
Abstract
This study aimed to determine optimal mitigation strategies in the event of an aerosolized attack with Bacillus anthracis, a category A bioterrorism agent with a case fatality rate of nearly 100% if inhaled and untreated. To simulate the effect of an anthrax attack, we used a plume dispersion model for Sydney, Australia, accounting for weather conditions. We determined the radius of exposure in different sizes of attack scenarios by spore quantity released per second. Estimations of different spore concentrations were then used to calculate the exposed population to inform a Susceptible-Exposed-Infected-Recovered (SEIR) deterministic mathematical model. Results are shown as estimates of the total number of exposed and infected people, along with the burden of disease, to quantify the amount of vaccination and antibiotics doses needed for stockpiles. For the worst-case scenario, over 500,000 people could be exposed and over 300,000 infected. The number of deaths depends closely on timing to start postexposure prophylaxis. Vaccination used as a postexposure prophylaxis in conjunction with antibiotics is the most effective mitigation strategy to reduce deaths after an aerosolized attack and is more effective when the response starts early (2 days after release) and has high adherence, while it makes only a small difference when started late (after 10 days).
Introduction
Bacillus anthracis, a gram-positive rod, is a category A bioterrorism agent that can be weaponized for aerosol dispersion. Anthrax is a complex infection with within-host dynamics that may result in late germination of spores after inhalation and multifactorial environmental, weather, and attack factors that determine the spore density, dispersion, and impact of an attack. Several studies have estimated the impact of an aerosolized attack using various modeling approaches informed by historical anthrax incidents.1-7 Anthrax's most common natural manifestation is cutaneous, but it may also present as gastrointestinal, inhalation disease, or meningitis. Inhalational anthrax has a case fatality rate of nearly 100% if untreated, 8 causing severe breathing problems and shock, 9 and should raise suspicion of a deliberate release. The US anthrax attack through the postal service in 2001 resulted in 11 inhalational and 11 cutaneous cases of anthrax and, with the use of antimicrobials, 6 of the 11 inhalational cases survived. 10
In addition to the treatment of ill patients, mitigation of potential exposure requires identification of extent of the zone of contamination. Postexposure prophylaxis (PEP) with antibiotics and vaccines 11 of exposed people is effective, but there may be uncertainty around defining the exposed population and estimating the attack size and the radius of exposure. The mainstay of PEP is antimicrobials, usually ciprofloxacin or doxycycline, given as soon as possible after exposure and continued up to 60 days, 12 as spores may remain in the body and germinate after the initial attack. Determining the extent of potential exposure in real time during an attack is challenging, and the precautionary principle may need to be used in the face of uncertainty, given the severe consequences of infection. During the US attack, which resulted in 22 clinical cases, 32,000 persons received antimicrobial prophylaxis, with 10,300 completing the 60-day recommended course. 10 However, in this case, the primary attack was through envelopes in the mail, resulting in a small-scale aerosolizing event. In a direct aerosolized attack, a much larger radius of exposure would be expected, and correspondingly, PEP may need to be more widespread.
Vaccines can also be used as PEP but immunity is acquired after 28 days; however, antimicrobials are recommended to be continued up to 60 days. 12 Hence, the primary value of vaccination is in protecting against late germination of sequestered spores within the body. 13 Since the US Food and Drug Administration-licensed anthrax vaccine adsorbed (trade name BioThrax) 14 was developed in the 1950s, a few newer anthrax vaccines have been in development. Anthrax vaccine adsorbed (0.5 mL at 0, 2, and 4 weeks) can induce neutralizing antibodies against the protective antigen, the cell-binding component of anthrax toxin. 12 AV7909 (trade name NuThrax) is a second-generation anthrax vaccine in Phase 3 clinical trial 15 and may elicit a faster immune response. Other vaccine and approaches also show promise.16,17 Vaccines and antibiotics for an anthrax attack need to be stockpiled as medical countermeasures to ensure a rapid response. 18
The evidence for the efficacy of PEP comes mainly from animal trials and modeling studies but suggests that PEP with a combination of antimicrobials and vaccines is superior to antimicrobials alone. 19 It should be noted that no late anthrax cases occurred in people taking antimicrobial PEP following the US attack, but this was not a large-scale attack and the true number exposed is uncertain. Other unforeseen complications of a response may arise, which cannot be neatly predicted by modeling. 20 In the US attack, 20 which was a small-scale aerosol attack using the postal system, the spores (ranging from 3 to 5 micrometers) were dispersed widely in the postal facilities through the action of mail-sorting machines. 20 This resulted in the need for a large-scale response, but the anthrax vaccine was not licensed, not in the stockpile, 18 and required procurement from the military. This, combined with hesitant and conflicting communication by uncertain public healthcare providers and the requirement for contacts to sign lengthy consent forms to receive the vaccine as an investigational product, 20 resulted in long delays. By the time the vaccine was available, it was clear no new cases had occurred, so the perception of risk had reduced. The net effect was low vaccine uptake (199 people accepted vaccine, whereas 1,700 received extended prophylaxis of 100 days). The risk of biological attack with B anthracis remains real, requiring evidence-based planning to mitigate such an event.
Few published models1-7 are available for estimating the impact of a weaponized B anthracis attack, and even fewer account for atmospheric spore dispersion. 21 The available models use different approaches in terms of atmospheric dispersion, age-dependent dose response, disease progression, and spatial distribution. For policymakers and responders, dispersion (plume) modeling can assist with estimating the affected area of contamination and the resulting requirements for prophylaxis, vaccination, and decontamination. A model that uses some form of dispersion modeling would give the best estimate, especially if wind conditions, weather, and topography are considered. Models that do not use these parameters may underestimate or overestimate contamination, depending on the specific context. An essential factor to consider is that most available B anthracis attack modeling studies use simplistic dispersion models, if at all, and lack thorough validation.
Our study aimed to determine optimal prevention strategies for the Australian population, accounting for immunosuppression and PEP with antibiotics and vaccines in the event of an aerosolized attack with B anthracis to inform adequate stockpiling for a small-, medium-, and large-release scenario.
Methods
Our study focused on prevention with vaccines and PEP. Treatment of acute cases of anthrax was not included. To simulate the effect of a B anthracis attack, we used a plume dispersion model, accounting for weather conditions, and used the greater metropolitan area of Sydney, Australia, with a population of 5.4 million people as a case study. We determined the radius of exposure in different attack scenario sizes (small, medium, large) and different weather conditions to estimate the potentially exposed population in the event of an attack. We then estimated spore concentration and used the exposed population and spore concentration to inform a Susceptible-Exposed-Infected-Recovered (SEIR) deterministic mathematical model to calculate the number infected, and the antibiotics and vaccination doses needed.
Dispersion Modeling of a Weaponized Bacillus Anthracis Release
Dispersion modeling of weaponized B anthracis release was done in 3 steps:
The modeling is based on 3 different time periods and weather conditions, along with 3 different release amounts from the same location. These cases were chosen to cover a broader range of potential scenarios and to understand the impact of the prevailing weather conditions.
Scenario 1 – Release of 1 g/sec for 1 hour (small attack); same time period.
Scenario 2 – Release of 2 g/sec for 1 hour (medium attack); same time period.
Scenario 3 – Release of 4 g/sec for 1 hour (large attack); same time period.
Scenario 4 – Release of 2 g/sec for 1 hour (medium attack); different time period.
Scenario 5 – Release of 2 g/sec for 1 hour (medium attack); different time period.
The detailed methodology, model specifications, and the geospatial plume dispersion figures are provided in the Supplementary Materials (www.liebertpub.com/doi/suppl/10.1089/hs.2022.0100).
We used data from the dispersion model to estimate the number of people exposed and the spore density of exposure to inform the SEIR model for prophylaxis requirements. The spore concentrations for different zones were calculated based on the assumption that there are 1 trillion spores in 1 g of weaponized B anthracis. 24 Once we had the different areas of spore concentrations, we used data on population density to count the number of people exposed and infected, used as initial conditions in the SEIR model.
The Australian Bureau of Statistics census data for destination zones include the place-of-work population and commuting patterns. 25 We estimated the daytime population per destination zone by adding the place-of-work population in the zone and the children population up to secondary education with usual residence in the same zone. As the geographic boundaries of destination zones and the areas of anthrax exposure are different, the intersection of the 2 data points on a pro rata basis was applied to the calculations for population exposure.
Anthrax SEIR Model
Few studies have estimated the length of the latent period,26-28 which showed similar findings on an average incubation period dose inhaled dependent; however, only Brookmeyer 26 estimated them by age. We therefore used data from Brookmeyer 26 on the duration of the incubation period by inhaled spore concentration and age (ie, 2 age groups: 40 years and under and over 40 years). Details are in the Supplementary materials. To include the effect of the immunocompromised population, we considered 25% and 33% shorter incubation periods, respectively, for mildly and severely immunocompromised populations; this is an assumption made due to the lack of data. We estimated in a previous study 29 that in Sydney 1.7% and 6.1% of the population are severely immunocompromised, while 5.1% and 21.8% are moderately immunocompromised, respectively, for the age groups 40 years and under and over 40 year. To include the effect of the immunocompromised population, we weighted the duration of latency for severely and mildly immunocompromised populations. Lastly, the spore concentration inhaled to infect respectively low, medium, high and very high percentages of exposed people was estimated in the fourth edition of the anthrax guidelines from the World Health Organization. 30 The Figure shows the schematic of the SEIR mathematical model, and all parameters used are shown in Table 1.
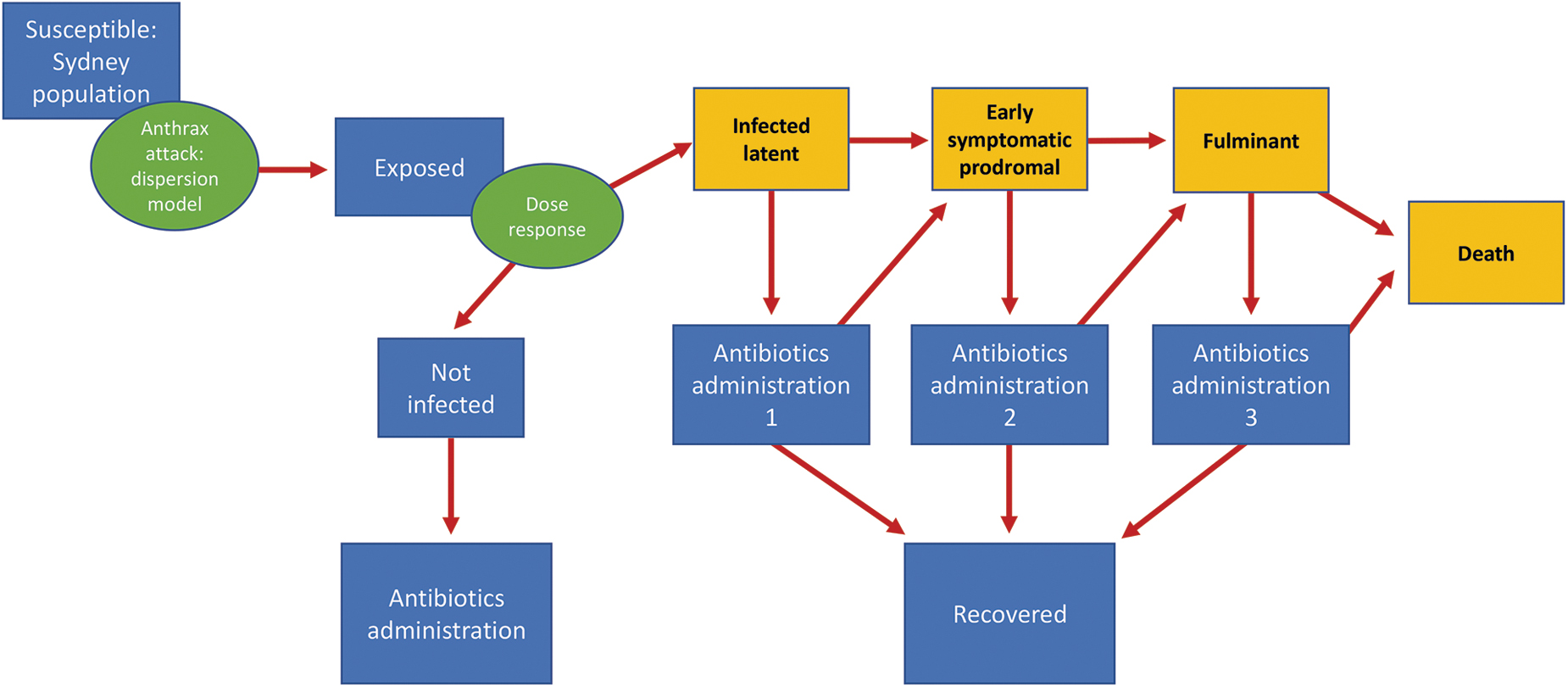
Schematic for SEIR mathematical model of anthrax infection.
Parameters Used for Model
High adherence is defined as 80%, 95%, and 100% adherence during the 3 epidemiological states.
Low adherence is defined as 40%, 65%, and 90% adherence during the 3 epidemiological states.
We considered the Sydney population as totally susceptible. Following the release of B anthracis calculated from the dispersion model, and using population estimates in different affected areas, we estimated the number of people exposed and infected for 5 different spore densities per cubic meter, as previously explained.
We assumed early symptomatic and fulminant duration to be 2.35 and 1.41 days, 31 respectively. Antibiotic effectiveness (to stop the infection progressing to the next stage) depends on the starting epidemiological state: latency, early symptomatic, and fulminant. We assumed 90% effectiveness if started in latency31,32 as a PEP; 60% effective if started as treatment in the early symptomatic phase, which is the midpoint of the 2 previous estimates of 40% 33 and 80% 6 ; and only 3.2% effective if started in the fulminant stage. 6 These estimates account for hospitalization of severe cases. We assumed 3.8% and 13.0% of the population are severely or mildly to moderately immunocompromised respectively. 29 While there are no data on anthrax in immunosuppressed people, available studies show that ciprofloxacin has reduced efficacy in immunocompromised people. 34 To account for the immunocompromised, we weighted the effectiveness for the mild to moderate and severe immunocompromised percentage of the population, assuming them to have a 25% and 33% reduction in effectiveness respectively. Regarding vaccination, studies show that the effectiveness is between 93% and 95%.35,36 There are no data on vaccine effectiveness in immunocompromised people, but reduced vaccine effectiveness is seen with other vaccines. 37 We assumed vaccination has the same effectiveness for all age groups; however, we weighted the vaccination effectiveness to include the effect of 3.76% and 12.95% 29 of the population being severely immunocompromised (ie, 33% reduction in effectiveness) and mildly to moderately immunocompromised (ie, 25% reduction in effectiveness), resulting in a weighted estimate of 90% effectiveness.
We assumed that the probability of starting the antibiotics cycle is 80%, 90%, and 100% in latent, early symptomatic, and fulminant states, respectively. Furthermore, an estimated 80%, 95%, and 100% in latent, early, and fulminant states would adhere to the 60-day antibiotics respectively (high-adherence scenario). We added a sensitivity analysis of 40%, 38 65%, and 90% of adherence (low-adherence scenario) for the 3 epidemiological stages. After weighting for immunocompromised and antibiotic adherence, we obtained the effectiveness shown in Table 1 by the epidemiological state of starting uptake and age groups. Vaccination is assumed to be given to 90% of all the exposed population, with an effectiveness of 90%3,32,33,39 in a latent presymptomatic state; however, the vaccine will become effective after 28 days from uptake. People already symptomatic are assumed to not get the vaccine, as the vaccine effectiveness for someone already infected and symptomatic is considered to be 0%. It should be noted that vaccine logistics is not considered in the model. We have estimated that in an emergency, 150,000 to 300,000 vaccination doses could be delivered in 1 day. During the COVID-19 pandemic, major mass vaccination infrastructure was established, including vaccination hubs, which individually delivered up to 1,400 COVID-19 vaccinations a day. 40
The model estimates deaths for each scenario tested. Once exposed people are vaccinated, they will have a 90% chance of recovery after 28 days. However, if they are not treated within 28 days, they may develop symptoms and die. Vaccination will also prevent disease in those people who fail to adhere to the entire course of antibiotics. Therefore, in our model, we use vaccination and antibiotics together, as they are more effective than either alone. 41 The calculation of how many vaccine doses and courses of antibiotic prophylaxis are required in the optimal situation, where it is assumed that every exposed person will get antibiotic prophylaxis and be vaccinated, is derived from the total number of people exposed based on the output of the dispersion model.
As we know the number of people infected by exposure levels (Table 1), the infected latent category represents a matrix by 2 age groups and 4 levels of spore density exposure, which determines the length of the latent period as previously described. In this category, people can use antibiotics and suppress the disease symptoms until the vaccine becomes effective, and then either move to recovery or stop using antibiotics and move to the early symptomatic stage. Once symptomatic, people can adhere to antibiotics and recover with a lower probability of antibiotics effectiveness or move to the fulminant stage with a low likelihood of surviving. The differential equations of the SEIR model are in the Supplementary Materials (www.liebertpub.com/doi/suppl/10.1089/hs.2022.0100).
Results for Scenario 3 (large attack) with sensitivity analyses on adherence to antibiotics, time starting intervention, and response with and without the addition of vaccinations as PEP are shown in the following section, while the same results for scenarios 1, 2, 4, and 5 are shown in the Supplementary Materials.
Results
When comparing the small-, medium- (results shown in the Supplementary Materials), and large-release scenarios with 1 g, 2 g, and 4 g of spores released per second, respectively, the number of deaths, compared with the small-release scenario, almost doubles for the medium release but increases by 4.5 to 4.7 times with the large release. Table 2 shows the results for the worst-case scenario of the dispersion model (Scenario 3). The remaining scenarios 1 and 2 for small- and medium-size attacks are shown in the supplementary materials. For Scenario 3, the total number of exposed people to any concentration of spores is 347,855, with 87,855 exposed to the highest concentration zone. For the small- and medium-release scenarios (1 and 2), an estimated 495,369 and 502,857 people were exposed and a total of 63,687 and 123,054 people were calculated as infected, respectively. The worst-case scenario (Scenario 3) affected a 231 km2 of area and exposed 508,358 people, with an estimated 347,855 people infected.
Results From the Plume Dispersion Model and Initial Conditions Used in the Anthrax SEIR Model
Using Sydney age distribution of 53% in ≤40 years old and 47% in >40 years old, population infected 347,860 (n ≤ 40 years old and >40 years old).
For Scenario 3 (Table 2), vaccination is required for 508,358 people exposed, and 60 days of antibiotics for the same population translates to 30,501,480 daily antibiotic doses.
However, the following results account for people not starting any PEP and people not adhering to 60 days of antibiotics (results shown are for low- and high-adherence scenarios).
Table 3 shows the number of deaths with a delay of 2, 5, and 10 days following the spore release of vaccine and antibiotic distribution. This information provides a quantitative measure of the impact of any potential delays in response, with the number of deaths and daily antibiotic doses used. This number represents the total days of treatments required, summing all people treated.
Total Number of Estimated Deaths and Required Doses of Vaccine and Antibiotics
Antibiotics stopped after 28 days.
High adherence is defined as 80%, 95% and 100% adherence during the 3 epidemiological states—latency, early symptomatic, and fulminant.
Low adherence is defined as 40%, 65%, and 90% adherence during the 3 epidemiological states—latency, early symptomatic, and fulminant.
If vaccination is added to antibiotics as a PEP, there is a reduction in the number of deaths of 25.4% and 20.2% for high- and low-adherence scenarios, respectively, if intervention starts after 2 days; 15% and 12.9% if response starts in 5 days; and 6.9% and 6.4% if response starts after 10 days. In the scenario where vaccine and antibiotics are used, the reduction in deaths is 21.9%, 7.7%, and 6%, respectively, if intervention starts after 2, 5, and 10 days when the adherence increases from the low-adherence assumptions (ie, 40%, 65%, 90%) to high-adherence assumptions (ie, 80%, 95%, 100%).
Scenarios 4 and 5 with medium release were added to show the impact that different weather conditions can have on spore dispersion, and consequently the number of people exposed and infected. Indeed, with the same release of 2 g/sec of spores we showed 3 different directions of the plume dispersion in Supplemental Figures 2S, 4S, and 5S (in Supplemental Materials www.liebertpub.com/doi/suppl/10.1089/hs.2022.0100), and they resulted in an exposed area of 177, 181, and 136 km3; however, as population density changes in different areas, those scenarios resulted in 502,857, 449,435, and 483,131 people exposed and 123,054, 247,165, and 302,910 people infected, respectively. Therefore, Scenario 5, where a smaller area was impacted, resulted in the highest number of people infected.
Our research shows that vaccination used as a PEP in conjunction with antibiotics is the most effective mitigation strategy to reduce deaths after an aerosolized attack and is more effective when the response starts early (2 days after release) and has high adherence, while it makes only a small difference when started late (after 10 days). Furthermore, wind direction and weather conditions can double the number of exposed or infected people with the same quantity of spore released.
Discussion
An attack with weaponized B anthracis may have a substantial health impact in a large city such as Sydney. The dispersal of spores would depend on the location of release, weather conditions, and wind direction. In a coastal city with favorable winds, however, much of the plume could be blown seaward. In this study, CALMET and CALPUFF modeling systems were used to simulate the dispersion of the B anthracis spores following release in Sydney. The outcome of the model was geographical areas of different spore concentrations that, together with data on population densities and percentages of infected people by exposure levels, were used to calculate the total number of exposed and infected people. Those numbers were then used in an SEIR model to calculate the burden of disease and quantify stockpile needed.
However, no attack of the scale in our scenarios has ever been documented. The largest-scale aerosol event was the Sverdlovsk accident in the former Soviet Union, which resulted in a lower estimate of 66 deaths and 77 total cases occurring at least 4 km downwind from the site of release. 42 Nonetheless, our study highlights the principle that combined use of antibiotics and vaccine as PEP would save the most lives, especially if started early, no matter the size of an attack. We estimated the impact of different quantities released and different weather conditions to inform adequate stockpiling of vaccine and antibiotics, but based on historical precedents such as the 2001 US anthrax attacks and Sverdlovsk leak, the worst-case scenario is unlikely to occur.
The possible ways to release B anthracis spores are infinite. We focused on 5 scenarios in Sydney, a city of 5.4 million people. This is the first study to illustrate the impact of vaccines as part of PEP and to account for the estimated immunocompromised proportion of the population and for population adherence to PEP. Furthermore, we used a Gaussian puff-based dispersion model tailored to estimate dispersion spores for wind characteristics in Sydney and the terrain of the Sydney region. Timing of PEP, use of vaccines in addition to antibiotics, and adherence are influential.
The present study has some limitations. First, the data available to estimate parameters are limited. The last unnatural outbreak of anthrax in humans was in 2001 in the United States, which was not an aerial attack and reported only 22 cases with 5 deaths. 10 Data from that attack, despite modeling efforts,43,44 are not sufficiently useful for the estimation of the latent period due to the lack of information on the dose at which the victims were exposed. 45 The largest available well-studied outbreak was in the former Soviet Union in 1979, 42 in which 77 individuals were reported infected and fewer than 70 died.46,47 The latter outbreak is the only event with enough data to determine the level of exposure (ie, dose) and the incubation period 27 including the time of exposure (estimated to be 1 day), the disease strains, and the particle size (estimated as 5 μm to 10 μm from the victims' geographic position). 48 (The 1979 and 2001 data sets are available in the Supplemental Appendixes, www.liebertpub.com/doi/suppl/10.1089/hs.2022.0100.) Using this dataset, the previous estimation of the dose-dependent incubation period goes from 7 to 12 days.26,28,48 We chose to follow Brookmeyer's estimation 26 but we modified it to include the effect of immunocompromised people. We accounted for the immunocompromised proportion of the population and assumed they would have a more severe outcome; however, the percentage reductions of 33% and 25% used for the latent period and vaccine/antibiotics effectiveness were assumptions because there are no data available to inform the estimates. Results are for the metropolitan area of Sydney, but we do not know how well they can be generalized for other places using population age distribution and density data, and for specific weather and wind conditions.
Sensitivity analyses were done on adherence to PEP for 60 days without interruptions but not on acceptance of PEP. For vaccination acceptance we assumed 90% acceptance, as Australia has high vaccine acceptance. For example, 95.9% of Australians 16 years and older had received 2 doses of COVID-19 vaccines as of November 16, 2022. 49 Another limitation is that we did not account for vaccine and antibiotic delivery logistics and delays. This would overestimate the effectiveness of vaccines and PEP.
Additionally, the dispersion modeling results reveal that the dispersion of B anthracis spores can be highly variable depending on the initial attack size (amount of weaponized B anthracis released) and the prevailing weather conditions and wind direction. Furthermore, use of the dispersion model in real time to predict the number of exposed people is limited without knowing the number of spores released, and the place and time of the release. 50 Therefore, in the absence of real-time models, we estimated stockpiling requirements and highlighted the importance of using vaccine as PEP, for different scenarios of release and by adherence to PEP. The spore distribution presented is based on 3 different time periods and for 3 different release amounts. For different time periods, the direction and size of the plume vary based on the weather conditions; hence the risk zones could be very different based on the time of the attack and may have much lower impact in a coastal city if the wind drives the plume mostly over the ocean. Also, the population exposure in this study is static and can be considered as the total exposure over time. Population data with temporal variations, such as Google Mobility data, may be used for future work to account for time sensitivity to population exposure.
Although our study shows response estimates for a limited number of attack scenarios, the methods and models can be used to estimate the number of people exposed and infected, consequently inform optimal stockpile levels of prophylaxis with antibiotics and vaccines for a worst-case scenario. Notably, during the US anthrax attack in 2001, the procurement of vaccines and lack of an immediate mechanism to deploy them led to delays and low compliance. 51 In preparedness planning for a range of scenarios, stockpiling and using vaccine and antibiotics as PEP will result in the best outcomes.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.