
Abstract
Botulism is a rare, potentially fatal illness caused by botulinum toxins produced by Clostridium bacteria. There are no coordinated worldwide reporting mechanisms for botulism cases and therefore few reliable case frequency estimates. This study aimed to establish an international benchmark for case frequency to determine estimated global rates of underreporting of botulism cases. To this end, a comprehensive, multilingual search of major global and national databases, including gray data and government sources, was performed. Data from case series were pooled, standardized against United Nations midyear population estimates, and analyzed using Kolmogorov-Smirnov tests to identify normally distributed data series. National incidence rates of normally distributed series were compared with that of the United States, which was considered the gold standard due to its extensive data reported for 2004-2018. A total of 6,932 botulism cases from 59 nations were identified in the literature, with a global case fatality rate of 1.37%. The national mean incidence rate ranged from 0.00 to 8.04 cases per million people, with an international mean incidence rate of 0.62 cases per million people. At the continent level, incidence rates tended toward normal distributions, although few countries outside of North America and Europe exhibited normal distributions. Based on comparisons with the US standard, an estimated 88.71% of botulism cases worldwide were unreported in 2016. Better awareness of botulism among healthcare professionals, coordinated global reporting mechanisms, and research on additional contributing factors to underreporting would enable better understanding of global case frequency, thereby potentially reducing the global incidence of botulism and improving outcomes.
Introduction
Botulism is a rare illness caused by botulinum neurotoxins (BoNT) produced by gram-positive, spore-forming anaerobes of the Clostridium species, including C botulinum groups I to IV, C baratii, C butyricum, and C sporogenes. 1 With an estimated median human lethal dose of 1 ng/kg body weight, BoNT is considered one of the most poisonous known biological substances.2,3 The median human lethal dose of BoNT, the spore-forming nature of the associated bacterial species, and its accessibility through rudimentary production techniques make BoNT a potential biothreat that could be used in “lone wolf” terrorism or state-sponsored biological warfare. 4
There are 6 clinical forms of botulism including foodborne, adult intestinal toxemia, infant, wound, and inhalational. Foodborne botulism is caused by the direct ingestion of BoNT, whereas adult intestinal toxemia, infant, and wound botulism are caused by the introduction of bacterial spores that germinate in the body to produce BoNT.5,6 Inhalational botulism may be caused by weaponized, aerosolized BoNT. Regardless of the form, botulism is characterized by descending flaccid paralysis due to blockage of neurotransmitter release at neuromuscular junctions and may lead to death due to respiratory failure. 7
While human botulism mortality rates were reported to be over 60% in the 1950s, 8 improved supportive care, including respiratory support and antitoxins, decreased mortality rates to less than 5% in 2016.9,10 Nonetheless, botulism continues to present a significant burden to the healthcare system due to the duration of hospitalization, including intensive care, required for many affected patients. 11
Increased public awareness of botulism through health promotion may reduce the number of new botulism cases. For example, increased awareness among pregnant women about the potential association between honey-containing products and infant botulism has also been associated with decreased rates of infant botulism. 12
Better awareness of botulism among healthcare professionals is also paramount. Emergency responders and other providers must have sufficient knowledge to rapidly recognize and treat BoNT poisoning cases when they present at the point of care. Death from BoNT poisoning is dependent on the dose, route, and patient. Because BoNT is a synaptic inhibitor, internalization of the toxin in sufficient quantity is required to disrupt major organ functioning and cause death. In cases of foodborne ingestion, where the toxin needs to be actively transported, the incubation period is extended to between 6 hours and 10 days, depending on the toxin quantity, with a mean clinical presentation at 18 hours. 13 This provides a clinical window of opportunity to apply antitoxin, given that the first 48 hours after ingestion or contamination are deemed critical to survival.10,14 Thus, rapid identification and early diagnosis of botulism at the first point of clinical contact are of critical importance.
Despite BoNT's inherent risks to life and its potential use in bioterrorism and warfare, there is no coordinated reporting mechanism for BoNT poisoning worldwide, and therefore few reliable case frequency estimates. This study aimed to establish an international benchmark for case frequency to determine estimated global rates of underreporting of botulism cases. The study also aimed to statistically analyze the case frequencies of botulism to extrapolate an estimated volume of global underreporting or misdiagnosis.
Methods
A comprehensive, international, multilingual literature search of MEDLINE, PubMed, Scopus, and Google Scholar databases was performed following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) principles. The aim was to identify historical botulism epidemiology data estimates, case series, and case reports using 10 associated composite search terms: botulism, botulism case study, botulism epidemiology, botulism outbreaks, botulism surveillance, botulism treatment, botulism toxin, foodborne botulism, infant botulism, wound botulism. All epidemiological databases containing botulism data in the languages of the search were also included. These included the databases of the European Centre for Disease Prevention and Control (ECDC); US Centers for Disease Control and Prevention (CDC); the Global Health Observatory; Australian Government Department of Health and Aged Care; UK Health Security Agency; Health Canada; the Centers for Disease Control in Argentina, Brazil, Chile, Colombia, Mexico, Peru, South Africa, and Africa; ProMED-mail; and Global Infectious Diseases and Epidemiology Network (GIDEON).
Additional searches of gray literature, including government sources, were conducted in 10 major languages (Cantonese, Dutch, English, French, German, Italian, Mandarin, Portuguese, Russian, and Spanish).
All searches were performed to identify literature published between January 2020 and January 19, 2023. ECDC nonreported years for each nation were assumed to have zero cases. For the purposes of the search, a case was defined as laboratory-confirmed human botulism with detection of C botulinum or its BoNT from clinical samples, or a positive BoNT serum test, or a case epidemiologically related to a laboratory-confirmed case. 1
A total of 2,230 articles were initially identified in the literature search. Article titles and abstracts were then evaluated to determine whether the content was relevant. Full-text articles considered to be potentially relevant were reviewed to collect available data regarding case fatality rates (CFRs) and clinical forms of botulism cases from case series and case reports. Articles that reported no cases were eliminated, as well as articles reporting duplicate case information and articles from before the year 2000. After screening for eligibility, 173 articles were included in this analysis (Figure 1).
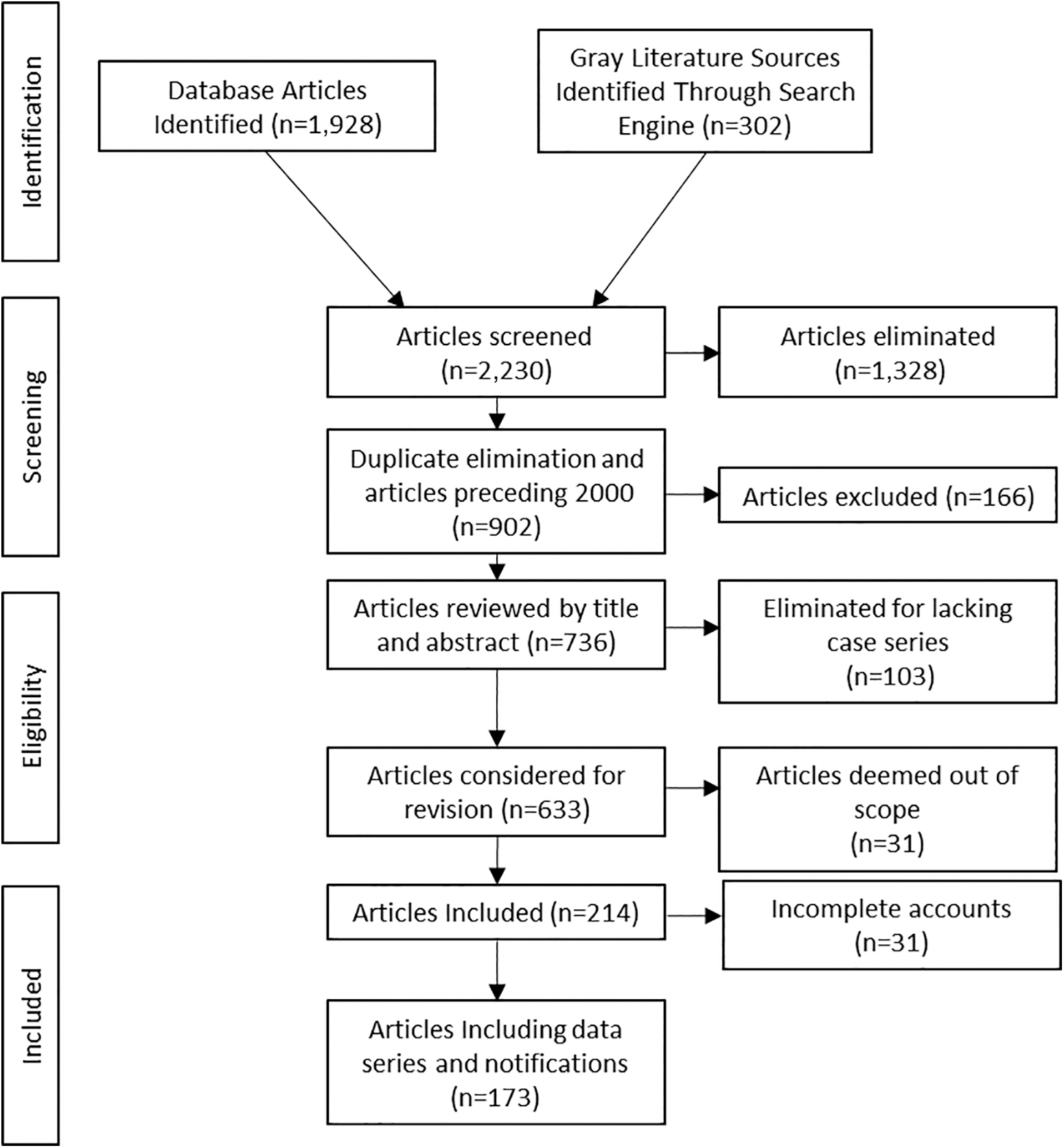
PRISMA flow diagram of literature search and data mining.
Data from case series were pooled to determine the estimated national incidence rate per million people and were then compared with respective United Nations midyear population estimates. The national annual mean cases per million people (casesM−1) and data series standard deviations (SDs) were calculated from the means. Where possible, hospitalization as a percentage of cases was calculated, as was the CFR. For cases that were reported as not requiring hospitalization, the percentage of cases resolved in primary care was determined.
Deviations from UN estimates in national annual reporting were calculated using national sample medians, as well as 25th and 75th percentiles. To assess whether the sample means were derived from normal distributions or whether major outbreaks had skewed the low probability event data series, data series with no 25th percentiles and with a value of zero were rejected. The Kolmogorov-Smirnov test was applied to all remaining data series to confirm the presence of normal distribution (P>.05).
Normally distributed national series were compared with the mean derived from US CDC data, 15 which was considered the global gold standard, using an analysis of variance (ANOVA) with a post hoc Tukey-Kramer test.
The national series mean values for botulism incidence were compared with United Nations International Food Safety Authorities Network (INFOSAN) national food availability and utilization scores to determine whether botulism cases had a shared national tendency with food insecurity. As the INFOSAN food availability and utilization scores were heavily skewed toward zero, a Wilcoxon signed ranked test was used to compare the variables. Given that the mean national botulism values were also skewed toward zero but of larger composite sample size (n=59), correlation with the normally distributed World Bank national physician density (value per 10,000) data 16 was assessed using parametric and nonparametric means by Pearson and Spearman rank correlation coefficients.
The data series were then grouped by continent to determine mean values and differences between continents. The 6 continental groups were reduced to include only the period 2013-2018 in order to exclude African continental zero values. The data were then assessed for normality using the Kolmogorov-Smirnov test (P>.05) and eligible data were subject to ANOVA Tukey-Kramer post hoc analysis (P<.05).
A global estimate of underreporting was produced from the global series mean value for 2016, the most complete reporting year.
As data series did not always include sources of botulism, the US CDC series was used to determine likely incidence rates for foodborne, wound, and infant botulism.
Results
A total of 6,932 cases of botulism were identified in the literature between January 2000 and January 2023 from 59 nations, with Hong Kong included in the China count (Figure 2). The largest proportion of reported cases was from the United States (41%; Figure 3). A total of 95 deaths were reported, for a global CFR of 1.37%. A total of 3,776 cases (54.47%) were reported as requiring hospitalization, and 685 cases (9.88%) were reported as not requiring hospitalization; the location of treatment was not reported for the remaining 2,471 cases (35.65%).


Number of reported botulism cases by country, 2000-2022.
More than 1 annual botulism report was available for 51 nations. The United States had the most comprehensive data series consisting of 18 years of data. Mean annual incidence rates ranged from 0.00 casesM−1 in South Korea to 8.04 casesM−1 in Montenegro. The international mean (SD) was 0.59 (± 0.1%) casesM−1 (Supplemental Figure S1; supplemental figures available at www.liebertpub.com/doi/suppl/10.1089/hs.2023.0081).
The 25th percentiles of 37 nations were recorded as 0.00, exhibiting a skewed distribution toward zero, while 21 nations demonstrated normal distributions (P>.05). The United States and the European Union (including the United Kingdom, which was included in the EU data before 2022) showed narrower ranges.
A 95% CI plot using the 0.51 casesM−1 US mean as a standard highlighted the large spread in non-EU and US data series (Supplemental Figure S2). Only 7 non-EU nations intercepted the US mean.
Continental data series showed normal distributions, with the exception of Australasia, for the period 2013-2018 (P<.05; Figure 4). ANOVA Tukey-Kramer post hoc testing revealed that only European and North American populations were not statistically different (P<.05).

Using an approximate world population of 7.6 billion, the global underreporting of botulism cases for 2016 was estimated to be 4,092 cases or 88.71% using the mean national value prevalence per world population.
The US CDC series (2006-2018) 15 reported most (72.98%) cases as infant botulism, followed by 13.79% of cases as wound botulism and 11.56% as foodborne botulism.
Analysis of INFOSAN values revealed higher annual incidence rates per million people between the INFOSAN food availability and utilization index and standardized national botulism incidence rates (P<.001). The INFOSAN index is an indicator of food safety and security, which is primarily used in non-EU nations, and was developed by the World Health Organization in partnership with the Food and Agriculture Organization of the United Nations. Higher cases per million were associated with a higher INFOSAN value. This would be expected as higher food safety standards should lead to a lower frequency of food poisoning. World Bank data 16 on national physician density showed no correlation with standardized national botulism incidence rates (r=-0.019; Spearman correlation=0.05).
Discussion
Data on botulism cases were unavailable for most countries globally, with only 59 countries having any case numbers available. Some countries, such as Russia, reported government estimates on caseloads but no raw data. 19 Additionally, many datasets remained incomplete as to the cause of disease, patient outcomes, and hospitalized case numbers. Only the US reports contained details on the cause, with a combined 250 food-related cases, 300 wound botulism cases, and 1,558 infant cases during the reporting period. 15 While infant botulism made up the largest proportion of reported cases to the US CDC, data on botulism types were lacking from all other case series. The lack of information relating to infant botulism may indicate that a significant proportion of mild case infantile botulism goes unreported in areas where botulism occurrences are not notified to authorities or published. Additionally, the calculated global CFR of 1.37% is extremely low considering the limited availability of botulism antitoxin globally and compared with the reported CFR of 1.37% in the United States, which is among the most prepared nations in terms of antitoxin stockpiles. The low CFR could indicate that cases were reported only in countries where healthcare professionals were aware of the signs and symptoms of botulism, such as descending paralysis, and announced such cases to their respective authorities, who in turn had antitoxin stockpiles available for rapid access. Similarly, the low hospitalization rate of 54.7% is likely the result of data underreporting given that the US CDC data series included only secondary care cases, despite that all suspected cases were admitted.
The available data suggest that the majority of global botulism cases are not reported, with an estimated 88.71% of cases unreported in 2016 based on comparisons with US CDC data. Such underreporting could be due to lack of awareness among healthcare professionals about botulism as a rare disease. 20 Underreporting in nations outside of North America and Europe may also result from a lack of coordinated notification and reporting mechanisms, particularly as the PubMed, ProMED, and GIDEON databases rely on reporting at an international level or media reports to capture case information. Other potential factors contributing to sporadic reporting and lack of data on the number of unreported cases include the following: (1) Clostridium spp. spores have been found to be ubiquitous in soil and agricultural products but are not evenly spread in soil around the globe, (2) food preservation practices and standards differ between nations, and (3) dietary habits and cooking practices differ based on cultural, economic, environmental, and religious circumstances. 1 Such differences may account for national reporting deviations from the US gold standard.
An additional factor that may contribute to underreporting is the effect of case volumes on reporting resources. This study found that only countries or supranational regions with with larger populations and well-coordinated centers for disease control, such as the US CDC and the ECDC, were able to present case frequencies greater than 50, enabling better approximation to normal distributions. While all continents, except the sparsely populated Australasia, followed a normal distribution for 2013-2016, 17 of the 21 nations that demonstrated normal distributions were European. Botulism is a notifiable disease in Europe with epidemiology reported to the ECDC. The influence of the supranational ECDC was evident in the reporting of the United Kingdom, which failed to report any botulism cases after exiting the European Union on January 31, 2021.
Outside of the European Union, large variations were seen in reporting, with a wide range of national mean annual case incidence and only 7 non-EU nations overlapping US mean case incidence reporting. Variations may be due in part to food availability as the INFOSAN food availability and utilization index was highly correlated with botulism case frequency. However, physician density is unlikely to play a role because World Bank physician density data were not considered a contributory factor in botulism case frequency. Additionally, the fact that the international mean of 0.59 (± 0.1%) casesM−1 was higher than mean botulism case incidence of 0.51 casesM−1 in the United States suggests that, on a global level, large outbreaks are more likely to be reported than individual cases and indicates a lack of consistent case-by-case reporting.
As botulism cases include both outbreak-associated cases linked by chains of causation and individual low-frequency events, prediction is difficult in low volumes. The collection of data from larger populations with annual botulism frequencies over 50 dilutes extreme annual events or outbreaks, creating greater accountability for surveillance systems and better predictability for preparedness. Findings from this research indicate that for botulism prediction to improve, surveillance of botulism cases should ideally occur in populations exceeding 100 million. A policy advancement, in terms of reporting sensitivity and appropriate planning for the provision of medical countermeasures, could consider supranational reporting and surveillance with procurement and geographically dispersed stockpiles.
There are some limitations to this study. It covered only publicly reported cases and those appearing in official databases, on official government websites, or that were picked up by international search engines appraising gray literature. There was also a restriction of the languages used to search for botulism terms and the willingness of governments to share information relating to botulism case prevalence, potentially due to security sensitivities related to disclosing national provisions of the BoNT antitoxin as a medical countermeasure for deliberate BoNT poisoning. Future research on surveillance of BoNT should consider other contributing factors to underreporting, including that although Clostridium spp. spores are not evenly spread in soil around the globe despite being shown to be ubiquitous in soil and agricultural products. In addition, food preservation practices and standards differ between nations, as well as dietary habits and cooking practices based on cultural, economic, environmental, and religious circumstances. 1 Such differences may account for national reporting deviations from the US gold standard.
Conclusion
Reporting of botulism cases was sparse outside of the European Union and North America. Epidemiological consistency in reporting would enable more in-depth statistical analysis and reduce the impact of large outbreaks on case volume anticipation. Thus, better surveillance of botulism cases is needed outside of the European Union and North America if global case frequency and mortality are to be fully understood and potentially reduced. A policy consideration could be to collect data at a suprainternational level to aid consistent reporting.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.