
Abstract
Vulnerable refugee communities are disproportionately affected by the ongoing COVID-19 pandemic; existing longstanding health inequity in these communities is exacerbated by ineffective risk communication practices about COVID-19. Culturally and linguistically appropriate health communication following health literacy guidelines is needed to dispel cultural myths, social stigma, misinformation, and disinformation. For refugee communities, the physical, mental, and social-related consequences of displacement further complicate understanding of risk communication practices grounded in a Western cultural ethos. We present a case study of Clarkston, Georgia, the “most diverse square mile in America,” where half the population is foreign born and majority refugee. Supporting marginalized communities in times of risk will require a multipronged, systemic approach to health communication including: (1) creating a task force of local leaders and community members to deal with emergent issues; (2) expanding English-language education and support for refugees; (3) including refugee perspectives on risk, health, and wellness into risk communication messaging; (4) improving cultural competence and health literacy training for community leaders and healthcare providers; and (5) supporting community health workers. Finally, better prepared public health programs, including partnerships with trusted community organizations and leadership, can ensure that appropriate and supportive risk communication and health education and promotion are in place long before the next emergency.
Background
Low levels of literacy and health literacy combined with language and cultural differences are common challenges to delivering health information in vulnerable refugee, immigrant, and migrant communities; however, COVID-19 presented an unprecedented challenge requiring immediate and urgent risk communication. The need to reach refugee, immigrant, and migrant community members rapidly to curb a potential acute outbreak of COVID-19 was paramount. In general, these community members live in high-density housing; work frontline jobs in manufacturing, healthcare, and food processing; are under- or uninsured; and lack access to healthcare providers for both culturally and linguistically concordant information and care. Communicating real-time guidance during a crisis increases informed decision making for refugees and their families. The task of delivering those messages to people who come from diverse countries, cultures, and languages is daunting, 1 and may be nearly impossible if the message is framed only in Western perspective, ethos, and language.2,3 If an overarching public health goal is to improve the health and quality of life for all cultures and life stages, providing health information that is culturally and linguistically appropriate is critical.1-3 Culture creates a framework that informs one's perspectives on risk, levels of danger, disease, treatment, health, and wellness; cultural perspectives align with myths, stigma, family values, and community values, all of which may vary from person to person and culture to culture.2,3 Different cultural perspectives also affect how individuals receive and process information; for many cultures, storytelling, educational entertainment, and communicating the value of community are the most appropriate messaging methodologies, and may be in direct conflict with general broad messaging campaigns.4,5 While foundational elements of risk communication require tailoring messages to specific audiences and using plain language, actual implementation of risk communication often fails to meet the needs of vulnerable, marginalized, multicultural communities.6-8
The Most Diverse Square Mile in America
Clarkston, Georgia, is a diverse ethnic community on the outskirts of downtown Atlanta where more than 17,000 refugees have initially settled since 2004. It has been referred to as the “Ellis Island of the South” and “the most diverse square mile in the United States.” 9 Currently, half of Clarkston's residents are foreign-born refugees, creating a community where more than 60 languages are spoken. They come from regions of the world—such as Democratic Republic of the Congo, Nepal, Syria, Burma, Iraq, and Somalia—where war, ethnic conflict, drought, and environmental degradation have spurred the flight of millions from their home country. Based on the Social Vulnerability Index 10 —a measure of potential community damage based on social determinants of health such as poverty, crowded housing, lack of transportation, and employment status (Figure 1)—Clarkston is subject to all of these adverse conditions. For the period of 2014 to 2018, the 8 census tracts that make up Clarkston had an average Social Vulnerability Index of 0.9741 with a range of 0.9309 to 0.9995 (values close to 1 indicate greater vulnerability). 10 The larger county area in which Clarkston resides had an index of 0.6892 during the same period. 10
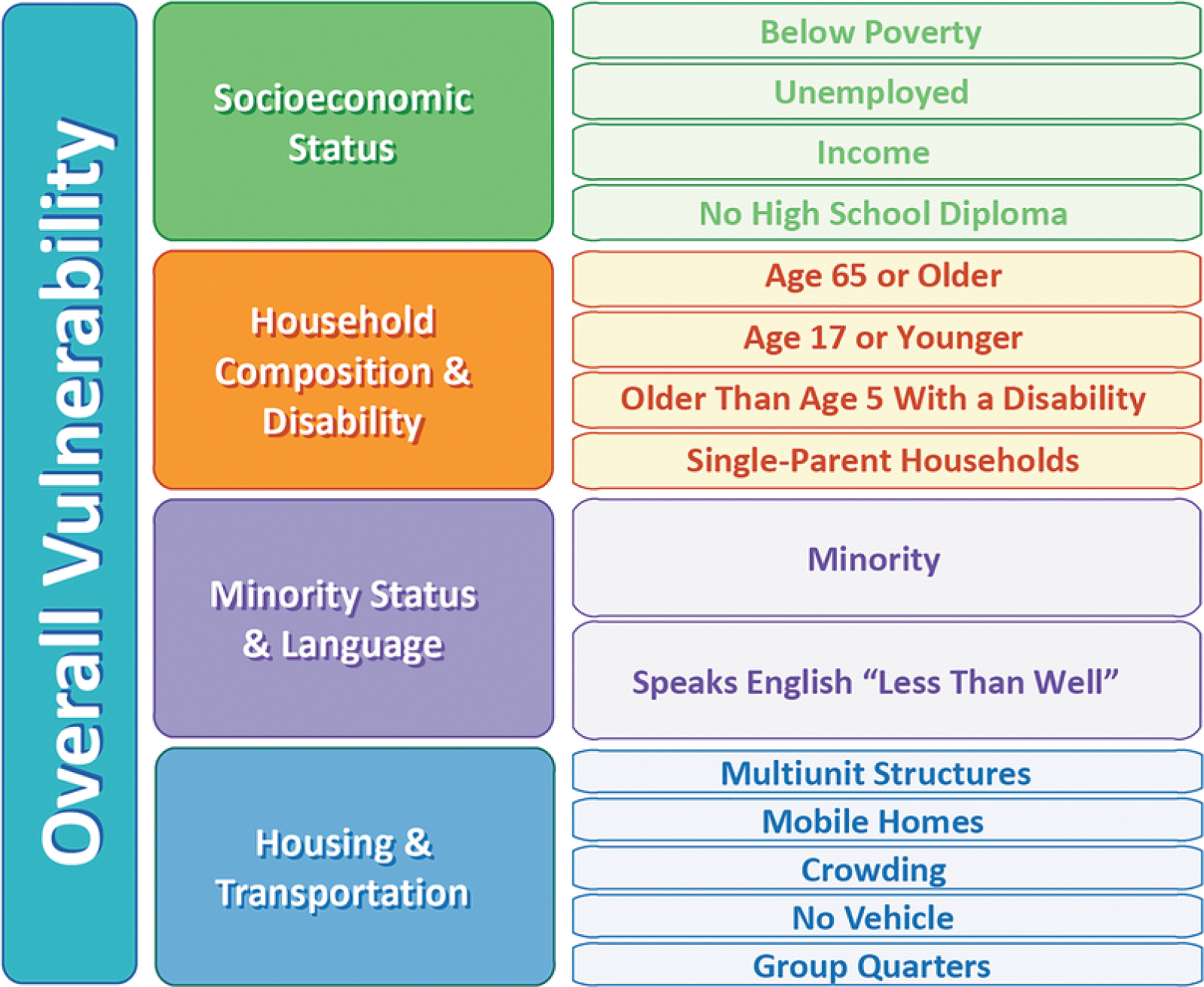
Elements of the Social Vulnerability Index. Census variables are grouped thematically into 4 categories: socioeconomic status, household composition and disability, race/ethnicity and language (minority status), and housing and transportation. Rankings are based on percentiles. Percentile ranking values range from 0 to 1, with higher values indicating greater vulnerability. 10
Before the COVID-19 pandemic, the Clarkston community faced substantial and persistent disparities that affected health outcomes. Residents had low incomes, high unemployment, employment in low-wage jobs, limited or no health insurance coverage, large families living in densely populated housing, and an inability to access systems that provide needed resources.6,11,12 In our study of healthcare access and social determinants of health in the community, average income ($15,476) was below the poverty level, 41.2% of respondents were employed, 66.9% had been in the United States less than 3 years, 29.4% had health insurance, and 57.4% reported limited English proficiency.6,11 A lack of English-language proficiency along with poor living conditions further compound social stigma and a mistrust of medical institutions and public health resources. 13 Having fled situations of oppression, often from their own governments, and facing rumors, misinformation, and information overload upon resettlement, refugee populations tend to be highly suspicious of institutional and governmental messaging. 14 As indicated by US Centers for Disease Control and Prevention reports, socioeconomically impoverished communities have suffered the brunt of the pandemic disproportionately 15 and for a superdiverse community like Clarkston, the impact has been uniquely challenging. The simple task of communicating risk mitigation, testing information, and vaccine guidance has been daunting. Beyond language barriers, delivering messaging from trusted sources has been yet another challenge to overcome.
Both the physical and mental health-related consequences of forced displacement are profound. 16 Many refugees who were forcibly displaced have had high rates of exposure to torture and violence and have witnessed or experienced human rights abuses. Compared with the general population, refugees have higher rates of anxiety, depression, posttraumatic stress disorder, psychosis, and dissociation. 17 In 2 cross-sectional studies in Clarkston before and during the COVID-19 epidemic, more than 66.0% of refugee respondents felt high levels of daily stress. 18 Refugees come to the United States with limited English proficiency, often limited literacy in their own language, and poor-quality, basic, or interrupted education.6,11,18 When refugees reach the United States, a small, short-term package of services is provided by resettlement agencies contracting with the US Department of Health and Human Services that can include around 6 months of housing and benefits support (eg, health insurance, food stamps), English instruction, and employment placement. 19
Even with this support, Clarkston's refugees continue to struggle with access to basic healthcare, high rates of mortality and morbidity, trauma-induced stress, lack of health insurance, and high rates of poverty and unemployment.12,20 Almost 70.0% of Clarkston refugees do not know where to get benefits such as financial assistance, unemployment, or healthcare. 18 Further, healthcare services in the community are often fragmented or duplicative and myriad needs (eg, eye care, dental care, mental health services) go consistently unaddressed; 12 cultural and language dissonance exacerbate the challenges that refugees face in accessing healthcare services. 6
The lack of culturally and linguistically appropriate health promotion materials has left refugee populations at high risk of not being able to find, understand, or use health information both before and during the COVID-19 pandemic.6,21 For Clarkston refugees, this low level of health literacy (66.2% of respondents had low health literacy) is directly correlated with poor health status and poor health outcomes. 6 Low health literacy skills also affect one's ability to understand how the body works, manage sick behaviors, know about preventive behaviors, and seek and use health information. 22 A further complication is low reading skills. Because 1 in 5 US adults read at elementary school levels, 23 more than 66 million Americans are potentially at risk of not being able to read or understand most of the materials currently written about COVID-19. Adults with low reading skills both in English and in their native language struggle with understanding the plethora of online and offline health communications. 24 In our recent study, 58.0% of Clarkston refugee respondents reported having limited English proficiency, 95.0% of patients reported language as the primary barrier to accessing healthcare, and 85.0% of healthcare providers reported language as a primary barrier to providing care. 6 Refugee populations face a higher barrier in addition to poor reading skills in English; they may have low or no written literacy in their native language, cultural discordance with healthcare providers, a lack of trust in the sender of the message, inadequate translation services, and difficulty parsing the technical, jargon-laden language of health and healthcare. 24 A pre-COVID-19 study in Clarkston confirmed that the primary barrier to healthcare access for both patients and healthcare providers in this community is language. 6
The Effect of COVID-19
The intensity of the COVID-19 pandemic has disproportionately affected refugee residents in Clarkston. Local epidemiological data for this city of 17,000 is unavailable, but based on smaller studies in the community, we have documented what is also found in other studies about refugee, immigrant, and migrant communities: lower testing rates, higher COVID-19 infection rates, and higher death rates. The root causes of vulnerability and inequity for these community members remain unchanged. However, the pandemic has highlighted existing disparities and brought into focus how circumstances such as the lack of digital access, digital literacy, and language proficiency further marginalize the vulnerability of low socioeconomic status communities.21,25 The problem is compounded by the economic impact on refugees, who are more likely to earn their income in the hardest-hit industries (eg, manufacturing, service-based, food processing). 26 In fact, according to the Clarkston city manager (Robin Gomez, email communication, January 21, 2021), for those who received rent assistance through Cares Act funds, the majority in Clarkston were Uber/Lyft drivers and restaurant or retail workers—industries severely affected by the pandemic. Not only do refugees work in jobs where they may be exposed to COVID-19 (and also often live in overcrowded housing where there is increased risk of transmission), but they are subject to layoffs, reduced work hours, or unemployment. They cannot work from home, are the sole provider for their family, and their reduced income affects their ability to pay rent, buy food, and seek healthcare. 26
Many refugee communities have a profound mistrust of the media, public health agencies, healthcare providers, and government organizations, resulting in the fomenting and fueling of myths and misinformation about COVID-19. 27 Although mistrust and misinformation are not new public health phenomena, the recent proliferation of social media provides a platform where falsehoods are both created and disseminated quickly. The United Nations Secretary-General António Guterres recently called COVID-19 a “pandemic of misinformation,” which has involved the rapid spread of inaccurate and even harmful home remedies that can supposedly prevent or cure the disease. 28 Social influencers who drive anti-science and anti-government rhetoric, coupled with weak political leadership, fuel conspiracy theories against public health initiatives29,30 and add to the complexity of communicating health information about COVID-19. Evidence from the HIV epidemic demonstrated that mistrust and misinformation have been associated with beliefs that medications are less necessary for maintaining health among individuals with HIV. 3 Individuals who were more mistrustful of medical organizations and more likely to endorse conspiracy beliefs were less likely to seek care during the Ebola epidemic. 8 Our current work with the refugee community in Clarkston has revealed profound mistrust of some news outlets, public health agencies, and healthcare providers as well as rampant myths and misinformation about COVID-19 (eg, racial/ethnic minorities and people from warm climates cannot acquire the disease, black tea can cure the disease, the disease was developed to eradicate racial/ethnic minorities).11,18
Disease containment strategies (eg, physical distancing, wearing a face mask, travel restrictions) can exacerbate stigma and xenophobia by encouraging “othering,” avoidance, and mistreatment toward people associated with COVID-19. 31 Recent news describes personal attacks against individuals suspected of testing positive for COVID-19, or of unknowingly infecting others. 32 Travel restrictions and the blaming of foreign “others” for disease transmission is likely to disproportionately affect vulnerable populations such as refugees and both documented and undocumented immigrants.31,32 Evidence suggests fear of social marginalization may negatively influence voluntary testing among individuals at risk of HIV. 33 Another study reported that refugees and immigrants were often reluctant to be tested for tuberculosis because of stigmatization concerns. 34 Stigma may also cause people to engage in riskier behaviors, deny clinical symptoms, and avoid seeking timely treatment as well as not adhere to treatment.35,36 Finally, stress from COVID-19 stigma may have a profound mental health impact. 37 Our current research indicates that many Clarkston residents feel concerned about being judged negatively if they seek COVID-19 testing or if they test positive for COVID-19 and admit to avoiding testing as a result. Stay-at-home orders and requests to wear masks may also propagate mistrust, stigma, fear, and marginalization in a community habituated to evading governmental and institutional authority as a result of their lived experiences of flight from persecution and oppression in their homelands. 37
Refugees have been marginalized by anti-immigrant public rhetoric, US Immigration and Customs Enforcement raids, the separation of children from parents, denial of permanent legal status to immigrants with legal protections to stay in the United States, dismantling of the refugee resettlement program, and reduction in social support services for refugees. 38 The Trump administration executive orders to ban migration from majority-Muslim nations, slash refugee admission numbers, and deny citizenship to legal immigrants had far-reaching repercussions in the communities where new arrivals had been welcomed for decades. 38 In Georgia, a local gubernatorial candidate drove a “Deportation Bus” to the heart of a refugee community and parked the vehicle emblazoned with messages reading: “Danger! Murderers, rapists, kidnappers, child molesters, and other criminals on board” for a campaign stop. 39 The provocations further marginalized Clarkston residents and fomented distrust and suspicion among community members who were already struggling to create a new life, learn a new language, adjust to different employment options, and overcome the substantial stressors associated with acculturation.
As the pandemic unfolded, specific needs of Clarkston residents were revealed by various organizations, local governments, community-led task forces, and researchers gauging how to best protect this high-risk community.40-42 With large numbers of refugees employed as contract laborers in service-based industries, rent assistance and food security became top priorities. The availability and affordability of personal protective equipment was also revealed to be a barrier to implementing recommended mitigation strategies. 42 Testing accessibility is another formidable obstacle. There are few test providers and many refugees lack transportation to reach testing sites. 43 Compounding all of these social determinants was the vast amount of misinformation in the refugee community about COVID-19. 44 Many refugees did not trust the guidance provided by government, public health agencies, and healthcare providers about the gravity of the situation.21,43 This distrust and misinformation may continue as the COVID-19 vaccine is rolled out, although vaccine hesitancy has not been systematically measured in any refugee communities within the United States to date. However, given historic mistrust in certain communities, a high level of misinformation and disinformation, and the novelty of the COVID-19 vaccine, continued vaccine hesitancy can be anticipated. 45
Communicating Risk
Although communicating about risk has a long history, modern risk communication can be traced back to the 1950s in the United States during the “Atoms for Peace” campaign; a more recent contextualization of risk communication occurred during the mid-1980s when William Ruckelshaus, the Environmental Protection Agency administrator, advocated for environmental risk management including community right-to-know principles. 46 The first formal legislation requiring community right-to-know passed in 1986 as the Emergency Planning and Community Right-To-Know Act, focusing on chemical storage, toxicity, and transportation. 46 Risk assessment, management, and public communication were foundational elements of risk communication policies; its source-oriented approach enabled experts to both perform epidemiologic studies to understand the extent of risk and harm and to communicate effectively to increase understanding of the issue and ensure those involved felt adequately informed. 47
Historically, the United States has been a complex ethnic and racial society, with Americans having multiple identities framed by ancestral origins and languages as well as varied outlooks on culture and race. 48 When the first risk communication legislation was written and passed in 1986, there were no US senators of color and only 21 (less than 5.0%) US house representatives of color. 49 Since then, policies and practices of risk communication have evolved to include perspectives and needs of minority populations. 46 Plain language guidelines and culturally and linguistically appropriate standards help address improvements in risk communication to adults with low literacy or those with limited English proficiency.50,51 Understanding how social determinants of health, such as housing, income, and education, affect risk communication has also improved the effectiveness of risk communication. 52 However, other systemic issues impede the effectiveness of risk communication to benefit vulnerable and marginalized communities, in particular for the millions of refugees, immigrants, and migrants in the United States today.
Recommendations
Current COVID-19 risk communication strategies have further marginalized vulnerable refugee communities.21,25 To improve these and other disparities, ingrained and inequitable policies for refugees need to be addressed with a broader lens than simply improving risk communication. We learned in Clarkston that there was a great need for a centralized effort to address the threat of COVID-19. Healthcare providers in the community assembled a volunteer Clarkston Community COVID-19 Task Force, which met weekly to share information, strategize, and collaborate on community-wide efforts to address the pandemic. Volunteer representatives from local resettlement agencies, health clinics, the local board of health, local government, and academic partners lead the activities of the task force. The task force began by conducting a community-wide needs assessment of the impact of COVID-19 on social determinants of health for community residents. With this information, the task force strategized a door-to-door distribution of 28,000 personal protective equipment kits, which contained masks, hand sanitizer, and COVID-19 health information; launched a community-wide mitigation and testing campaign; and created vaccine guidance videos and social media posts available in a wide range of languages. Community agencies were able to focus other social support efforts on areas identified by the needs analysis including food insecurity and rent assistance.
In addition to a local task force, other recommendations should also be considered. First, prolonged high-quality language and literacy services should be available for refugees immediately upon arrival to gain oral proficiency in English. 53 Limited English proficiency keeps refugees relegated to a socioeconomic stratum that prevents them from accessing education, jobs, and healthcare they need to improve and enrich their lives.20,54 Refugees often have difficulty accessing social service benefits (eg, health insurance, childcare, nutrition services, mental health services) due to limited English proficiency. Gains in English proficiency not only help individuals but also help improve community resilience as measured by the Social Vulnerability Index. 10 Relatedly, although patients with limited English proficiency in the United States have a legal right to access language services, and clinicians have legal and ethical responsibilities to communicate through qualified interpreters when caring for these patients, there remains inadequate access to or sporadic use of these services. For example, because healthcare facilities are often unable to have qualified bilingual staff on site who can communicate in all of the patients' preferred languages, ad hoc interpreters (a broad category that includes a patient's friends or family members) often step in. However, evidence indicates that the use of ad hoc interpreters can result in reduced trust in physicians, lower patient satisfaction, breach of patient confidentiality, inaccurate communication, misdiagnosis, inadequate or inaccurate treatment, and reduced quality of care.55-57 Thus, healthcare systems need to ensure they are informing patients about these rights before a healthcare encounter and maximizing their own capabilities to offer certified language interpretation by contracting with telephonic or videoconference services for access to interpretation services on demand.55-58
Second, refugee perspectives on risk, health, and wellness should be respected and incorporated into both risk communication and general health messaging.58-60 Refugees experience substantial levels of acculturative stress during their assimilation into American society that can often be more taxing than the stressors experienced before and during their flight from home.61,62 Cultural myths, stigma, and fear of authorities are well documented in the refugee community, yet there is little data addressing the use of evidence-based standards to improve acceptance of risk or health communication.61,62 Solutions for these vulnerable communities should take into account individual and actual experiences and knowledge rather than only population-generalized data. These efforts are particularly important in the context of addressing misinformation and promoting awareness of the COVID-19 vaccine in refugee, immigrant, and migrant communities. Our team is currently conducting focus groups with 7 different language groups in Clarkston to document knowledge, attitudes, and beliefs about the vaccine to inform the development of culturally and linguistically tailored vaccine-related messaging. Focus group participants are also being asked about the modalities by which they prefer to receive such health information (eg, print, phone call, text, email, social media, in-person) so the dissemination of such health communication messages can have maximal reach. Others have initiated similar efforts to make vaccine information available in multiple languages and use culturally appropriate images and messaging. 63 Simply translating an intervention into a particular language does not make that intervention meaningful or usable. In fact, programs aimed at stigma reduction that do not engage the stigmatized community have been shown to fail dismally for both the individual and society. 62 Refugees can also provide insight into the psychosocial context in which their health behaviors occur; individual behaviors fall within the realm of the social context, which exerts influence by shaping and reinforcing community norms.51,60,63
Third, education and training for anyone involved in providing healthcare or health promotion and education should include specific health literacy and intercultural competence communication training to enhance patient-centered care. 51 Data show that health-literate communication skills can be learned through intentional and systematic training.64-66 There are 150 accredited US medical schools 67 ; few have separate and distinct cultural competence and health-literate communication skills courses in their curricula, relying instead on embedded instruction in other courses. Critical health-literate and culturally competent communication skills affect how information is shared, understood, and acted upon by patients.68,69
Fourth, there should be an increase in paid community health workers (CHWs) from within each ethnic community. CHWs provide vital services to refugee health and wellbeing. 70 Because they are from the communities, CHWs can assist with navigation by ensuring residents have descriptions of support services (eg, healthcare, transportation options, after-school care, childcare, job training, language classes, legal assistance) and maps of their locations within the community. CHWs play an important role to clinicians because they also assist with patient navigation for referrals, benefit applications, and medication education to improve patient adherence and access to health services. Frontline CHWs are often more trusted than clinical and public healthcare providers because they are members of the community, have deep understanding of the community they live in, and build trusting relationships with their friends and neighbors. 71 CHWs understand the role of social norms within their communities, are culturally competent, and can transform communities through patient and community education, outreach, social support, and advocacy. 71
Fifth, public health agencies and health promotion and education professionals should be better prepared by anticipating, planning, and implementing alternatives to print materials for the tens of millions of US adults who have low reading skills or who are nonnative English speakers. US adults with low literacy skills rely more often on radio, television, and the internet than on printed information with an online focus on social media sources.72-74 Materials should be developed using culturally and linguistically appropriate standards, plain language, and other health literacy guidelines, such as being action oriented and concrete.50,51 Creating audiovisual materials in multiple languages for television, radio, and social media can help raise awareness and change attitudes and behaviors by reaching people where they are with clear, understandable, and actionable messages. 74 Messages should focus on what people need to know in times of a pandemic to take care of themselves and their families; messages that answer the question, “What should I do?” are more likely understood and acted upon. 75
Finally, risk communication plans need to be put in place with community leadership before emergencies and disasters occur so individuals can rely on their own trusted source for accurate information. A key element of risk communication is getting trustworthy, easy-to-understand, and actionable information into peoples' hands without delay. 1 Strong partnerships and coordinated efforts between community organizations that serve similar populations can assist with delivering trustworthy information in a timely manner.76,77 Refugees who live in vulnerable communities tend to trust those they know, such as a religious leader, adult education teacher, or community organizer. 77 Health professionals and public health organizations can help disseminate critical health information to communities by partnering with local trusted sources.
Existing systemic disparities have been exacerbated by COVID-19 for all vulnerable populations in the United States. 78 Along with changes in the healthcare system, local, state, and federal policies should be changed to democratize health, education, social services, and other social determinants of health to ensure the impact of a pandemic does not further disadvantage these populations. The pandemic has exposed the vulnerabilities of communities most at risk because of structural inequities; refugees are clearly one of those groups that warrant our collective attention. While this article focuses on a local refugee community, it must be situated in the context of the growing global migration crisis. Both global and local (US) systemic racism and xenophobia make refugees among the most marginalized populations on the planet. Under President Obama, the United States was resettling more than 85,000 refugees per year; that number dropped to 30,000 during the Trump administration. However, the numbers of forcibly displaced people have doubled since 2012, and nations have been closing their doors to refugees; less than 1.0% of displaced individuals can expect to be resettled in a new home. 79 Escalating anti-immigrant sentiment around the world has widened the gap between the involuntarily displaced and services to support them. We anticipate the reopening of our borders along with funding for supportive services under the current administration; the Biden administration has pledged to revitalize the refugee resettlement program and is planning to admit up to 60,000 refugees in 2021 and double that number in 2022. 79 If lessons learned from ineffective risk communication and health education and promotion during this COVID-19 pandemic can be implemented, we may have the opportunity to ameliorate inequitable health for refugee communities in the United States.
Footnotes
Acknowledgments
We appreciate and acknowledge the many contributions of Clarkston collaborators and residents, without whom this work would not be possible.