of applicants or established health department staff.
A 2023 analysis of general workforce needs showed that state and local health departments need to hire a minimum of 80,000 full-time equivalent (FTE) employees to provide a minimal set of public health services. 16 This estimate includes 54,000 FTE employees at the local health department level and 26,000 FTE employees at the state level. However, that estimate does not include the potential need for additional staff to respond to a public health emergency. This case study suggests that a centralized staffing approach to support a public health response can provide skilled staff to affected jurisdictions quickly and on a large scale. The use of a third party is one of several mechanisms to improve surge capacity during an emergency response. Other mechanisms used by health departments to increase workforce capacity during the response included volunteers and collaborations with nongovernmental organizations. 19 In addition, the CDC deployed 208 teams in the early phase of the COVID-19 pandemic to assist state, tribal, local, and territorial health departments. 20 Other potential sources of surge staff include members of crisis response teams and medical reserve corps, and persons returning from military deployments. 6 Having third-party contracts in place before an emergency might speed the hiring of surge staff. 6 Kilmarx et al 21 noted that the removal of administrative and other barriers and strengthening of human resources capacity will be needed in order to hire an expanded workforce quickly to respond to the emergency.
Conclusion
The COVID-19 pandemic exacerbated staffing challenges that health jurisdictions have faced for years, including understaffing and inadequate expertise and infrastructure for emergency response management and vaccine equity. This case study reports on the successful role of a nongovernmental organization as a mechanism to meet immediate surge staffing needs for health jurisdictions during a nationwide public health emergency. The comprehensive and collaborative approach undertaken by the CDC Foundation brought skilled staff to jurisdictions in need and bypassed many obstacles typically encountered by these jurisdictions when hiring public health staff. Use of national recruiting strategies, remote work, and competitive salaries resulted in filling many positions that might have otherwise remained vacant. The development of data systems and reporting tools not only supported the immediate response but also strengthened existing infrastructure. In some jurisdictions, activities to address gaps in public health infrastructure (eg, strengthening community engagement and establishing or strengthening work in health equity) continued beyond the end of the project.
The centralized systematic approach described in this case study offers many advantages for a large public health response. The recruitment and hiring approach allowed the types of staff positions to change as the pandemic evolved and as jurisdictions identified specialized personnel needs. Such flexibility suggests that this approach to surge staffing could also be used for a range of public health emergencies, for which specialized staff are needed quickly and for a prolonged period of time (eg, for a chemical spill, earthquake, or hurricane).
Footnotes
Acknowledgments
Recruiting, hiring, and maintaining this public health workforce succeeded because of the work done by many staff at the CDC Foundation and partners in state, tribal, local, and territorial health jurisdictions. The authors wish to recognize the work of Robert Foley and Beth Handler, project directors; Angelina Esparza, vice president for health equity for the Workforce/Vaccine Initiative; Breannon Babbel and Kristen Rankin, associate project directors; the area and regional managers who implemented the work; and the data team who maintained the datasets. The project was supported by internal operations including Monique Patrick, chief operating officer, and the staff of the human resources, finance, communications, and IT departments at the Foundation. The authors recognize the support of Lisa Waddell, MD, medical director of the CDC Foundation at the time of the project, and Toni Perling, senior communications specialist. We also wish to thank the leadership in the health departments of the jurisdictions and the more than 800 points of contact at the state, tribal, local, and territorial health jurisdictions who made the work assignments successful. The authors recognize the hard work and dedication of more than 3,000 field assignees who supported health departments in their response to COVID-19. Finally, thanks to the team at the CDC who developed the concept of a third-party hiring effort and provided funding to support the initiative.
This project was 100% funded by the CDC and the US Department of Health and Human Services (HHS) as part of financial assistance awards of $200 million and $20 million. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, the CDC, HHS, or the US government.