
Abstract
Despite decades of US government attention to biological threats, COVID-19 revealed substantial deficits in US preparedness. In our evaluation, we sought to catalog and quantify information delivered to members of Congress that would enable them to determine their level of concern about emerging infectious disease (EID) risk and direct a course of action. We examined hearings on EID from 1995 through 2019 as a proxy for congressional awareness of EID risk, searching the Congressional Record using keywords. During this timeframe, Congress conducted 167 hearings relevant to EID, encompassing 860 witness appearances. The most active House and Senate committees were those with jurisdiction over homeland security, health, oversight, and funding. There was a markedly lower level of activity among committees with jurisdiction over foreign relations, financial services, small business, agriculture, and every other relevant area of jurisdiction. Our results suggest that absence of lawmaker knowledge of EID risks was not the cause of the United States' lack of preparedness.
Introduction
The consequences of the COVID-19 pandemic to human life and economic activity have driven many to ask why the US government was not better prepared for this historic moment. The notion that an infectious disease outbreak could have vast consequences for human and economic health, and that the nation needed to prepare for such contingencies, was not new to government officials. President Bill Clinton is widely credited with setting in motion a governance structure and programs designed to counter his administration's perception of a mounting bioterrorism threat,1,2 while also initiating the first major effort to strategically address the burgeoning global health threat of emerging infectious disease (EID) through enhanced global engagement. 3 These activities continued under President George W. Bush, with increased emphasis on bioterrorism after the anthrax attacks of 2001. 4 In addition, an increase in biothreat activity related to influenza and other potential sources of viral pandemics can be found in the annals of the Barack Obama presidency. 5 Many biodefense programs funded during these years continued under President Donald Trump. Each of the Congresses in power across these presidencies concurrently pursued oversight, authorizing legislation and funding bills that enabled this work.
The measurement of government and specifically of legislative branch productivity is the subject of extensive political science inquiry.6-9 A common metric for legislative branch progress is the number of bills passed.10,11 The authors are unaware of studies that have systematically assessed authorizing legislative outputs on biodefense policy matters. Even so, legislative activity with respect to biodefense has not widely been a perceived bottleneck to progress; new legal authorities to implement biodefense programs have rarely been needed, although Congress has provided some statutory backing in areas like creation of a national stockpile, provision of medical countermeasure contracting and regulatory authorities, and establishing leadership authority for public health and medical response to biological emergencies.12-15
Another way to measure government effort is through expenditures, or legislative outputs in the form of appropriations bills. One annual evaluation estimated that biodefense spending, based on congressional appropriations, has ranged from $4.9 billion to more than $11 billion annually since 2001,16-18 with funding for the subcategory of “civilian pandemic influenza and emerging infectious disease” at $1.3 billion in fiscal year 2010 and reaching as high as $1.5 billion by fiscal year 2018. Spending increased after the Ebola virus disease emergency prompted congressional appropriations during fiscal year 2015 to support domestic and global response. 18 Funding for “global health security” as its own category has also waxed and waned over time but has generally been in the area of $400 to $500 million annually over the last decade. 19
In this evaluation, we assessed inputs—that is, information delivered to decisionmakers that would enable them to determine their level of concern and direct courses of action, such as through federal programs and appropriations. Through cataloging congressional hearing activity, the authors examined to what extent Congress was aware of the risk from EID in terms of threat, vulnerability, consequences, and/or the federal activity being undertaken or requested to address that risk.
Methods
The modern biothreat can be viewed as a tripartite construct that consists of emerging infections from nature, intentional acts, and accidents. 20 Preparedness for that threat may be specific to 1 of those elements, to individual pathogens of concern, or may be approached generally as “all hazards.” This study was designed to capture lawmakers' awareness of the threat of emerging infections, or EID, and the risk to the United States from that threat, whether through direct education on the threat or risk, or indirectly through education on programs designed to address them. For the purpose of this study, we considered EID to encompass those kinds of outbreaks caused by nonendemic pathogens: newly emerging or recently emerged infectious diseases; reemerging infectious diseases; and others that may be endemic in certain locations or species but which then appear in nonendemic areas or species. We did not seek information related to intentional acts and bioaccidents.
The Congress.gov website 21 was used as a primary source of information on congressional activity by way of the Congressional Record, which is maintained in the database beginning with the 104th Congress (1995-1997). The Congressional Record was chosen because it captures committee activity in the form of titles and descriptors (when available) of hearings, briefings, and business meetings. We used keyword searches to return records from the beginning of the database's availability through December 31, 2019, marking the approximate beginning of awareness of COVID-19, and enabling us to consider all hearings from the first session of the 116th Congress. We searched for the following terms: biodefense; biological threat; biopreparedness; biosurveillance; biothreat; CBRN; chemical, biological, radiological, and nuclear; coronavirus; Ebola; emerging infectious disease; global infectious disease; health security; infectious disease epidemic; influenza; MCM; medical countermeasure; medical preparedness; medical readiness; medical supply chain security; MERS; Middle East respiratory syndrome; pandemic; public health response; SARS; severe acute respiratory syndrome; and Zika. Results were exported into a comma-separated values file. We reviewed these records for the 2 types of hits that contain information on committee activity, the Daily Digest and Senate committee meetings. We reviewed each record and categorized the activity it represented as a hearing, briefing, or business meeting. Hearings were the primary unit of interest, as they represent one of the most public forms of congressional oversight and information gathering. Briefings are often not formalized or noticed in the Congressional Record; because the number of briefings listed thus would be an insignificant fraction of the briefings that members would actually receive during their time in Congress, search results representing briefings were removed from the analysis. Business meetings almost always represent markups of legislation; these data points were also removed.
Search parameters were designed to exclude bioterrorism-specific hearings, but they sometimes still appeared in the data captured. After we identified all of the hearings consistent with the search terms, we excluded those that were solely targeted to terrorism, based on the titles or descriptions provided in lieu of titles. Some hearings covered both topics or used the topic of bioterrorism to discuss broader preparedness efforts also relevant to EID, and these were included. This system required a judgment by the first author. Hearings that specifically addressed HIV/AIDS, tuberculosis, or malaria were excluded; these are major global health burdens, but fell outside the scope of emerging threats. Occasionally the search resulted in an announcement for an upcoming hearing but no actual notice confirming that the hearing took place; additional research through the Congress.gov website, 21 the US Government Publishing Office website, 22 or committee websites was undertaken to find a notice confirming that the hearing was held. Rarely no such notice could be found, and these hearings were excluded on the presumption that they had been canceled. The authors knew about the existence of 6 relevant hearings that were not captured by any of the keywords and included these for comprehensiveness (ie, the majority being appropriations hearings that did not explicitly mention EID in their titles but extensively discussed relevant expenditures). Witness names and affiliations for each hearing were noted from the Congressional Record and other sources, including official committee reports available at the US Government Publishing Office govinfo website 23 and committee websites. Names were manually standardized to resolve spelling or other discrepancies. Each hearing was tagged as having occurred during either Democrat or Republican control of a given chamber.24,25 Some committee names changed across the data capture period; hearings from committees with changed names were grouped with their names as of 2020 to permit proper committee-level analysis of activity. 26 All hearing duplicates were removed.
Results
Since 1995, Congress has conducted 167 hearings relevant to EID (Figure 1). The average number of hearings per year is 6.68, although congressional interest as reflected by hearings has not been constant but rather punctuated by bouts of activity. The extent of focus on this topic has been variable under both Republican and Democratic majorities.
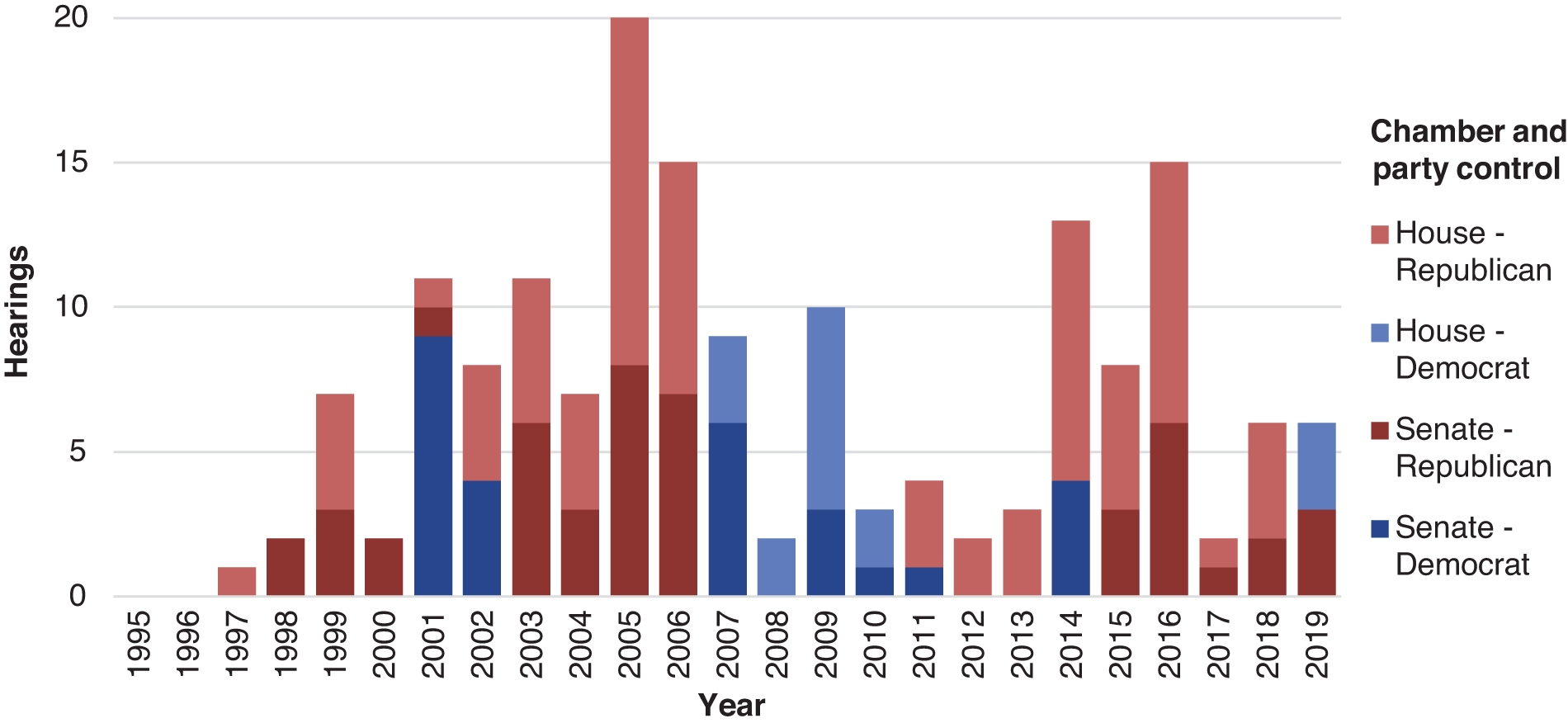
Annual number of congressional hearings on emerging infectious diseases from 1995 through 2019, categorized by chamber and party control. Note that party control of the Senate flipped partway through 2001.
The House of Representatives (n = 92) has been more active than the Senate (n = 75) in terms of absolute number of hearings; this is expected, as the House generally holds more hearings in a given year than the Senate. 27 In the House across the entire period of interest, the Committee on Energy and Commerce (n = 23) was the most active, followed by the Committee on Homeland Security (n = 18) and the Committee on Oversight and Reform (n = 15). In the Senate, the Committee on Homeland Security and Governmental Affairs (n = 21) was most active, followed by the Committee on Health, Education, Labor, and Pensions (n = 18) and the Committee on Appropriations (n = 16). When viewed collectively across the chambers, activity is emphasized in those with jurisdiction over health, homeland security, appropriations, and general government oversight (Figure 2). Foreign affairs committees come in at the next level, with 10 hearings in the House and 5 in the Senate, while financial services, small business, agriculture, and every other relevant area of jurisdiction show markedly lower or nonexistent activity.

Number of congressional hearings on emerging infectious diseases from 1995 through 2019 as categorized by committee and area of jurisdiction. All committees holding at least 1 hearing are shown. Hearings held jointly by 2 committees count toward both committees' totals. The most active committees collectively across both chambers by area of jurisdiction are color coded based on primary area of jurisdiction; because the Senate Committee on Homeland Security and Governmental Affairs is both a homeland security and a general government oversight committee, it is color coded as both. Committees are labeled using their modern names as of 2020.
Hearing topics varied over time and by committee jurisdiction. Hearings on particular infectious disease events drove much of the annual variability in the number of hearings held (Figure 3). Additionally, even at hearings not structured to examine any particular disease event, we often encountered extensive discussion of contemporaneous disease events and their policy implications.

Congressional hearings on emerging infectious diseases by hearing topic. Number of hearings by year from 1995 through 2019, color-coded with hearings that were about or focused on 1 of 7 key outbreaks. Abbreviation: DRC, Democratic Republic of the Congo.
In addition to discussing the details of contemporaneous disease events, witnesses also provided warnings relevant to long-term preparedness efforts. In many cases, witnesses forewarned gaps in preparedness that have become apparent during the national response to COVID-19 (Table).
Table. Examples of Warnings from Statements and Testimonies at Congressional Hearings on Emerging Infectious Diseases, 1995 to 2019
Authors' analysis of sources returned from a keyword search of the Congressional Record and transcripts from congressional hearings retrieved from the US Government Publishing Office govinfo website. 23 The concept and some entries were adapted from a report, 25 Years of Pandemic Warnings: Health Security Net, A Global Health Security Library, published in January 2021 by the Georgetown University Center for Global Health Science and Security. 33
Abbreviations: EID, emerging infectious disease; Labor/HHS, Labor, Health and Human Services, Education, and Related Agencies; SARS, severe acute respiratory syndrome.
The number of witness appearances across all hearings was 860, with 551 unique individuals providing testimony (witness information is available in the Supplemental Material, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0205). Of the individuals who testified, the majority (n = 434) testified only once. Among all witness testimonies, 474 were provided by federal witnesses (excluding members of Congress), while the remaining 386 testimonies were given by a range of academics, international experts, state and local government officials, medical practitioners, former federal officials, current and former members of Congress, and others. Some experts appeared repeatedly. Anthony Fauci testified most often, appearing before Congress 43 times among the hearings captured. Julie Gerberding testified next most often (n = 20), followed by Anne Schuchat (n = 12), Tom Frieden (n = 11), Janet Heinrich (n = 11), and Tara O'Toole (n = 11). Although frequent testifiers tended to hold positions high within the executive branch, a set of outside experts also repeatedly appeared.
Discussion
Using publicly available information, we gathered written and verbal instances when EID information was provided to the legislative branch of the US government in the form of hearings. The goal was to determine the extent to which elected officials were exposed to information on naturally occurring infectious disease threats and the risk to the United States from those threats. This exercise, while valuable in an academic sense, is designed to be applicable toward current and future efforts to better understand the dynamics of policymaker decisionmaking, to improve methods for policymaker education and advocacy on EID threats, and to help Congress optimize its own oversight and policy action related to these threats.
Hearings as a Pathway to Knowledge and Action
Hearings are a critical path for the transmission of important information to decisionmakers; they may be used as a proxy for what legislative officials knew, or reasonably should have known, about EID. Hearings are of interest because they represent inputs to Congress—in this case, 860 witness appearances offering information that Congress could use to make decisions about policy and funding. The number of hearings and in particular of federal witnesses is important because these testimonies are essentially a bridge between the executive and legislative branches. They reflect an exchange of knowledge among the very individuals empowered to act upon that knowledge. They also offer a window into congressional priorities; hearings only appear on a committee calendar when a member of Congress decides to place them there. In this sense, the body of hearings since 1997 seems to reflect a strong interest on the part of Congress in EID threats and government activity needed to address them. Interest, however, does not equate to organized action and funding. Sometimes hearings serve as political statements unaccompanied by policy change. Other times, they result in outputs in the form of legislation that authorizes or funds activity, but that output may not be sufficient to meet the need. That is, outputs may not match inputs. Additional research might assess the extent to which the hearings documented here resulted in outputs such as proposed legislation, enacted laws, changes to funding levels, or increased oversight. Intra-action reviews, after-action reviews, and most likely a national commission on COVID-19 will assess the extent to which the outputs were either inherently insufficient or were ineffectively carried out. Other analyses may look to fields such as political psychology to unravel the ways that awareness of problems does or does not lead to action on the part of individuals and the institutions within which they function.
Other analyses have used congressional hearing activity to catalog how policymakers responded to high-profile emergencies and other disruptions, including, for example, terrorism. 34 Our collection of hearings similarly provides insight into the congressional response to particular EID emergencies. Congressional interest as reflected by hearings has been punctuated by bouts of activity at or around the time of health events of major concern: 2003 (severe acute respiratory syndrome, or SARS), 2005 (avian influenza/H5N1), 2009 (H1N1 pandemic influenza), 2014 and 2018 (Ebola virus disease), and 2016 (Zika virus disease). The spike in activity from 2005 to 2006 seems to reflect the pandemic influenza threat (ie, human cases of avian influenza were appearing in Asia at that time) and was also a time when the first Pandemic and All-Hazards Preparedness Act 13 was being drafted and debated in committee. It was also when the Senate Committee on Health, Education, Labor and Pensions established a Subcommittee on Bioterrorism and Public Health Preparedness; our search captured 6 hearings held by this short-lived subcommittee between 2005 and 2006, accounting for 17.1% of hearings held in that 2-year period. Congressional interest in EID as reflected in hearings never again approached that level during the timeframe analyzed here.
Reaction can be a positive sign that Congress is paying attention and drawing lessons from ongoing events. H5N1 in Asia prompted a focus on pandemic influenza originating from birds, but also on pandemic influenza generally, avian disease surveillance, and medical surge capacity. Yet solely reacting to each latest infectious disease emergency does not substitute for strategic planning and preparedness. Members of Congress are not simply accountable to their constituents, they depend on them for reelection, and prior research shows that voters reward disaster response, not preparedness. 35 Reaction is also easier than the laborious work of developing a detailed national strategy to address biological risk and holding routine hearings to ensure all of the boxes have been checked. These labor-intensive activities compete with more politically salient issues and the constant work of campaigning. Congress itself is poorly constructed to address complex interdisciplinary problems, with both its authorization committees and funding subcommittees siloed from one another and ill-equipped to advance collaborative solutions that acknowledge multisectoral risk. 36 Addressing these issues of electoral incentives, chronic campaigning, and inadequately construed committee oversight may help narrow the chasm between awareness and action.
Given the frequent and bipartisan nature of hearings cataloged here, our findings point past issues of partisan gridlock or a lack of congressional engagement, possibly indicating deeper pathologies in the electoral and other incentives facing lawmakers and the structure of Congress. The role of incentives and disincentives could be explored as part of efforts to understand why Congress makes the choices it does with respect to prevention and preparedness.
Committee Jurisdiction, Interest, and Activity
The far-reaching effects of COVID-19 demonstrate that many committees hold jurisdiction over some critical piece of EID oversight. Among authorizing committees, it is the health and homeland security committees that have taken the most interest in the infectious disease threat and the nation's readiness for it. In doing so, homeland security committees implicitly acknowledged that infectious diseases are national security issues. These committees, however, were relatively unempowered from their inception to create and enforce the systematic oversight and legislative activity that EID prevention, preparedness, and response requires. 37 Outside of the 2 homeland security committees, interest in this topic has been largely confined to the authorizing committees with purview over human health. This relatively constricted interest in the human health impacts of infectious disease may reflect a common framing of the biothreat: a tendency to think about it in terms of human health, although dozens of sectors are relevant for prevention, detection, response, and recovery, a reality that in turn must drive planning and implementation. 38 This may have manifested in the far more limited committee activity in, for instance, foreign affairs/relations, even though many of the hearings tallied for this study issued warnings that an EID was most likely to originate overseas, and that it would disrupt international trade, travel, and critical supply chains.39-41 The House financial services and small business committees each held only 1 relevant hearing in 25 years despite warnings about the projected costs of a pandemic and threats to financial structures.42-44
The House Committee on Education and Labor and the Senate Committees on Banking, Housing, and Urban Affairs; Finance; and Small Business and Entrepreneurship are among those that held no hearings. The same is true for House and Senate intelligence committees, and while many of those committees' hearings are classified and thus would not have been captured by the search, they are not all classified, and EID is a topic that can be discussed in open session. Much of the concern over how widespread COVID-19 was in the United States before its scope was understood relates to the extent to which it was an epidemic intelligence failure.45,46 The intelligence committees' jurisdiction is implicated not only based on COVID-19 but also by the decades of warnings about infectious diseases and pandemics issued via the director of national intelligence's annual Worldwide Threat Assessments.
Appropriations committees are unique in their role not as authorizers (although they are often de facto authorizers) but in carrying the power of the purse. They are the only committees that can directly influence the amount of money available to the executive branch for EID and related activity. The House appropriations committee (or its subcommittees) held 10 hearings, and its Senate counterpart held 16, reflecting 15.6% of the total hearing activity. Some of this activity was part of routinized appropriations oversight in advance of annual spending decisions, while some—like their authorizing counterparts—reflected a reaction to current events, such as avian influenza, pandemic influenza, and Ebola virus disease.
For context, one might compare the number of EID hearings with those that Congress held on other issue areas. One study identified the number of climate change hearings from 1969 through 2007 and found 253 hearings and 1,350 testimonies, an average of 6.5 hearings per year, 47 which is comparable to this study's findings. One might also compare with another key national security topic, that of terrorism. Terrorism as a category may be too broad a comparator, one that is more akin to “health” overall than EID as a subset of health. One review of “subsystems” of terrorism (ie, a given policy area within the larger terrorism umbrella) found hearing tallies from 1988 through 2004 comparable to this study's findings—national disaster preparedness and response (n = 199), food safety (n = 112), public health emergencies (n = 122)—although some categories received considerably more activity (such as domestic preparedness, n = 332). 34 On balance, the level of EID hearing activity is relatively consistent with that of other national security topics; Congress held what might be deemed a reasonable number of hearings to educate itself on EID issues. Yet that hearing portfolio was imbalanced across committees of relevant jurisdiction. The oversight for this activity might have been shared across many congressional committees, but was restricted to a small few. Dealing with the complicated matter of EID requires an interdisciplinary, multisectoral approach at the implementation level, 38 and the same principle could have been applied to Congress' oversight of the problem.
Hearings as a Proxy for Awareness: An Important but Limited Metric
The list of hearings captured is conservative. Search terms did not include biological terrorism, biological warfare, laboratory biosecurity, or related terms. The exclusion of these terms could have excluded hearings at which natural infectious disease outbreaks and/or preparedness needed for any biothreat were discussed. Further, a keyword search of the Congressional Record captures hearings in which the search term is reflected in the hearing title, hearing descriptor, or witness affiliation; it does not reflect the hearing transcript, which would better reveal the extent to which hearings veered into oversight territory relevant to EID. For instance, each year, the director of national intelligence testifies on the Worldwide Threat Assessment findings. The Worldwide Threat Assessments offer a useful window into how engaged the US intelligence community was with EID and the ways in which, when communicating with policymakers, the US intelligence community framed EID as a national security threat. While these Worldwide Threat Assessment hearings are tangential to infectious disease matters and were not picked up by the search terms, our review of the director's written testimony for these hearings shows they have referenced the biothreat every year since 2006 (with the exception of 2007), beginning with their growing concern over H5N1 influenza. This written testimony provided an opportunity for lawmakers to be exposed to the director's concerns. In addition, at 5 of the annual hearings, the director also verbally mentioned pandemics or infectious disease threats; a review of the hearing transcripts shows that no members asked questions on this topic.48-52
This evaluation did not capture private member briefs, another important way by which members receive information without the public pressure or jurisdictional considerations of a hearing. These are essentially not documentable, but may be reasonably estimated to number in the hundreds and possibly thousands over 25 years. We also did not identify notices of classified briefings. It is further impossible to capture the number of times members read classified documents on the biothreat in secure facilities. It is also a challenge to account for the ways that attrition of members of Congress changes the overall congressional perception of the threat, and whether new versus experienced members receive the information in the same way.
Future Directions
Further research could evaluate member remarks on the House or Senate floors related to EID as a possible additional source of information exposure. Content analysis of the cited hearings and reports could help to ascertain and quantify their specific messages. Further work could also explore how executive branch understanding led it to enact policies and programs and to request funding and authorities from Congress to address the risk. The hearings and associated data are publicly available online (see Supplemental Material, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0205) and are included in the digital repository Health Security Net, 53 which comprises thousands of other US and global records that may provide context for this future research.
This study's natural limitations in assessing the extent to which lawmakers were briefed on the threat, understood the threat, and took actions that could meaningfully prevent or mitigate that threat create opportunity for further work by researchers or a national commission to better understand these dynamics. Exploration of the committee activity identified herein could improve understanding of how Congress's awareness of EID issues aligns to legislation, to implementation oversight, to funding levels and other resource allocation, and eventually to how well these elements align with outcomes. Understanding why, despite the decades of warnings, the country was unable to prevent and to adequately respond to COVID-19 could advance broad political science understanding of barriers that prevent policy change, the study of legislative productivity, and the measurement of federal government performance. It could also guide future efforts to address biothreats.
Conclusions
In the early days of the COVID-19 response, President Trump and some members of Congress stated that they were unaware of the threat of such a consequential pandemic as COVID-19, or of the extent of US vulnerabilities to that threat. Yet for more than 2 decades, Congress received official testimony across a conservative estimate of 167 hearings and 860 witness testimonies that communicated a real and growing infectious disease risk to public health and national security. These hearings elaborated on efforts that federal, state, and local governments were taking or should have been taking to counter that threat. They reflect a substantial scope of opportunity for awareness of threat, vulnerability, consequences, government programs, and governance structures relating to EID. They cover topics like preventing transmission of viral respiratory diseases; air travel's role in spreading disease; stockpile readiness; national surge capacity for biological events; hospital preparedness; the US response to SARS; impacts of influenza on small businesses and healthcare providers; and pandemic financing, among many others. That is, many of the issues apparently revealed by COVID-19 were in fact known well before its emergence. Our results suggest that absence of knowledge of the EID threat or an inability to convey that information to policymakers was not the cause of the United States' lack of preparedness. It is imperative to consider why congressional awareness did not translate into action sufficient to prevent the major disaster that COVID-19 became.
Footnotes
Acknowledgments
The authors wish to thank Jeffrey S. Schlegelmilch, Claire J. Standley, and Rebecca Katz for their kind review of drafts of the manuscript. Schmidt Futures provided a gift to Georgetown University (Grant #334) that funded both authors' work on this analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.