
Abstract
In the context of the COVID-19 pandemic, reassessing intensive care unit (ICU) use by population should be a priority for hospitals planning for critical care resource allocation. In our study, we reviewed the impact of COVID-19 on a community hospital serving an urban region, comparing the sociodemographic distribution of ICU admissions before and during the pandemic. We executed a time-sensitive analysis to see if COVID-19 ICU admissions reflect the regional sociodemographic populations and ICU admission trends before the pandemic. Sociodemographic variables included sex, race, ethnicity, and age of adult patients (ages 18 years and older) admitted to the hospital's medical and cardiac ICUs, which were converted to COVID-19 ICUs. The time period selected was 18 months, which was then dichotomized into pre-COVID-19 admissions (December 1, 2018 to March 13, 2020) and COVID-19 ICU admissions (March 14 to May 31, 2020). Variables were compared using Fisher's exact tests and Wilcoxon tests when appropriate. During the 18-month period, 1,861 patients were admitted to the aforementioned ICUs. The mean age of the patients was 62.75 (SD 15.57), with the majority of these patients being male (52.23%), White (64.43%), and non-Hispanic/Latinx (95.75%). Differences were found in racial and ethnic distribution comparing pre-COVID-19 admissions to COVID-19 admissions. Compared with pre-COVID-19 ICU admissions, we found an increase in African American versus White admissions (P = .01) and an increase in Hispanic/Latinx versus non-Hispanic/Latinx admissions (P < .01), during the COVID-19 pandemic. During the first 3 months of admissions to COVID-19 ICUs, the number of admissions among Hispanic/Latinx and African American patients increased while the number of admissions among non-Hispanic/Latinx and White patient decreased, compared with the pre-COVID-19 period. These findings support development of strategies to enhance allocation of resources to bolster novel, equitable strategies to mitigate the incidence of COVID-19 in urban populations.
Introduction
Optimizing the use of intensive care units (ICUs) is an important healthcare priority in the United States, 1 which requires a critical understanding of variables that contribute to regional usage of adult ICUs. For instance, geographic and sociodemographic factors (eg, prevalence of ethnic and racial populations, poverty, education status)2,3 and the presence of certain medical conditions4,5 are associated with adult ICU utilization and admissions.5,6 When assessing common diagnoses, such as sepsis and acute respiratory distress syndrome, present on admission to adult medical ICUs, these diagnoses cluster in regions with high prevalence of certain medical conditions (eg, hypertension and diabetes) 7 and with socioeconomic factors (eg, race, ethnicity, poverty).5,8 Insight into the aforementioned variables would ensure efficient use of critical care resources for hospitals, communities, and patients.
The current pandemic caused by SARS-CoV-2 has created unprecedented demands on acute healthcare, necessitating the development of triage algorithms typically assigned to battlefields to determine who receives medical treatment or access to medical equipment, and in which order. 9 Specifically, COVID-19 frequently results in sepsis and acute respiratory distress syndrome,10,11 which warrant ICU admissions. Having reached a point several months into the pandemic, reassessing ICU utilization, specifically regional impact, should be a priority for hospitals in an effort to assist in ongoing public health policies to mitigate the spread of the virus and plan for critical care resource allocation.
In our study, we reviewed the impact of COVID-19 on a community hospital serving an urban region. Specifically, we conducted a time-sensitive analysis to determine whether ICU admissions during the COVID-19 pandemic reflect ICU admission trends before the pandemic in regard to regional and sociodemographic characteristics.
Methods
Patient Population
We obtained data on admissions to 2 ICUs—the medical ICU and the cardiac ICU—at Johns Hopkins Bayview Medical Center over a period of 18 months (December 1, 2018 to May 31, 2020). The medical center is 1 of 3 academic hospitals within the Johns Hopkins Health System, located in Baltimore, Maryland, and has a potential capacity of 500 beds. The reason for choosing the medical and cardiac ICUs is that both were converted to specialized COVID-19 ICUs to provide care for critically ill patients confirmed or suspected of having COVID-19. We reviewed the records of all adult patients (aged 18 years or older) admitted to the ICUs during this period. The study was approved by the Institutional Review Board at Johns Hopkins School of Medicine and all actions undertaken by the authors were in accordance with the Declaration of Helsinki.
The Johns Hopkins Bayview Medical Center serves diverse populations within the hospital's proximity (zip codes: 21202, 21205, 21206, 21213, 21218, 21219, 21222, 21224, 21231). The 3 primary populations within this region are African American (12.4% to 27.5%), and Hispanic/Latinx (17.1% to 31.9%), and White (55.2% to 80.1%). 12 The median household income ranges from $32,102 to $71,660, and the family poverty rate ranges from 15.2% to 43.6%. 12
Study Period
The study period occurred over 18 months (December 1, 2018 to May 31, 2020), which provided an entire fiscal year of ICU admissions, allowing secular trends to be identified in how specific populations used critical care resources during a specific period. In addition, by capturing the first 3 months (mid-March to May 2020) of COVID-19 ICU admissions, we could assure that trends observed during this period were (1) not specific to the current year and (2) not typical seasonal trends (as our data also captured March to May 2019).
The data were then divided into pre-COVID-19 ICU admissions (December 1, 2018 to March 13, 2020) and COVID-19 ICU admissions (March 14, 2020 to May 31, 2020). We chose March 14, 2020, as the beginning of the COVID-19 period because the first case of COVID-19 was reported in Baltimore on that date 13 and this timeframe correlated with an increase in COVID-19 admissions in our hospital.
Variables of Interest
We collected individual sociodemographic data including age, sex, race, ethnicity, and preferred language spoken (identified as “English not preferred”) of all patients admitted to the medical ICU and the cardiac ICU during this period. We defined older adults as individuals 65 years or older. We also documented the length of stay in the ICU and ICU mortality.
Statistical Analysis
All continuous variables are presented as a mean with standard deviation (SD) or median (interquartile range [IQR]). Categorical variables were summarized as counts and percentages. Variables were compared using Fisher exact tests and Wilcoxon signed-rank tests when appropriate. For comparisons of more than 2 groups, an analysis of variance was performed. We used conditional density plots to display population admissions over the 18-month period. Statistical analyses were conducted with RStudio version 0.99.903 (R Foundation, Vienna, Austria).
Results
Over the course of 18 months, the medical and cardiac ICUs saw a total of 1,861 admissions. The mean age of the 1,861 patients was 62.75 years (SD 15.57, IQR 19 to 100). The majority of these patients were male (52.23%), White (64.43%), and non-Hispanic/Latinx (95.75%). Of the 1,861 patients, 419 (22.51%) died. A complete list of sociodemographic and hospital variables is provided in Table 1.
Demographic Data of the Patient Population, December 2018 to May 2020 (N = 1,861)
Note: Pre-COVID-19 admissions occurred from December 1, 2018 to March 13, 2020, and COVID-19 admissions occurred from March 14 to May 31, 2020.
Abbreviations: ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
Of the 1,861 patients, 210 were admitted between March 14 and May 31, 2020, during the COVID-19 pandemic. No statistically significant differences were found in age (P = .18), ICU length of stay (P = .95), or death (P = .46) between pre-COVID-19 and COVID-19 ICU admissions. However, our findings showed significant statistical differences in racial and ethnic distribution. Compared with pre-COVID-19 admissions, COVID-19 admissions saw a significant increase in African American patients compared with White patients (P = .01), and a significant increase in Hispanic/Latinx patients compared with non-Hispanic/Latinx patients (P < .01). Table 1 further dichotomizes sociodemographic variables by pre-COVID-19 and COVID-19 admissions.
Hispanic/Latinx Patients
Among Hispanic/Latinx patients, 35.44% of admissions during the 18-month period occurred between mid-March and May 2020 (Figure 1). By May 2020, Hispanic/Latinx patients represented 13.3% (n = 28 ) of 210 COVID-19 ICU admissions. By contrast, during the pre-COVID-19 period, Hispanic/Latinx patients represented 3.1% on average, ranging from 2.34% to 5.27% of monthly ICU admissions. However, there was no difference in mean age between Hispanic/Latinx ICU patients admitted before (mean 48.46, SD 13.07) and during (mean 49.67, SD 19.50) (P = .75) COVID-19. No differences were found in Hispanic/Latinx male patient admissions either, as they continued to represent the majority sex admitted to the ICU: 34 patients (66.67%) pre-COVID-19 and 21 patients (75.00%) during COVID-19 (P = .61). There was also no difference in ICU length of stay (P = .14) and no difference in mortality (4 deaths among Hispanic/Latinx patients before COVID-19 compared with 1 death during COVID-19) (P = .79).
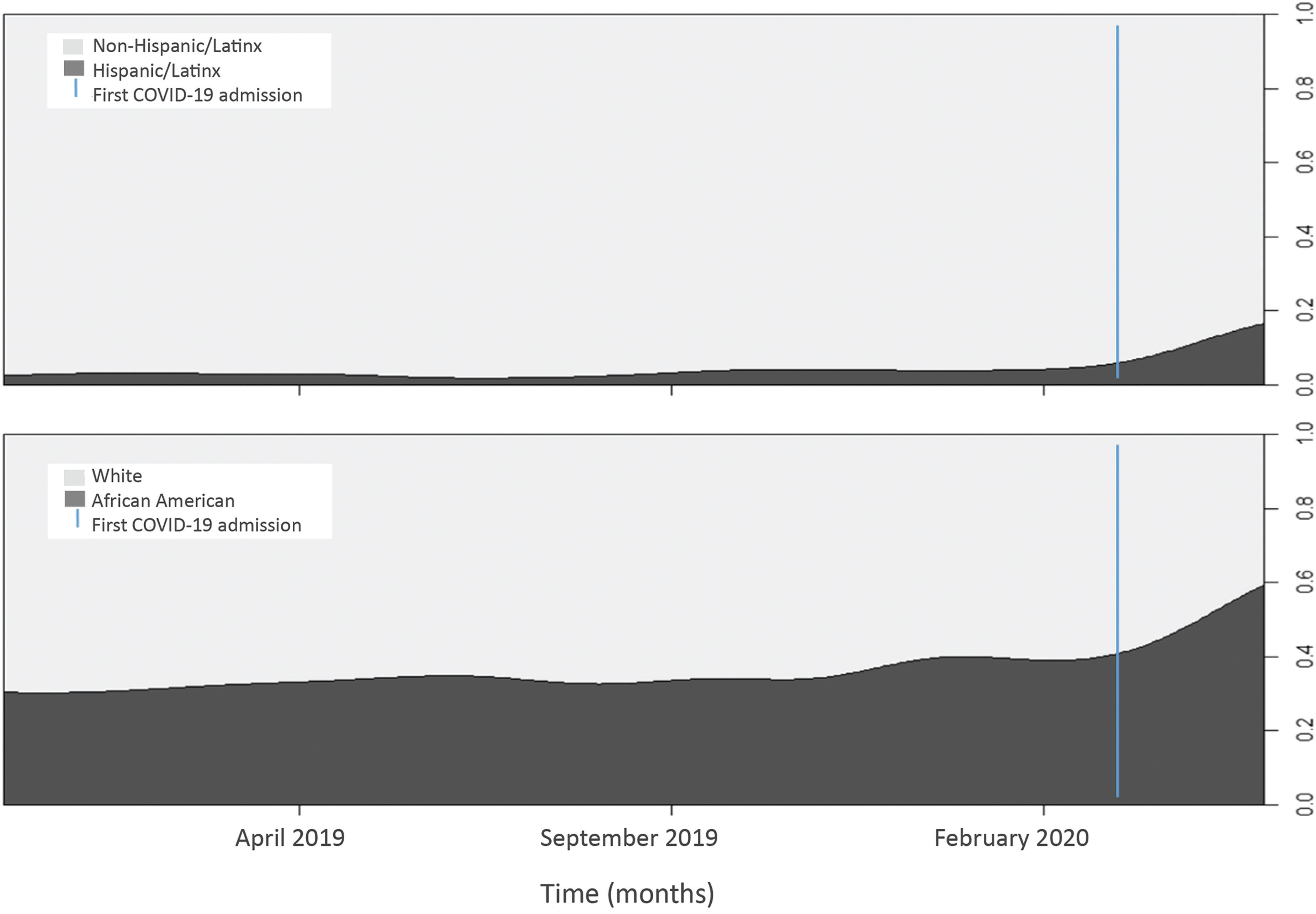
Comparison of intensive care unit admissions by population before and during the COVID-19 pandemic. The blue line represents March 14, 2020, the date that divides the pre-COVID-19 and COVID-19 periods.
During COVID-19, Hispanic/Latinx ICU admission patients were younger (mean 48.46, SD 13.07) than non-Hispanic/Latinx patients (mean 63.25, SD 16.29) (P < .01) and predominantly male (P = .04). However, deaths occurred at a higher rate among non-Hispanic/Latinx patients (28.02%) than Hispanic/Latinx patients (3.57%) (P = .01). Table 2 further emphasizes differences between race and ethnicity outcomes.
Intensive Care Unit Admissions by Ethnicity and Race During the COVID-19 Pandemic
Note: COVID-19 admissions occurred from March 14 to May 31, 2020.
Abbreviation: ICU, intensive care unit; IQR, interquartile range; SD, standard deviation.
African American Patients
Among African American patients, 13.5% of admissions during the 18-month study period occurred between mid-March and May 2020 during the COVID-19 pandemic (Figure 1). By May 2020, African American patients accounted for 35.20% (n = 74) of the 210 total COVID-19 ICU admissions. In contrast, African American patients represented 28.65% of ICU admissions before COVID-19. No statistically significant differences in age were found between African American patients admitted before (mean 58.96, SD 15.91) and during COVID-19 (mean 57.95, SD 16.63) (P = .56). There was a statistically significant difference in ICU length of stay, however. Before COVID-19, the median ICU length of stay was 3 days (IQR 1.00 to 6.00), whereas during COVID-19 it was 4 days (IQR 1.25 to 7.75) (P = .04). Further, a significant difference was found in mortality among African American ICU admissions before COVID-19 (n = 88, 23.98% of 367 total deaths) and during COVID-19 (n = 23, 44.20% of 52 total deaths) (P = .04).
Among ICU admissions during the COVID-19 pandemic, the mean age of African American patients was lower (57.95, SD 16.63) than the mean age of White patients (64.95, SD 15.96) (P < .01). Further, African American patients had longer ICU stays than White patients (P = .02). No difference in mortality was found during the same period.
Older Adults
Among adults aged 65 years or older, 12.4% of admissions during the 18-month period occurred between mid-March to May 2020. No statistically significant difference in age was found between older adults admitted before COVID-19 (mean 75.42, SD 8.46) and during COVID-19 (mean 75.60, SD 8.60) (P = .84), and no significant difference in sex was found (P = .25). White older adult patients accounted for 71.71% (n = 573) of 799 total older adult patients before COVID-19, and 68.9% (n = 51) of 74 total older adult patients during COVID-19 (P = .0495). Finally, there was a nonstatistically significant increase in mortality among older adult ICU patients admitted during COVID-19 (n = 37, 37.37%) than before COVID-19 (n = 228, 28.53%) (P = .82). When evaluating older adults by race, there was a statistically significant increase in mortality among African American patients from before COVID-19 (n = 113, 14.1% of 799) to during COVID-19 (n = 23, 31.08% of 74) (P = .02). There were no deaths among older adult Hispanic/Latinx patients (n = 6) during COVID-19 ICU admissions.
Discussion
During the first 3 months (mid-March to May 2020) of admissions to COVID-19 ICUs at Johns Hopkins Bayview Medical Center—an urban, academic, community hospital—the number of admissions among Hispanic/Latinx and African American patients increased while the number of admissions among non-Hispanic/Latinx and White patients decreased, compared with the pre-COVID-19 period. Hispanic/Latinx patients admitted to the COVID-19 ICU were younger than non-Hispanic/Latinx patients. As expected, given the age differential, Hispanic/Latinx patients had greater survival rates compared with non-Hispanic/Latinx patients. African American ICU patients had worse mortality outcomes during COVID-19 than before, especially among older African American patients ages 65 or older. Overall, this shift in both admissions and outcomes based on race and ethnicity was significant during the COVID-19 pandemic for this community hospital compared with the previous year's ICU admissions.
Disparities in critical care diagnoses and admissions have been well documented.5,6,14 And in the case of the COVID-19 pandemic, disparities continue to exist in the proportion of racial and ethnic populations impacted by COVID-19. 15 In the analysis by Price-Haywood et al, the authors found a disproportionate impact on African Americans with COVID-19—76.9% of the patients hospitalized and 70.6% of the patients who died were African American. 16 The data reviewed spanned the first 6 weeks of the public health crisis of COVID-19 in Louisiana (March 1 to April 11, 2020). Such a disproportionate impact was also seen in African American patients in our hospital's admissions. However, our data showcases that the pandemic had differential effects, increasing the number of African American ICU patients admitted while simultaneously decreasing the admissions of White patients. This finding is new, as evident by our review of critical care admissions from December 1, 2018 to March 13, 2020 which were consistently stable for both African American and White patients, as well as for Hispanic/Latinx versus non-Hispanic/Latinx patients.
Optimizing regional ICU utilization has been a priority during the COVID-19 pandemic. 17 Using time-lapsed, sociodemographic data from ICU admissions may help identify communities disproportionately impacted by COVID-19 and inform strategies to attenuate such disparities. Such investigations into ICU admissions would parallel other interventions and may result in community efforts to mitigate these severe diseases. For instance, Victor et al 18 demonstrated a community intervention to improve blood pressure control among non-Hispanic/Latinx African American men by partnering with barbershops in Los Angeles; such an effort is warranted as this population has the highest rate of hypertension-related critical care admissions. 19 ICU-level information reaffirms the need to promote testing and identify resources to facilitate isolation and quarantine for African American16,20,21 and Hispanic/Latinx20-22 individuals who are experiencing COVID-19-related health disparities. Social and community responses are needed due to the important and active role that communities can play in preventing disease and promoting health, especially given the social transmission pathways of COVID-19. 23 Such collaborative strategies will require active community engagement and partnerships with neighborhood leaders to leverage community-based resources and venues, in addition to structural changes at policy and advocacy levels.
This study has several limitations. First, we did not evaluate more granular clinical data, such as severity of symptoms on presentation and preexisting conditions. Second, we did not investigate which COVID-19–related syndromes warranted ICU admissions (eg, sepsis, acute respiratory distress syndrome, heart failure). While these limitations are important to address in future studies and are necessary overall to understand the complete clinical presentation of COVID-19, we believe such information was not as relevant for implementing immediate community engagement initiatives among populations impacted disproportionately by the pandemic. Finally, this information is relevant for our community hospital based in an urban area; it is unclear if similar findings would occur in community hospitals serving rural areas. This should be investigated to understand urban versus rural differences in populations as related to COVID-19 incidence and ICU admissions.
Conclusion
In the first months of the pandemic, a significant sociodemographic shift occurred in regard to patients admitted to the Johns Hopkins Bayview Medical Center, an urban community hospital ICU. At the same time ICU admissions for non-Hispanic/Latinx and White patients decreased, ICU admissions for Hispanic/Latinx and African patients increased. While much has been said regarding the disproportionate impact of the COVID-19 pandemic on racial and ethnic urban populations, we have shown, using time-lapse evaluations, that pre-pandemic/pandemic ICU trends for specific populations at our hospital were indeed significantly different. As strategies are discussed to curb the incidence of COVID-19 among specific patient populations, monitoring whether such a reduction results in a decrease in ICU admissions should be emphasized as a public health priority.