
Abstract
Similar to the early phases of the COVID-19 pandemic, New York City was the national epicenter of the ongoing 2022 mpox (formerly monkeypox) outbreak. Cases quickly began to rise in July 2022, primarily in gay, bisexual, or other men who have sex with men. Tools in the form of a reliable diagnostic test, an effective vaccine, and a viable treatment option have been available from the onset, although logistically complex to roll out. The special pathogens program at NYC Health + Hospitals/Bellevue, the flagship facility for the largest public hospital system in the United States, collaborated with multiple departments within Bellevue, the hospital system, and the NYC Department of Health and Mental Hygiene, to swiftly establish ambulatory testing, immunizations, patient-centered inpatient care, and outpatient therapeutics. With the ongoing mpox outbreak, hospitals and local health departments must prepare a systemwide response to identify and isolate patients and provide high-quality care. Findings from our experience can help guide institutions in developing a multipronged, comprehensive response to the ongoing mpox outbreak.
Background
First reported in humans in the 1970s, 1 mpox (formerly monkeypox) is characterized by skin lesions, acute tonsillitis, coughing, and lymphadenopathy, and can lead to long-term complications including vision damage and scarring. 2 Endemic to Central and West Africa, 3 the first confirmed case of the 2022 mpox outbreak outside of Africa was reported in the United Kingdom on May 6, 2022. 4 The virus quickly began spreading in Europe and other non-endemic countries,5,6 including the United States, when a patient who traveled to Canada was admitted to Massachusetts General Hospital in Boston and later tested positive for mpox. 7 Primarily circulating in men who have sex with men (MSM) social networks, the virus has been identified in every US state. 8
Projections of mpox cases have been scarce. One study simulating a population of 50 million people with socioeconomic and demographic characteristics of a high-income European country suggested an introduction of 300 cases without public health interventions could cause 402 secondary cases and lead to a 37-week-long outbreak. 9 The model predicted that isolation of primary cases, contact tracing, and postexposure prophylaxis (PEP) in the form of ring vaccinations would reduce secondary cases by 86.1% and the duration of the outbreak by 75.7%. A 2022 modeling study demonstrated similar findings. 10 These examples highlight the importance of a robust public health response through reliable, accessible testing and PEP.
New York City is the national epicenter of the 2022 mpox outbreak. 11 Cases quickly began to rise in July 2022, primarily in gay, bisexual, or other MSM.11,12 With 3,821 patients diagnosed as of December 31, 2022, the city needed healthcare institutions to partner with its public health authority to control the outbreak. 11 As the US Department of Health and Human Services Region 2's Regional Emerging Special Pathogen Treatment Center (RESPTC), New York City Health + Hospitals (NYC H+H)/Bellevue has served as the backbone of the city's response. Due to an atypical clinical presentation and an unusual pattern and speed of transmission, mpox was initially treated as a high-consequence infectious disease. 13 Bellevue rapidly amplified its role as the RESPTC to provide inpatient biocontainment unit care, outpatient therapeutics, postexposure vaccinations, diagnostic testing, and mental health support to those primarily affected by the virus. Managing this dynamic and fast-moving outbreak was complex and required intense collaboration. Bellevue leveraged many partnerships developed in response to the COVID-19 pandemic with the NYC Department of Health and Mental Hygiene (DOHMH), NYC H + H leadership, and the NYC Public Health Laboratory (PHL). DOHMH provided leadership and support across NYC health systems, including NYC H+H/Bellevue, to implement treatment programs, facilitate vaccine distribution and administration, and access testing through NYC PHL. The systems and procedures developed at Bellevue in response to the mpox outbreak can provide a blueprint for other institutions and hospitals navigating this public health emergency and future outbreaks.
Infection Control Strategies
From an infection control perspective, it is imperative to educate the public that although the virus is disproportionately circulating through social networks of MSM through close skin-to-skin contact,5,11,14,15 anyone in close contact with an infected individual's infectious skin lesions or contaminated material can contract the virus.3,15,16 Hand hygiene with alcohol hand sanitizer, or soap and water, should be performed after touching potentially contaminated material. For those sharing spaces or providing care to a patient with mpox infection, US Environmental Protection Agency-approved disinfectant wipes are recommended to disinfect shared surfaces. Patients who must leave their isolation space should always wear a mask and cover all lesions with clothing or bandages.
Community transmission depends on the effectiveness of several public health measures: testing capacity, public education, treatment availability, and vaccine distribution. A small number of women and children have already contracted the virus, and it could continue to spread to other groups or social networks unless testing, vaccine access, and contact tracing tools are implemented. 11 Tracking testing trends, such as the number of tests performed and the testing positivity rate, are key data tools that the hospital's infection control department uses to monitor the extent of transmission and adequacy of testing capacity. The tools are at our disposal to contain this outbreak, and the national epidemic curve has fallen significantly since the 2022 summer peak. However, without ongoing surveillance and implementation of these effective public health measures, mpox could continue to spread or become resurgent in the United States. 17
Therapeutics
On June 19, 2022, Bellevue became the second institution in the city to prescribe tecovirimat and the first for an ambulatory patient. Tecovirimat was available under an expanded access investigational new drug (EA-IND) protocol held by the US Centers for Disease Control and Prevention (CDC; Institutional Review Board [IRB] approval #6402), which was the basis of the NY Langone Health IRB (#i22-00812), approving an expanded access program protocol. Prescribing under this program required a large quantity of paperwork to stay in compliance, including the submission of patient informed consent forms and case report forms to the CDC, 18 and reporting all prescriptions to our local health department and IRB. Exacerbated by increased demand for treatment in July 2022, the workload became comparable to a clinical trial but providers lacked the support staff usually associated with research. This made prescribing tecovirimat at scale difficult for providers who also manage existing clinical responsibilities. To expand Bellevue's outpatient treatment capacity, additional infectious disease specialists and general internists were added to the expanded access program IRB protocol. An mpox treatment decision workflow (Figure 1) determined the best course of action for each patient depending on severity and risk factors. The treatment workflow emphasized the importance of supportive care, including pain control, anti-itch creams, wound care, and antibiotics for superinfection of skin lesions.
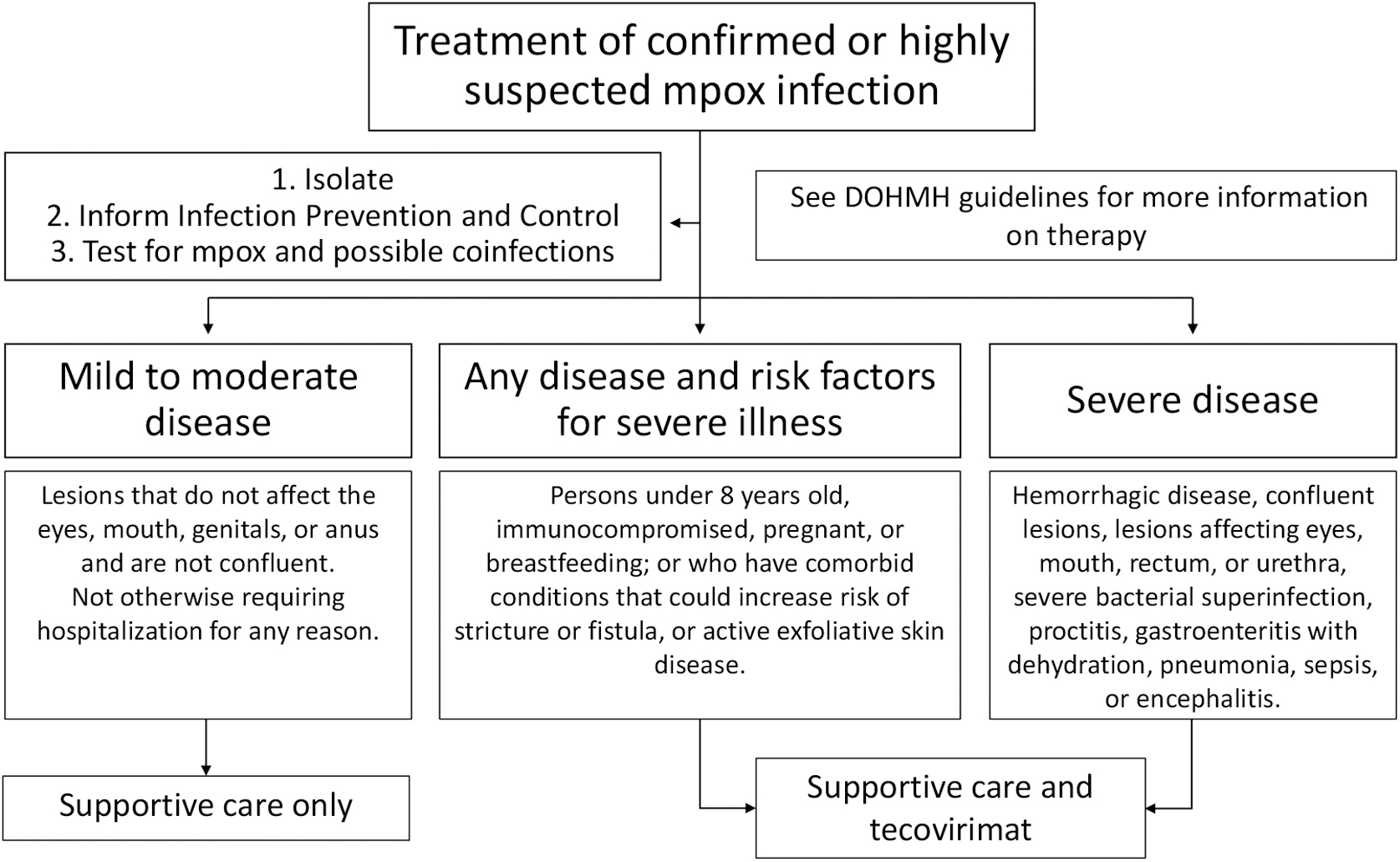
Mpox decision workflow to determine treatment options based on severity and risk.
Given the limited number of available treatment appointments, we built a system of triaging patients who needed antiviral treatment. A team reviewed a daily mpox testing report, called patients to communicate results, and conducted a brief phone interview assessing whether they may be antiviral treatment candidates based on current treatment guidelines published by our local health department. Potential treatment candidates were added to a list of patients and discussed every morning by a treatment triage team consisting of infectious disease specialists. This team assessed the clinical urgency of each case and scheduled patients into available appointments for the week. We maintained close communication with our local health department as they would refer additional treatment candidates from throughout the city to Bellevue based on our weekly treatment capacity.
The initial model of prescribing tecovirimat was through video telehealth visits. For patients able to navigate telehealth visits, this approach made scheduling more flexible and made it easier to adhere to infection control precautions. To comply with the expanded access program requirements for telehealth visits, patients signed a PDF version of the informed consent form, took photos of their skin lesions, and submitted all files to the prescriber via the electronic medical record (EMR) patient portal. If a patient was unable to do so, or also required sexually transmitted infection testing, we accommodated in-person clinic visits in the ambulatory clinic staffed with nurse practitioners and physicians.
DOHMH Collaboration to Expand Treatment Access
Many providers across the city, including those with investigational new drug experience, have had difficulty navigating the EA-IND protocol for tecovirimat. DOHMH supports clinical providers by offering technical assistance to implement the EA-IND protocol and finding ways to efficiently implement the protocol. DOHMH's goal has been to facilitate treatment access for any patient who would benefit, and to act as a liaison between providers and the CDC.
Another DOHMH role has been connecting patients to providers who can prescribe tecovirimat. The DOHMH tecovirimat navigation team received emails from outside providers looking to refer their patients for treatment and developed an intake form for referred patients. Intake forms were triaged and connected to external providers able to take external referrals with limited capacity. In mid-July 2022, the team received 5 to 15 intake forms a day. The tecovirimat navigation team has been an essential bridge for many New Yorkers looking for treatment options. However, as NYC providers able to accept referrals from outside their health systems became inundated with their own patients, the DOHMH focused on supporting providers with implementing tecovirimat protocols in their own practices.
DOHMH has also facilitated the distribution of tecovirimat. Providers with an onsite pharmacy have been stocked, so patients seen for in-person visits can leave with their prescriptions in hand. In addition, DOHMH has partnered with a central pharmacy to deliver the medication from a citywide cache directly to patients' homes. This complements community-based and telemedicine services with a patient-centered approach to tecovirimat distribution.
Unfortunately, gaps left by the federal government have meant that local health departments must continue to meet this need. The protocol and much of the logistical information were not readily accessible on the CDC website but were shared through email and phone communications only. Information was clarified with an updated protocol approved by the CDC on July 22, 2022, which streamlined the EA-IND process by making the reporting of laboratory tests and photos of lesions optional, allowing telemedicine visits, and removing some follow-up visits as requirements. 18
Hospital Leadership
Hospital leadership played an important role in coordinating and facilitating communication across departments. Bellevue hospital leadership organized the response into 5 domains: emergency department testing, ambulatory care testing, inpatient care, outpatient care, and immunizations. In each domain, NYC H+H/Bellevue's special pathogens program (SPP) led the way by developing the early protocols. However, as case counts grew in New York City, the SPP required assistance from the general hospital to manage the influx of patients coming for testing and the expected rise in inpatient and outpatient care.
The SPP, in close collaboration with departments across the hospital, set up the ambulatory testing center; trained more hospitalists, physician assistants, and nurse practitioners to administer tests to emergency department walk-ins; developed surge plans; increased capacity for outpatient care; and coordinated vaccinations. The transition to a hospital-wide approach would not have been possible without the help of hospital leadership bridging departments together.
Hospital leadership has also supported the staff by allowing overtime pay (also known as “moonlighting”) for doctors performing testing, conducting video visits, or providing care outside their routine clinic sessions. Nurses were redistributed to staff the ambulatory testing center and given overtime pay for any additional hours. Additionally, NYC H+H/Bellevue used agency staffing to ensure the hospital remained fully staffed. The hospital has established a culture of going above and beyond to achieve its mission, with many staff volunteering to help however they can. Nonetheless, moonlighting was established for providers to help combat burnout, which was already at a high level due to the COVID-19 pandemic.
Vaccine Distribution
NYC H+H/Bellevue was one of the first hospitals in New York City to administer the JYNNEOS mpox vaccine, prioritizing high-risk contacts of known cases to receive PEP, in collaboration with the DOHMH. Initially, Bellevue received 200 doses from the Strategic National Stockpile, enough for 100 PEP vaccine series. The ambulatory care team repurposed 2 stations in our COVID-19 vaccine hub and dedicated them to mpox vaccinations. As a precautionary measure, they were strategically located adjacent to an exterior doorway and physically distant from our COVID-19 vaccinations. All PEP patients were called the day prior and the day of their vaccine appointments to ensure new lesions or other symptoms had not developed since scheduling their vaccine appointment. To further minimize potential exposures, as several patients presented with active lesions despite the screening calls, a patient navigator was stationed at the door to direct those with scheduled mpox vaccine appointments. This obviated vaccine recipients from using the main facility entrance to navigate to the vaccine area.
New York City's goal has been to make the vaccine widely available to those groups most affected by the current outbreak—social networks of gay, bisexual, or other MSM, and/or transgender, gender-nonconforming, or gender-nonbinary individuals aged 18 years or older who have had multiple or anonymous sex partners in the last 14 days. In addition to PEP, the DOHMH began offering PEP++ (eg, expanded PEP) for MSM and/or transgender, gender-nonconforming, or gender-nonbinary individuals who had multiple or anonymous sex partners but no identified exposure to a known case at their sexual health clinics as vaccine supply increased in June 2022. Healthcare workers and laboratorians are offered preexposure prophylaxis in the event of a breach in personal protective equipment (PPE) or exposure. By late July, the United States received an influx of 300,000 doses of the mpox vaccine with an additional 800,000 doses arriving in early August. 17 Vaccines should be accessible to all who are eligible. To maintain health equity, modalities other than online scheduling (eg, telephone hotlines) are necessary, and translating information into languages other than English must be done. To this end, DOHMH is awarding US$5 million to community-based organizations who will promote vaccination, with a focus on New Yorkers who are lesbian, gay, bisexual, transgender, queer, intersex, and asexual (LGBTQ+) Black, Indigenous, or people of color. 19
EMR and Epic Integration
The first phase of the mpox response was similar to the early COVID-19 outbreak response. All diagnostic tests were sent to the NYC PHL and the CDC. The government laboratory systems could not directly integrate into Bellevue's EMR, Epic, requiring hospital laboratory staff to enter test results manually. Moreover, in May 2022, mpox visit types were not available in Epic. Providers ordered mpox laboratory tests categorized as “miscellaneous” and in the free text area specified, “R/O Monkeypox, please send this to PHL.” This temporary workaround allowed operations to continue but inhibited our ability to track the volume and results of the tests. We rapidly built out a new infection status category to capture mpox tests and visits, which permitted us to leverage automation and create an mpox dashboard. The dashboard monitors the hospital system's daily case counts, test turnaround times, and positivity rates, which can be filtered by age, race, ethnicity, and gender.
Due to the overwhelming number of tests being done in New York City at the beginning of the mpox outbreak, Bellevue patients began experiencing longer turnaround times for their test results. On July 14, 2022, the first commercial testing laboratory received approval to process mpox diagnostic tests, with 4 additional laboratories approved in the following week. 20 The ability to use commercial testing laboratories increased national testing capacity 13-fold, 21 and reduced NYC H + H testing turnaround times. Commercial laboratories could also integrate with the patient's EMR so that results automatically appeared after being reported. Integration with commercial laboratories has provided the aptitude to create a much quicker and more reliable testing system.
Outpatient Testing
In early June 2022, demand for mpox testing began to increase in New York City; however, availability remained limited as all testing was done through NYC PHL. 22 One month later, as mpox testing became available through commercial reference laboratories, staffing, testing supplies, and hospital spaces were organized to establish an ambulatory mpox testing center on July 14, 2022.
Figure 2 presents an overview of the steps involved in testing for mpox in an ambulatory setting. The process begins when patients schedule their mpox testing appointments. Prior to their arrival, they receive instruction to wait by the orange square posted outside the hospital at the designated time until a navigator arrives to escort them to the testing center. The navigator is always masked and gloved while escorting patients. A specific elevator is reserved to minimize contact with other patients and hospital staff. Once patients are assigned to a room, an assessment is done over the phone to gather information about symptoms, lesion sites, and their ability to isolate. This allows providers to order tests, print labels, and prepare the collection kit before entering the room. Providers also assess for treatment eligibility. If deemed eligible, they are notified and linked to our infectious disease colleagues for treatment. After swabbing is complete, patients are sent electronic discharge instructions via MyChart, which includes instructions on isolation, the turnaround time of results for mpox testing, and concerning signs or symptoms to monitor. Patients are encouraged to reach out via MyChart with questions and concerns post-visit if needed. The whole process takes approximately 20 minutes. After patients are escorted out of the building by the navigator, environmental services is notified for terminal cleaning. Clinical rooms cannot be used for approximately 30 minutes after terminal cleaning. With 3 dedicated rooms for mpox testing, visits are scheduled in 30-minute slots to ensure 1 room is always available for testing and to minimize patient care delays.
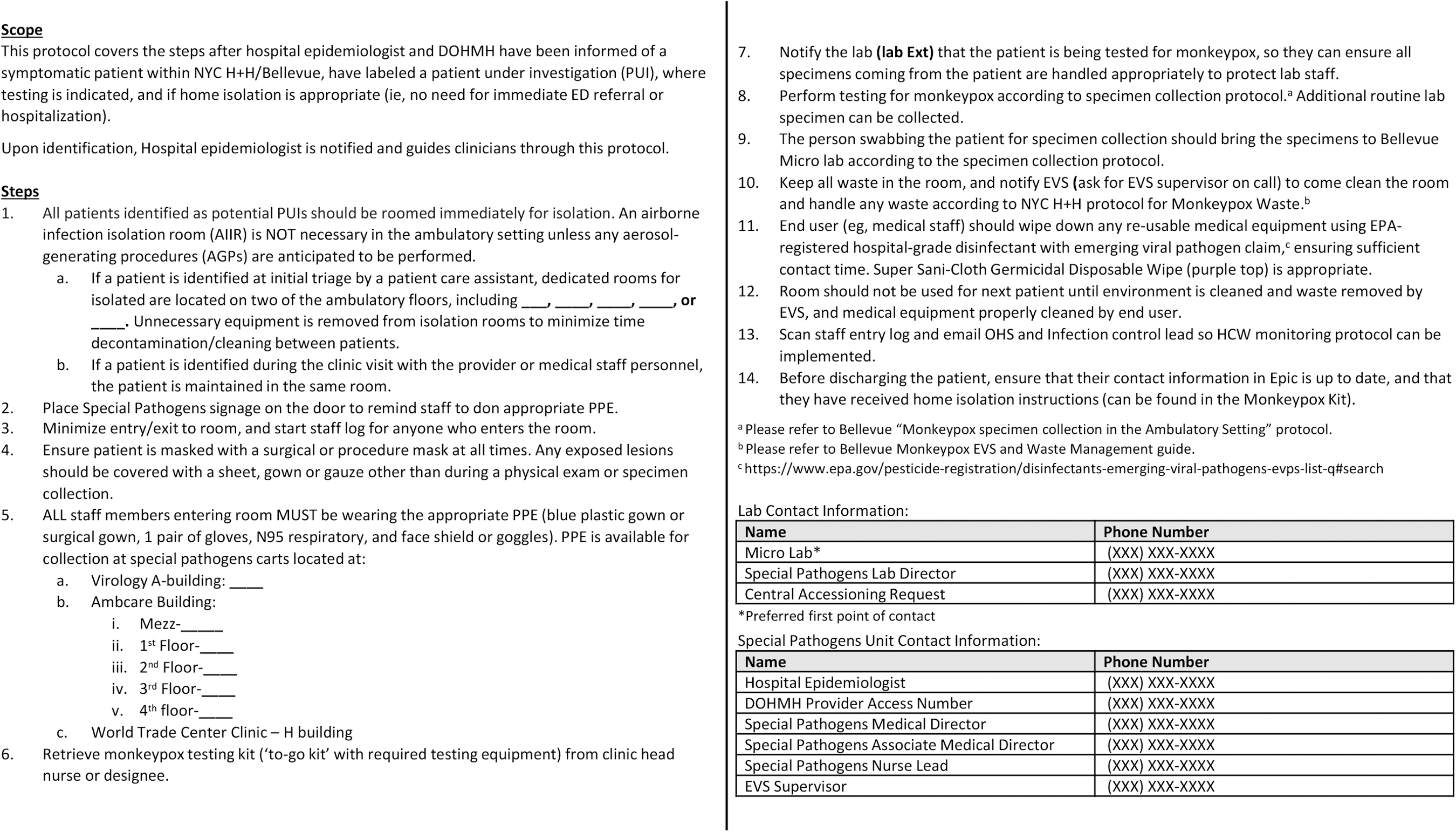
Mpox testing ambulatory setting protocol. Abbreviations: DOHMH, New York City Department of Health and Mental Hygiene; ED, emergency department; EPA, Environmental Protection Agency; EVS, environmental services; HCW, healthcare workers; NYC H+H, New York City Health + Hospitals; PPE, personal protective equipment.
Adapting our current COVID-19 monoclonal antibody treatment center's model, 3 rooms in the adult primary care clinic were repurposed for mpox testing by appointment only. Appointments were scheduled via an electronic referral in Epic, either from a patient's primary care provider or the NYC H + H virtual ExpressCare team. Community providers could also refer patients using our Epic CareLink online portal. The center was initially able to test up to 20 patients each day, 4 days a week.
Isolation sign (for patient door)
Stop sign (for patient door)
Specimen bag with 4 Dacron swabs and 4 specimen vials
3 specimen bags
Informational packet
Cheat sheet
Log sheet (for patient door)
Personal protective equipment checklist for N95
Personal protective equipment checklist for controlled air-purifying respirator
Home isolation instructions
Existing staff were assigned to operate the testing center, including 2 adult primary care nurse practitioners who performed mpox testing and contacted patients with their results, 2 patient navigators who escorted patients from outside the hospital's main entrance to the testing rooms, and a general medicine physician who oversaw all elements of the testing. Establishing the testing center was vital to expanding our diagnostic capacity.
Testing “go bags,” detailed in the Box, were created in the event that an outpatient who arrived for a routine clinic visit—not in the emergency department or the designated mpox ambulatory testing center—was suspected of mpox infection. In those circumstances, the patient would be isolated in the room where their suspected infection was first identified. Transferring the patient to the testing center or emergency department would only increase the risk for transmission and require environmental services to decontaminate 2 rooms for 1 patient. The go bag contains instructions and essential reference materials for mpox testing. Bags were supplied to each clinic and managed by the head nurse. This approach enabled the patient to receive testing without transferring rooms and possibly infecting others.
Inpatient Care
Frequent drills, including mystery patients presenting with mpox-like symptoms, and education on clade-specific presentation, increased the capacity of Bellevue's emergency department to rapidly triage, identify, and isolate potential mpox patients. Triaged patients were isolated in designated negative pressure rooms within the emergency department. Just-in-time guidebooks, signage, and donning and doffing checklists were developed by the SPP for staff to standardize care. To account for the large influx of patients presenting to the emergency department with suspicion of mpox infection, additional physicians and nurses were trained to swab, and moonlighting provided a further incentive.
Bellevue hospital has had multiple patients suspected or confirmed with mpox admitted to the inpatient service. The decision to admit a suspected or confirmed mpox patient depended on 2 factors: their ability to successfully isolate at home and their clinical status. Patients who live in congregate settings such as shelters, those in homes with shared spaces, and those under the City of New York Police Department or NYC Department of Correction custody have been unable to isolate themselves. As New York City's safety net tertiary care center, Bellevue provides care to these patients regardless of their insurance status. Patients were also admitted to manage comorbidities and/or pain. The clinical presentation of mpox can resemble other infectious diseases, and coinfections are possible. 14 Some patients needed treatment for HIV/AIDS, syphilis, gonorrhea, chlamydia, chickenpox, rickettsialpox, or other common bacterial infections while admitted or awaiting test results. Although most patients in our experience have been clinically stable and discharged to home isolation, some reasons for admission have included vomiting, rectal bleeding due to proctitis, and the inability to tolerate oral intake due to painful oral lesions. Patients who did not require hospital admission were sent home with a locally developed instruction sheet (Supplemental Material, www.liebertpub.com/doi/suppl/10.1089/hs.2022.0120) providing guidance on isolation and whom to contact with questions.
Once modes of transmission and virulence were better understood, the special pathogens program developed an mpox-specific activation plan without sacrificing quality of care (Table). Deviating from the staffing models used for special pathogens like Ebola, we decreased nurses from 4 to 2, and decreased physicians and unit lead to intermittent coverage while the nurse lead, site manager, and command center maintained 24-hours-a-day/7-days-a-week coverage. Laboratory technicians reported to the unit's biocontainment laboratory daily to perform all testing, if needed. Environmental services reported to the unit as needed once waste was downregulated from category A to category B. PPE also changed from enhanced contact to transmission-based. As cases continued to rise, and after mpox waste was further downregulated to regulated medical waste, we transitioned to routine care. Lifting the burden on the special pathogens unit, mpox patients could be treated on medical floors and in the intensive care unit. The SPP provided just-in-time training to critical care and medicine floor nurses for PPE and mpox patient care; main hospital laboratory staff for PPE and processing test specimens; and environmental services for mpox-specific waste handling. Nursing leadership educated their staff on the potential of an mpox admission into their unit. The established hospital-wide PPE delivery system was adapted to increase the availability of mpox PPE, such as face shields. To streamline clinical care processes and just-in-time training, patients were colocated as much as possible.
Table. Evolution of NYC H+H/Bellevue's Mpox Activation
Abbreviations: EVS, environmental services; PAPR, powered air-purifying respirator, PPE, personal protective equipment.
Patient-Centered Care
This outbreak is currently affecting MSM disproportionately.7,11,13 There are fears that the stigma associated with the early days of the HIV/AIDS outbreak in the 1980s is reemerging with mpox. This can be triggering and mentally and emotionally scarring for individuals in the LGBTQ+ community. Many patients infected with mpox feel scared, anxious, and worried about how their illness may progress. Being transparent, responsive to questions and concerns, and shortening the time spent in the emergency department or clinic are ways to ease patients' anxiety. In collaboration with partners of our National Emerging Special Pathogens Training and Education Center (NETEC), a clinician guide to discussing mpox in destigmatizing ways is in development.
In addition, we have developed trauma-informed care workflows to proactively address fears and anxieties that patients might experience while admitted. All patients admitted to the special pathogens unit are contacted by and given the phone number for the hospital's patient relations service (sometimes referred to as patient advocacy). They advocate for the patient by acting as a liaison between them and the care team. They also can connect patients to trained mental health counselors. The goal is to provide compassionate and trauma-informed care. Another way inpatient care has been improved is by increasing avenues of communication between the patient and the doctors and nurses. Two iPads were obtained for rooms in the special pathogens unit that patients can use to send messages to the clinical team and access test results via MyChart. This is especially important for patients who do not own a smartphone.
Community Outreach
After some challenges with mpox testing and vaccination in New York City, efforts to improve communication were made by both NYC H + H and DOHMH, including targeted outreach to at-risk patient populations through partnerships with community-based organizations, the creation of a public-facing mpox web page, 23 and use of our existing NYC H + H contact center with the ability to provide “warm” handoffs to our virtual ExpressCare providers. The NYC H + H mpox web page includes updates on NYC case counts, mpox educational materials, vaccine eligibility, and vaccine scheduling. 23 Calling the city's general information hotline, 311, or texting “MONKEYPOX” to 692-692 provides city mpox updates and vaccination appointment information. A phone tree for those calling 311 directs callers seeking mpox information to a DOHMH call line to speak with qualified nurses.
Another avenue of community outreach is through social media. Many people, including the LGBTQ+ community, receive news through Twitter, Instagram, and other social media outlets. Leveraging those platforms correctly can ensure that accurate health information reaches the intended audience. NYC H+H/Bellevue physicians have collaborated with NETEC to provide much-needed information to clinicians, researchers, and patients alike. Near-weekly NETEC newsletters, sent via email, have featured mpox updates since May 20, 2022. 24 Subscription to the newsletter is free and contains links to other NETEC educational materials, their resource library, situation reports, blog posts, and more.
When developing community outreach campaigns, one should consider how messaging may be received. The term “mild illness” can understate the severity of the symptoms that patients are experiencing, which can be very painful, debilitating, and drastically decrease the quality of life. Supportive care is still needed to mediate pain resulting from oropharyngeal, urogenital, and rectal lesions. 25
Discussion and Conclusions
Mpox is quickly spreading around the world. Although it has been primarily affecting social networks of MSM, it is not considered a classic sexually transmitted infection.5,16 Any activities that involve skin-to-skin contact, like kissing or hugging, can also transmit the virus. 16 Transmission outside networks of MSM has occurred, and at some point, it may circulate among the general population. 11 The rapid increase in the number of mpox cases in New York City demanded a swift response from federal and local governments as well as local health systems. Safety net hospitals, such as NYC H+H/Bellevue, have a specialized role in ensuring that historically marginalized populations receive the attention they deserve. The hospital's strategy of using their special pathogens unit to lead the response until transmission dynamics were better understood and care could be routinized was a sensible use of resources. Both interfacility and intrafacility partnerships were critical to a cohesive response.
For hospitals preparing for this outbreak or future outbreaks, we advise identifying a multidisciplinary team of doctors, nurses, epidemiologists, and pharmacists within their facility to respond to such an emergency. This team should establish protocols for screening, testing, treatment, vaccination, inpatient care, patient transportation, and EMR tracking. These individuals should also develop and provide routine PPE training and just-in-time training to staff during an activation. The early identification of this team will ensure the facility is in a position to provide the best care to patients and reduce the spread of the virus. Additionally, discussions should be held among leadership staff to identify clinic space to establish a testing center, develop staffing redistribution plans to meet the needs of an activation, allocate funds toward maintaining PPE supplies, establish relationships of collaboration with applicable health departments, and invest in staff training so more physicians and nurses are prepared to provide care to a special pathogen patient.
In striving to provide high-quality, patient-centered care, we must be cognizant of the trauma that MSM experienced during the early days of the HIV/AIDS outbreak and avoid repeating those mistakes today. Hospitals should create plans for interdisciplinary inpatient and outpatient care in close collaboration with local public health departments to maintain the standard of care in an equitable, humane way.
The emergence of mpox outside of Sub-Saharan Africa shortly after the novel SARS-CoV-2 outbreak in 2020 highlights a recent acceleration in the frequency of special pathogen outbreaks. It is only a matter of time before the next special pathogen arrives on our shores, making preparation of staff, space, and materials increasingly imperative.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Tania Kupferman—director of the Antimicrobial Stewardship Program at NYC H+H/Bellevue and Department of Medicine, NYU Grossman School of Medicine—for her work on the mpox treatment workflow. In addition, the authors acknowledge Isaac Holmes, the medical director of ambulatory care, for his essential role in obtaining the resources to establish mpox testing. We thank Nicole Huff, senior director of communications at NETEC, for developing mpox resources physicians rely on with a focus on patient-centered care. Vikramjit Mukherjee, Amanda Klinger, Justin Chan, Patricia Tennill, and Anthony Lo Piccolo are members of Region 2's RESPTC at NYC H+H/Bellevue, which receives funding from the Administration for Strategic Preparedness and Response.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.