
Abstract
In fall 2020, COVID-19 infections accelerated across the United States. For many states, a surge in COVID-19 cases meant planning for the allocation of scarce resources. Crisis standards of care planning focuses on maintaining high-quality clinical care amid extreme operating conditions. One of the primary goals of crisis standards of care planning is to use all preventive measures available to avoid reaching crisis conditions and the complex triage decisionmaking involved therein. Strategies to stay out of crisis must respond to the actual experience of people on the frontlines, or the “ground truth,” to ensure efforts to increase critical care bed numbers and augment staff, equipment, supplies, and medications to provide an effective response to a public health emergency. Successful management of a surge event where healthcare needs exceed capacity requires coordinated strategies for scarce resource allocation. In this article, we examine the ground truth challenges encountered in response efforts during the fall surge of 2020 for 2 states—Nebraska and California—and the strategies each state used to enable healthcare facilities to stay out of crisis standards of care. Through these 2 cases, we identify key tools deployed to reduce surge and barriers to coordinated statewide support of the healthcare infrastructure. Finally, we offer considerations for operationalizing key tools to alleviate surge and recommendations for stronger statewide coordination in future public health emergencies.
Introduction
In fall 2020, COVID-19 infections accelerated across the United States. For many states, a surge in COVID-19 cases meant planning for the allocation of scarce resources and, subsequently, revisiting previously developed crisis standards of care (CSC) guidance or rapidly adapting CSC guidance from other states. 1 Conventional, contingency, and crisis phases of medical surge operations constitute a gradient of clinical context that dictate the standard of care available at a given time. 2 Under conventional care, healthcare staff use standard resources and provide the standard level of care through maximal use of the facilities' usual beds, staff, and resources. Under contingency care, healthcare staff provide functionally equivalent care, but care may be adapted from usual practices (eg, boarding critical care patients in postanesthesia care areas). Under crisis care, inadequate resources are available to provide equivalent care, and healthcare is provided to the highest level possible given the resource gap; increased risk of morbidity and mortality defines the care provided in this phase—this risk can be minimized by implementing consistent proactive resource use strategies. 3 A healthcare facility may move from conventional to crisis care in a week or a few hours. Moving into crisis operations and the equivalent standard of care has legal ramifications for healthcare providers and facilities, and clinical impacts for patients. Multiple studies document an increase in mortality for COVID-19 patients admitted to hospitals when facilities are above their standard patient capacity.4,5 CSC planning centers on guidance for decisionmaking in extreme operating conditions, which involve triage decisions. 2 While extensive guidance exists, 6 the approach to operationalizing CSC is not uniform, with wide variability in the existence and specificity of CSC guidance. 7
The US Constitution, administrative law, and other legal authorities in the United States endow individual states with legal powers to protect public health. Undergirding these legal duties are core ethical principles of public health, including public beneficence. Public beneficence, the duty of a government to act to maximize public benefit and minimize public harm, is the foundational moral commitment that serves public health. 8 Yet, federal and state guidance to forestall CSC in the healthcare infrastructure has been patchwork and does not systematically address the public health tools that can spare the healthcare system from extreme operating conditions. Moreover, the United States lacks comprehensive liability protections for public health emergencies, 9 which is a critical lever for ensuring protections for patients and healthcare workers.
One of the primary goals of CSC planning is to use all preventive measures available to avoid reaching crisis conditions. However, guidance on CSC centers on the context of adjudicating crisis conditions and ethically allocating scarce resources and focuses less on statewide and regional strategies to avoid them. Strategies to stay out of crisis conditions must respond to the actual experience of people on the frontlines, or the “ground truth” experience of healthcare providers. These strategies often include efforts to increase critical care bed numbers and augment staff, equipment, supplies, and medications to provide an effective response to a public health emergency.10,11 In addition, pandemic preparedness and response efforts that can forestall CSC must account for both public and private entities with the authority to facilitate coordination and bring all relevant stakeholders along to optimize efforts. 12 Successful management of a surge event where healthcare needs exceed capacity requires national support, planning, and coordinated strategies for scarce resource allocation. 13 Instead, over the COVID-19 pandemic, efforts to avoid CSC often fell to a small army of volunteers specialized in infectious disease preparedness and response leading through relationships in their organizations and states, rather than a care delivery network coordinated and supported nationally with the appropriate requirements.14,15 In this article, we provide an overview of the structural assumptions for avoiding crisis conditions—meaning the common clinical, legal, and public health actions taken to alleviate surge in the healthcare infrastructure. Next, we examine ground truth challenges encountered in response efforts during the fall 2020 surge in 2 states—Nebraska and California—and the CSC guidance and strategies each state used to enable healthcare facilities to stay out of CSC. Through these 2 cases, we identify key tools deployed to reduce surge and barriers to coordinated statewide support of the healthcare infrastructure. Finally, we offer considerations for operationalizing key tools to alleviate surge and recommendations for stronger statewide coordination in future public health emergencies.
Structural Assumptions for Avoiding Crisis Conditions
During the current pandemic, states and regions have demonstrated multiple complementary actions that help avoid crisis conditions in the healthcare infrastructure. Infectious disease and disaster health experts have assumed leadership roles to support population-level management of the emergency.
16
Strong, collaborative regional efforts are necessary for effective response and must be implemented regardless of any competitive posture between healthcare systems that may exist during usual operations. The following list, while not comprehensive, represents critical strategies and tools recommended to protect the healthcare infrastructure during a surge
17
:
Hospitals must share information, adjust protocols, and balance resources and patient loads across the immediate surrounding region to ensure standards of care are as consistent as possible.
17
To achieve necessary broad collaboration, healthcare institutions must incorporate emergency management principles of “mutual aid,” as outlined in the National Incident Management System Guideline for Mutual Aid, to effectively respond to a large-scale surge and provide a means for jurisdictions to augment their resources when needed for high demand incidents.
18
Effectively managing surge resources and load balancing—essentially the process of coordinating emergency response by sharing resources, transferring patients among hospitals, or both—are key for avoiding CSC.
19
Broad, public–private collaboration should involve a variety of healthcare systems, funding sources, jurisdictions, and payers to ensure effective allocation of scarce resources. Working together—with the support of state and/or local public health departments—hospitals can effectively and transparently form an efficient statewide system to respond to COVID-19. A clear, formal declaration for CSC at the hospital, hospital system, healthcare coalition, and jurisdictional levels is needed to provide consistency in care for the locality affected. This should include consistent clinical guidance about the scope of the declaration (ie, which resources or processes it applies to and which it does not). Intensive care units (ICU) are particularly vulnerable to strain from surge. ICU clinical leaders must have situational awareness (ie, being aware of what is happening around oneself) of staff, bed, and supply resources in absolute amounts and imminent availability to understand the responsible limits to which resources may be stretched during periods of critical clinical prioritization.20,21 Early transfer of patients before a hospital is overwhelmed promotes the effective conservation of resources and enables providers to offer optimal care standards. Transfer centers interface with all hospital and health systems in a region or state and typically may be engaged after routine referral sources are no longer accepting transfers. Their role is to facilitate and triage patient transfers quickly to an appropriate hospital setting including ICU and medical or surgical beds, while efficiently and effectively using capacity at both larger and smaller hospitals. Transfer centers have been an instrumental strategy in load balancing healthcare facilities close to or at crisis care level.
22
These centers provide a broadly impactful process for maintaining contingency care across entire regions and states; centers have ranged in their operations from statewide support for individual centers to massive regional off-loading of specific sites.
23
Successful transfer centers require regional and statewide commitment, coordination, and teamwork among healthcare systems, professional associations, and health departments. The goal of the transfer center is to ensure patients receive the appropriate level of care without delay, while load balancing other healthcare resources.
24
Alternate Care Sites (ACS) are often used as temporary sites that are intended to alleviate stress on the healthcare infrastructure by caring for low-acuity patients. ACS can be useful in providing hospital overflow, patient isolation, expanded ambulatory care, care for recovering noninfectious patients, limited supportive care for noncritical patients, primary triage, and rapid patient screening or quarantine.25-28
Simultaneous goals to drive COVID-19 into an outpatient disease entity managed by a multitude of primary care and outpatient clinicians can help mitigate surge and entry into CSC situations. Monoclonal antibody infusions were the first therapeutics to become available for outpatient use for patients with mild or moderate COVID-19 symptoms. Benefits of such treatments include improvement of patient outcomes and prevention of hospitalizations
29
; however, administration of these treatments can be challenging to operationalize due to the resources needed for infusion and the timing (ie, infusions must occur quickly after testing positive for COVID-19).
30
During the winter wave of 2020-2021, monoclonal antibodies were in limited supply—but implementation challenges proved more constraining. Again, during the Omicron wave, supply became an issue, as only 1 monoclonal antibody product retained effectiveness. As additional therapeutics have become available, options and complexity have increased. Unfortunately, as of February 2022, new oral antivirals remain limited in quantity, and the option of outpatient infusions of the antiviral drug remdesivir faces the challenge of 3 daily infusions as opposed to 1 for monoclonal antibodies.
31
As a result, most patients who qualify for outpatient therapeutics in the health system end up not receiving any. Future efforts should focus on enabling effective treatments for people with mild to moderate disease to reduce the burden on the healthcare system.
32
Preventing disease transmission within a locality is the first line of defense for the healthcare ecosystem. Often neglected in CSC planning, nonpharmaceutical interventions (NPI) are a critical tool for reducing community cases of communicable diseases and preventing the necessity for CSC in health emergencies. Some NPIs include quarantine and isolation, physical distancing, limits on travel and gathering, hand hygiene, and mask wearing. The impact of NPIs in reducing community transmission of COVID-19 is now well established.33-35
For NPIs to be effective in avoiding crisis conditions in healthcare, the role of triggers and legal mandates around NPIs should be specifically addressed. CSC planning should include setting triggers in hospital capacity and community disease burden that activate NPIs, which could effectively decrease disease transmission.
Successful management of a surge event where healthcare needs exceed capacity will require consistent use of these tools and strategies, and advanced planning and coordination at the local, state, regional, and federal levels. While this list represents activities protective of an overwhelmed healthcare infrastructure, federal- and state-level coordination of these activities is not required. Without federal requirements, there are no assurances that actions taken at the state and federal levels will support ongoing efforts to reduce the impacts of the emergency on the healthcare system infrastructure.
Two Case Studies
The approach to CSC planning to date does not reflect a uniform, national path but represents the extraordinary efforts of experts leading in their home states, often in the absence of political actors, public health agencies, and healthcare institutions. Over the course of 2020, Nebraska and California represent 2 distinct demographics faced with the realities of medical surge.
Nebraska
Nebraska has 2 major consolidated urban centers in the easternmost part of the state, with rural regions more characteristic throughout the rest of the state, all with differing population and hospital densities. With an area of 77,220 square miles and a population of over 1.9 million people, Nebraska is home to a range of private for-profit hospitals, public nonprofit hospitals, public for-profit hospitals, and critical access hospitals. Nebraska has over 31 general acute care hospitals with 63 critical access hospitals, more than 6,900 licensed hospital beds, and 232 licensed ICU beds. Nebraska has 20 local public health departments, and 427 licensed emergency medical services agencies.
Ground Truth Challenges
In fall 2020, Nebraska directly faced the challenge and difficulty of maintaining low case fatality ratios with a rising COVID-19 surge. Managing rising hospitalizations required broad collaboration among healthcare coalitions, healthcare facilities, emergency medical services, county emergency management agencies, long-term care and medical associations, state and local public health departments, and other state and federal agencies to be successful.
Nebraska was 1 of approximately 37 states without a CSC plan. While ventilator and personal protective equipment allocation dominated planning considerations early in the pandemic, stakeholders indicated that transport and staffing shortages were the primary resource allocation concerns during the surge. Clinicians were encountering severe strain that was not accounted for in existing CSC guidance, and where clinical judgment was needed to determine optimal use of available resources. 36 For instance, most state CSC guidance did not substantively address the needs of small and critical access hospitals or rural settings (eg, limited staffing prevents a CSC triage and oversight committee, greater need for regional support), which meant defining and agreeing on guidance in the middle of the pandemic. 6
Without state CSC guidance, Nebraska providers were in urgent need of legal protections for healthcare workers practicing in crisis situations. Hesitancy and inaction in planning, endorsing, or activating CSC created barriers for the healthcare and response community. By not providing codified guidance, the state left healthcare systems to shoulder extremely difficult planning and allocation decisions on their own. If individual hospitals or providers were not part of a larger healthcare system and could not benefit from ancillary support systems such as a legal department, they were left on their own in their decisionmaking. This vacuum of guidance also presented challenges for communication—limiting what people felt comfortable sharing and contributing to a culture of secrecy about the situations they were facing. Importantly, in the absence of clear guidance, frontline providers were left to make decisions about end of life and comfort care on their own, which impacts the consistency of care and may disproportionately impact disadvantaged populations in rural and frontier areas due to inequities in access to healthcare and/or due to inequities in comorbid condition prevalence and other effects of systemic racism. 7
Nebraska Crisis Care Guidance Development
In fall 2020, a small team from a multidisciplinary background of ethics, law, hospital clinical leadership, and emergency management was convened to work with the Public Health Fusion Cell to establish a CSC guidance document for the state of Nebraska. The surge team worked with over 40 healthcare providers across Nebraska to ensure it met the needs of all hospitals, rural and urban. Upon completion, the plan was endorsed by both the Nebraska Hospital Association and Nebraska Medical Association and was distributed to their members.
Legislation in most states provides the framework for CSC decisionmaking, including triggers for when to activate those standards. This legislation typically serves to establish a legal standard of care for the given state, which provides hospitals and other clinical providers with protection from liability. In Nebraska, no such legislation was in place during the fall 2020 surge, meaning that the team-developed CSC plan did not carry the same level of protection for providers as would exist under a state-backed plan. Through collaboration with state lawmakers and healthcare policy advocates, a bill was put before the Nebraska state legislature in early 2021 to establish and enact a Health Care Crisis Protocol for Nebraska, with the protocol being based on the team-developed CSC plan.37-40 The bill passed the legislature and was codified into law on May 25, 2021.
Key Strategies for Avoiding Crisis Conditions
The Nebraska Department of Health and Human Services launched the Nebraska Public Health Fusion Cell to improve public health coordination in Nebraska through interagency collaboration. In turn, the Public Health Fusion Cell endorsed the Regional Disaster Health Response System grant team request to create the Nebraska Medical Emergency Operations Center (MEOC) with the aim of coordinating medical surge response across the state and maintaining a low COVID-19 case fatality ratio of all Nebraskans (Figure 1). The MEOC tracks data across the state and at a local and healthcare coalition level for bed availability, patient transfers, COVID-19 hospitalizations, supply and equipment needs and resources. Throughout the COVID-19 pandemic, the MEOC has brought together statewide healthcare leadership and other key stakeholders to address healthcare-specific challenges. Integrated response centered on efforts to ensure the system put the right patient in the right bed at the right time. In addition, the MEOC served as a center for information sharing, rumor mitigation, and strategy development. The MEOC worked with critical access hospitals to facilitate infusions of monoclonal antibodies in long-term care and assisted living facilities. The MEOC worked directly with long-term care and assisted living facilities in the region and used existing relationships with a US Centers for Disease Control and Prevention Nebraska-based infection prevention grant group for phone technical assistance to establish a program to promptly distribute, prepare, and administer monoclonal antibody therapy to long-term care and assisted living residents in need, preventing COVID-19-related hospitalizations and deaths. 41 The state deployed a series of directed health measures (DHMs) to attempt to mitigate community spread of the disease (Box 1). Nebraska's DHMs remained in place throughout the fall and winter surge of 2020-2021 and were modified in stringency based upon community transmission rates and hospital capacity.
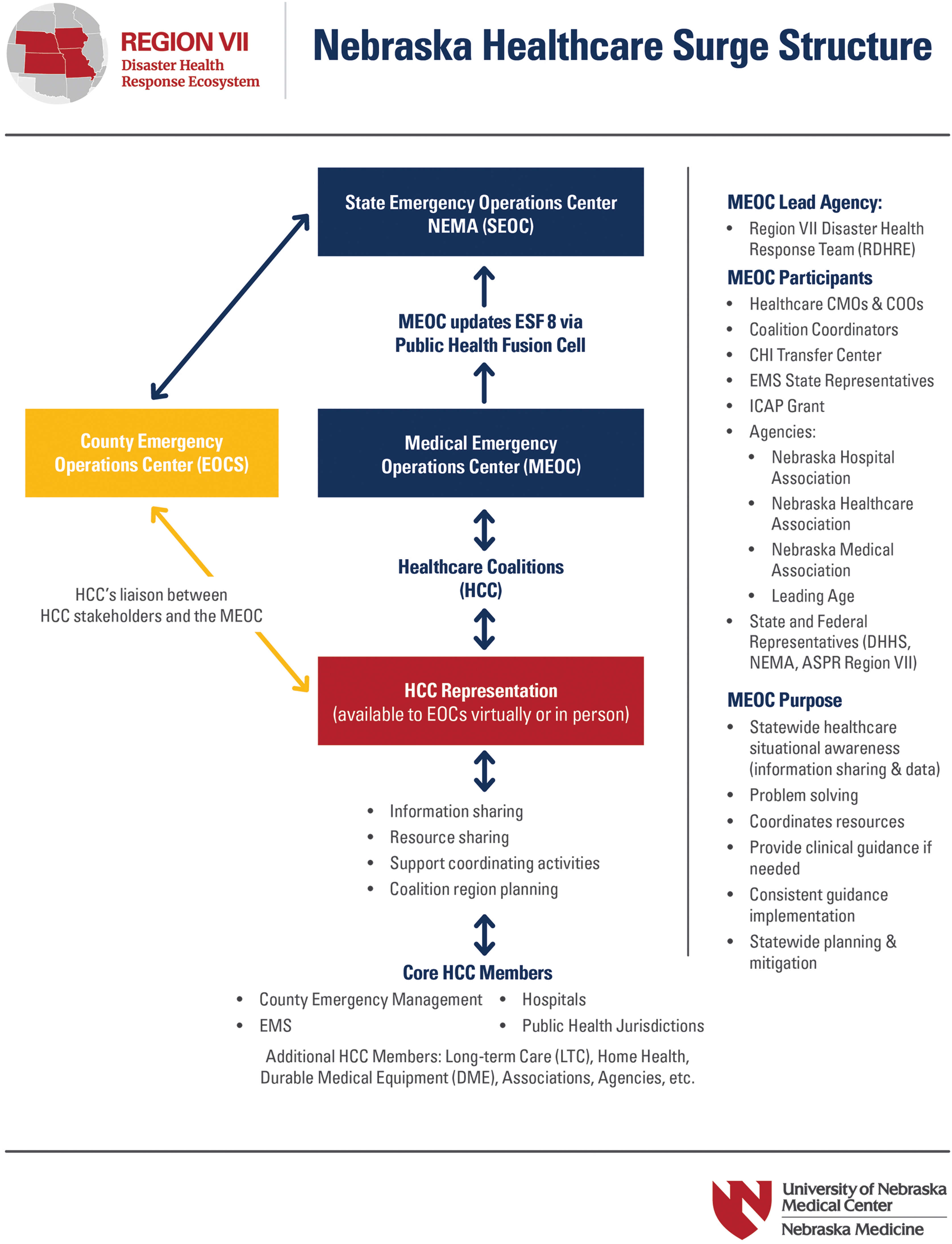
Nebraska Medical Emergency Operations Center had the aim of coordinating medical surge response across the state and maintaining a low COVID-19 case fatality ratio of all Nebraskans. Abbreviations: ASPR, Assistant Secretary for Preparedness and Response; CMO, chief medical officer; COO, chief operating officer; DHHS, Department of Health and Human Services; EMS, emergency medical services; ESF, emergency support function; HCC, healthcare coalitions; ICAP, Interventional Cooperative Agreement Program; MEOC, Medical Emergency Operations Center; NEMA, National Emergency Management Association.
Nebraska experienced many hospitalizations and deaths during surges in 2020 and 2021. In contrast to some of its Great Plains neighbors, Nebraska did not experience a crisis-level surge in its major hospital systems during that period and in large part was able to maintain conventional or contingency operations. The state allowed all DHMs to expire in late May 2021, as the Delta variant surge was building. Despite dramatically increased community case numbers and COVID-19 hospitalizations, only 1 DHM limiting elective surgeries has been reinstituted as of early September 2021. 42
Over the course of the surge, Nebraska identified and deployed key tools with the aim of avoiding crisis conditions: transfer center, CSC surge team, public health orders implementing NPIs, and tools for monitoring the pandemic (Box 1).
Nebraska Tools Deployed to Avoid Crisis Conditions
Abbreviations: CSC; crisis standards of care; DHM, directed health measures; MEOC, Medical Emergency Operations Center; NPI, nonpharmaceutical interventions; SOFA, sequential organ failure assessment.
California
California is home to approximately 40 million people spread across a total area of approximately 163,696 square miles. It is the most populous state in the United States, is the third largest state in terms of area, and has 2 of the top 5 most populated urban regions of the United States, the Los Angeles and San Francisco Bay areas. California has over 390 general acute care hospitals, more than 73,000 licensed hospital beds, and 11,500 licensed ICU beds, of which approximately 7,000 are adult beds, 750 are pediatric ICU beds, and 3,500 are neonatal ICU beds. California has 65 local public health departments, and 33 local emergency medical services agencies.
Ground Truth Challenges
At the 2020 winter peak of the pandemic, more than 21,900 COVID-19 patients were hospitalized (more than 36% of hospital census), and more than 4,800 COVID-19 patients were in the ICU (more than 60% of ICU census). ICU bed availability dipped to 8% statewide but was at or near 0% in many hospitals and counties. Due to its size and disaster risk (eg, earthquake, wildfires), California has a robust emergency management system. The state response to COVID-19 has been a collaboration between the California Office of Emergency Services, the California Health and Human Services Agency, and departments within the California Health and Human Services Agency, including the California Department of Public Health and the California Emergency Medical Services (EMS) Authority. The various state agencies worked in collaboration to address logistics and supply chain (California Office of Emergency Services), patient movement and transfers (California EMS Authority), hospital and skilled nursing facility staffing (California Department of Public Health), ACS, and more. The California EMS Authority includes a Disaster Medical Services Division, 43 which oversees multiple programs to respond to healthcare-related disasters including an Ambulance Strike Team, California Medical Assistance Teams, the Disaster Healthcare Volunteers registry, the Regional Disaster Medical Health Coordination Program, and the Medical Health Operational Area Coordinator Program. State documents defining large-scale medical response include the California Public Health and Medical Emergency Operations Manual, 44 and the California Patient Movement Plan. 45 Seven ACS spread strategically throughout the state provided care to over 1,900 patients and over 1,500 patients were transferred via the All-Access Transfer Center (Figure 2). ACS site selection was based on hospital utilization data and designed to provide support to the regions most impacted by COVID-19.

Alternate Care Sites and oxygen depots in California during surge. Abbreviation: ACS, Alternate Care Sites. Image created by Arzoo Salami, MD.
California engaged in a process to define crisis care guidelines for pandemics from 2008 through 2010; however, the project was shelved incomplete due to funding challenges. As many cities and regions witnessed crisis situations in Italy and New York during early 2020, local cities and hospital systems formulated crisis care plans in the absence of state and national guidance. In preparation for crisis, clinicians from various specialties and hospital systems initiated conversations that enabled a grassroots network for collaboration, which is foundational in averting crisis (Figure 3). For example, the city of San Diego had previously formed healthcare coalitions already in place in addition to disaster coordinators who met routinely from each hospital system; however, the city lacked clinical experts required to help anticipate regional needs and formulate crisis care plans for this novel and dynamic virus that causes patients to be hypoxemic and critically ill. By the time the state of California formulated plans, the region's healthcare system leadership had also formed a strong coalition and then partnered with San Diego County Public Health to implement crisis care plans at the hospital level. The early networking and education of clinicians regarding crisis care and triage helped build a bond of trust among bedside clinicians in the region. However, California, like Nebraska, was one of the states without complete crisis care standards supported by state legislation, a decision driven, in part, by political hesitancy and a lack of federal guidance.
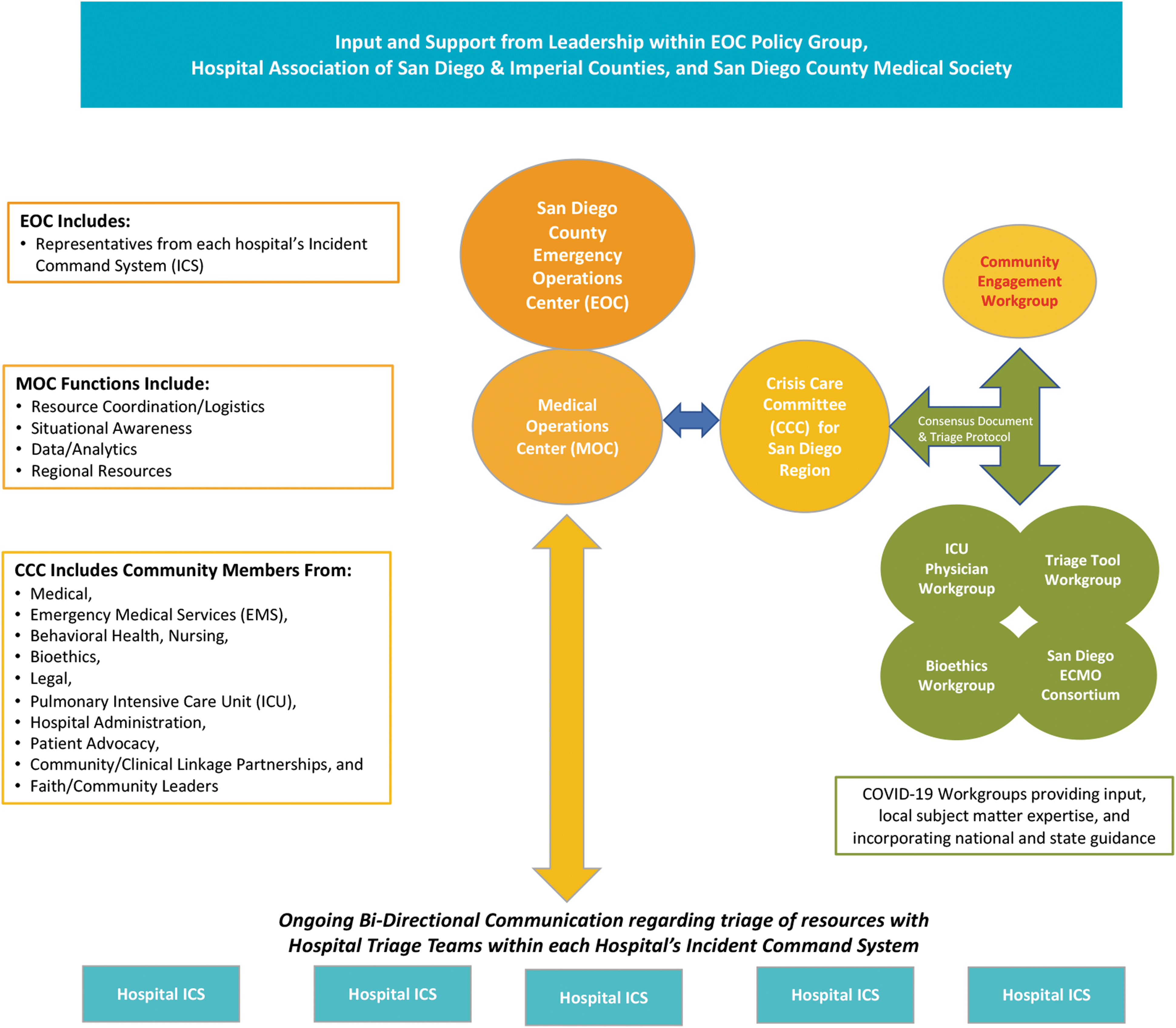
Example of healthcare coalition formation and groups formed to avert crisis care in San Diego, California. 13 Abbreviations: CCC, Crisis Care Committee; ECMO, extracorporeal membrane oxygenation; EOC, Emergency Operations Center; ICS, incident command system; ICU, intensive care unit; MOC, Medical Operations Center.
California Crisis Care Guidance Development
Beginning in April 2020, the California Department of Public Health convened a state team to draft CSC guidelines using the original 2008 state work, current literature on the topic, review of multiple guidelines from other states, and review of existing California Health Systems documents addressing crisis care (eg, San Diego, University of California Health, Kaiser Permanente, Stanford University). The California Department of Public Health also identified a Crisis Care Advisory committee of 11 individuals from throughout the state and included representation from various advocacy groups. After publication of the initial guidelines, meetings were held for feedback from multiple stakeholder and advocacy groups. 46 The feedback resulted in revisions to the guidelines, with publication of the final version in June 2020. 47
Given the time-sensitive nature to issue guidelines facing the impending COVID-19 surge, the process faced numerous challenges, including difficulty in messaging to the entire health system in California, and sufficient time for feedback from the wide array of relevant stakeholders. The advisory committee was instrumental in providing diverse expertise and input to finalize guidelines. Several conference calls were held to engage hospital leaders throughout the state for review of the crisis care guidelines and to encourage adoption into existing facility emergency operations plans. Unlike sudden onset and unannounced disasters (eg, earthquake, terrorism), pandemics are slower in onset and longer in duration. The slower onset affords healthcare the benefit of advanced planning, and the execution of a tiered surge response appropriate for the level of surge. A critical feature of the California pandemic guidelines is the following requirement: before reaching the highest level of surge response necessitating the allocation of lifesaving scarce resources, any health facility must first ensure they have engaged with all local, regional, and state partners for mutual aid assistance, resource requests for supply and staffing procurement, and intrafacility transfers for load balancing of patients. This feature firmly places the focus of crisis care on averting the need to allocate lifesaving resources to some but not others.
Key Strategies for Avoiding Crisis Conditions
Based upon rising cases and modeling data on ICU peak capacity, medical societies, such as the California Thoracic Society, instituted weekly calls for critical care clinicians, respiratory therapists, public health, and industry to connect and collaborate regarding near crisis situations. Problems were solved in real time with brief clinical updates regarding evolving science discussed by experts within the state to maintain common standards of care. The medical society also facilitated connections among state experts in extracorporeal membrane oxygenation (ECMO) and invited ethicists to help define and discuss CSC. Clinicians throughout the state from community hospitals to large academic institutions connected and enabled frontline concerns to be addressed. Building and strengthening connections within the medical field proved to be an important foundation in alleviating the burden of CSC in the event of formal declaration.
Over 1,900 patients were successfully managed by California Medical Assistance Teams, California EMS Authority, and contracted healthcare workers at ACS throughout California (Figure 3). Running hospital-level care with oxygen, therapeutics, and complex medical needs for COVID-19 patients was challenging. Limitations in healthcare workforce staffing, supplies, oxygen, and space resulted in near crisis situations in many hospital systems. The ACS and creation of oxygen depots provided necessary support and relief. 48 The ACS also served to help with vaccination and monoclonal antibody administration to alleviate burdens on hospitals. California found that the most cost-effective effort was to assist hospitals directly with expansion of alternate care spaces connected operationally to existing hospitals due to logistics and staff training needs.
Even when maximizing the health system's ability to manage surge using the strategies previously noted, widespread disease transmission during a pandemic can still overwhelm the capacity of a surged health system. Because of this, another essential element to avoiding crisis care resides in the ability of public health to impose NPIs that have substantial impact on disease transmission. 33 At various times during the pandemic, California Public Health used various mandates to decrease COVID-19 transmission, including mask mandates, nonessential business sector closure, curfews, and ultimately a statewide stay-at-home order in mid-December. Tracking of cases and hospitalizations in relation to NPIs confirm that these NPIs had a measurable effect in blunting disease transmission, surging cases, and resulting hospitalizations.
California identified and deployed key tools with the aim of avoiding crisis conditions: patient movement for load balancing, California multiagency COVID-19 surge teams, executive and public health orders, and tools for monitoring the pandemic (Box 2).
California Tools Deployed to Avoid Crisis Conditions
Abbreviations: ASPR, Office of the Assistant Secretary for Preparedness and Response; CDPH, California Department of Public Health; EMSA, Emergency Medical Service Authority; EMT, emergency medical technician; HHS, US Department of Health and Human Services; ICU, intensive care unit; OES, Office of Emergency Services; PH, public health; PPE, personal protective equipment.
Operational Considerations and Recommendations
Public health emergencies and pandemics require strong public health leadership with collaboration from the private sector and the local, state, and federal government. No single organization can weather a response at the scale of COVID-19 on their own. 49 With the examples drawn from California and Nebraska, we offer operational considerations and recommendations for more comprehensive CSC planning moving forward (Table 1).
Patient Movement During the COVID-19 Pandemic in California Included 3 Distinct Complementary Processes
Abbreviations: AATC, All-Access Transfer Center; EMSA, Emergency Medical Services Authority; IFT, intrafacility transfer; MHOAC, Medical Health Operational Area Coordinator; RDMHC, Regional Disaster Medical Health Coordinator.
Operational Considerations for Public Health Tools
Tools to avoid CSC include advanced planning; identification of triggers for early intervention; robust use of mutual aid for expanding space, stuff, system, and staff; transfer considerations for patient load balancing; utilization of modeling and forecasting to trigger NPIs with healthcare capacity in mind; and emergency orders. Throughout the case studies, we discussed how these tools were leveraged in California and Nebraska; in Table 2, we outline some of the key considerations that supported optimizing resources and operational considerations. While the tools outlined in the figure are critical to alleviating surge, more is needed at the federal and state level to require efforts that can spare the healthcare system from crisis conditions.
Tools to Avoid Crisis Standards of Care
Abbreviations: ACS, Alternate Care Sites; CSC, crisis standards of care; IFT, intrafacility transfer; MEOC, Medical Emergency Operations Center; NPI, nonpharmaceutical interventions.
Recommendations for Stronger Statewide Coordination of Care in Public Health Emergencies
1. Consistent deployment of public health tools directly to alleviate surge in the healthcare infrastructure
State leadership (ie, public health, governors, attorneys general, regulatory entities) should identify ways in which mitigation and surge strategies can be implemented. 50 As stewards of their state's resources and chief executive officers of their states, governors are in a unique position to ensure that the basic needs of their populace are being met in a disaster. By failing to provide leadership or to create an atmosphere that is inclusive of CSC planning, governors run the risk of not protecting their citizenry in an emergency and exacerbating the potential impacts of that emergency in their state.
To achieve effective coordination of surge, the federal government should provide coordinated leadership of CSC guidelines, but importantly, more work is needed to ensure the public health tools (eg, monitoring tools, transfer centers, public health orders, CSC Surge Teams) necessary to prevent crisis are deployed at the state and local levels to ensure there is equity, balance, and consistency across US planning. 2 In California, after instituting mandatory masking and multiple nonessential sector closures (eg, restaurants, bars) hospitalizations continued to surge. California used a trigger of less than 15% ICU bed availability to enact a stay-at-home-order in efforts to decrease case rates. NPI efforts were effective and deferred the peak by 3 weeks; even with the stay-at-home order, the state dropped to 8% ICU availability before hospitalizations began to drop. Whereas in Nebraska, as the Delta surge accounts for continued increase in hospitalization, the state has only 1 DHM (ie, limiting elective surgeries) in place, a decision made without any modeling to support effective protection. From early July to late August 2021, Nebraska saw a 10-fold increase in COVID-19 ICU hospitalizations—hitting 40% of total ICU availability for the state. 51 Even with the rapid increase in COVID-19 hospitalizations, Omaha, Nebraska, did not implement masking requirements to slow community transmission. Without a citywide mask mandate in the fall of 2021, public schools and superintendents were left to decide whether to require masks as students returned to school; a decision that was complicated for school districts due to the governors clear stance to keep masks optional in schools.52,53
2. Improve state leadership on surge strategies and crisis standards of care guidance
Although many states experienced crisis conditions in 2020, 54 Arizona and New Mexico were the only states to formally declare CSC. 55 Often, state officials are hesitant to activate CSC. 56 In Nebraska, even with a codified law, political leaders were hesitant to enumerate their role in activating CSC, instead shifting those decisions to facilities. Declaring CSC at the state level acknowledges the reality of the situation and can have negative implications spanning from managing messaging about CSC (eg, the faulty notion that it is akin to death panels) to critiques of failed leadership (eg, that state officials did not do enough to prevent the situation) to practical concerns (eg, scope, authority, liability, issues on what shortages rise to a declaration of crisis) 50 ; however, failure to acknowledge the reality of a situation does not invalidate the experiences of providers and patients. The private sector faced the financial realities while making decisions to mitigate surge, as caring for critically ill patients is often a threat to the typical business case for health systems. While state leadership will continue to play a role in surge strategies and CSC guidance, more study is needed to understand what future efforts are effective, and how to best incorporate public and private partnerships into future planning.
3. Create requirements for consensus-driven and evidence-based crisis standards of care guidance
Currently, the United States lacks a central, consensus-driven CSC protocol at the federal level and at the medical society level. In both Nebraska and California, the states were left to determine the appropriate guidance, but providers and facilities had to shoulder the responsibility and accountability for oversight often with little state-backed support. Federal oversight for CSC could provide accountability for policy choices at the state and local levels. 57 The Centers for Medicare and Medicaid Services have demonstrated the ability to innovate approaches to ensure lifesaving healthcare delivery in other areas, and this approach should be applied to readiness in the future. 58 The Centers for Medicare and Medicaid Services, in partnership with state governors and their regulatory authorities, can compel health insurers to participate in partnerships to develop a better business case for health systems to be ready for future outbreaks.
Conclusion
The continued COVID-19 surge sweeping US healthcare facilities in the winter of 2021 only underscores the need to strengthen our governing structures, promote public and private partnerships, and encourage state and federal leaders to use every available strategy and tool to ensure the health and safety of the US population.