
Abstract
This paper presents research conducted by the Arlington County Department of Human Services to understand the use of safety net services during the pandemic, identify disparities, and reduce or eliminate them. Arlington County's levels of health and economic wellbeing are generally high; however, residents of color experience significant disparities compared with White residents, with lower median incomes, lower rates of college completion, lower life expectancies, and higher rates of chronic illness. During the COVID-19 pandemic, these disparities were amplified as Black and Latinx residents experienced disproportionately high rates of COVID-19 infection, hospitalization, and death, as well as disproportionately high rates of job loss. During the COVID-19 pandemic, Arlington County mounted an interdisciplinary response to stabilize community needs, including food security, eviction prevention, isolation housing, behavioral health stabilization, and digital equity. This integrated approach was especially important during the pandemic, as the direct and indirect effects of the pandemic disproportionately impacted health and economic wellbeing among Arlington's Black and Latinx residents, low-income residents, and vulnerable communities.
Introduction
Arlington County, Virginia, is an urban community located directly across the Potomac River from Washington, DC. Arlington's levels of health and economic wellbeing are generally high, with a median income of over $120,000, 1 75% of residents aged 25 years and over holding a bachelor's degree or higher, 2 an average life expectancy of 85.2 years, 3 and the title “Fittest City” from the American College of Sports Medicine. 4 However, residents of color experience significant disparities compared with White residents, with lower median incomes, lower levels of educational attainment, lower life expectancies, and higher rates of chronic illness. Development in corridors served by rapid transit has resulted in economic growth; however, comparable levels of growth have not been seen in all parts of the county. 5 In the ZIP codes with the highest level of disparities, life expectancy is up to 10 years lower 6 ; poverty rates are 32% higher 7 ; median income is 26% lower 8 ; and rates of diabetes and asthma are higher than in the rest of Arlington. 9 Although 70% of Arlington residents are White, the majority of residents in these underserved ZIP codes are people of color. 10
Arlington County Department of Human Services
The Arlington County Department of Human Services provides a uniquely integrated response to health and social needs, combining social services, housing assistance, employment services, behavioral health, and public health in a single organization. As the anchor of Arlington County's safety net system, the Department of Human Services (DHS) receives more than 56,000 walk-in visits to the customer service center each year. In addition, DHS works in close partnership with nearly 50 area nonprofit organizations to meet the full range of community needs.
DHS strives to provide integrated services in a coordinated, collaborative, client-centric, and equitable manner. Service integration offers the chance to respond holistically to the needs of communities affected by poverty and systemic racism, addressing needs across life domains and avoiding the challenges of fragmented care that fails to address the social determinants of health. During the COVID-19 pandemic, integrated care has been especially important, as the direct and indirect effects of the pandemic disproportionately impacted health and economic wellbeing among Arlington's Black and Latinx residents.
Countywide Work Toward Racial Equity
Before the pandemic, Arlington County had begun enterprise-wide work on racial equity, including racial equity training for leadership through the national nonprofit Government Alliance on Race and Equity (GARE), 11 and passage of an equity resolution by the Arlington County Board. 12 In addition, DHS had begun to work on racial equity by mapping existing disparities in the community through the Destination 2027 public health initiative, 6 providing GARE training for all managers, creating a multidisciplinary racial equity advancement team, and piloting a process to disaggregate results-based accountability performance measures by race and ethnicity to understand disparities in access and outcomes of services. During the COVID-19 pandemic, Arlington enhanced its focus on race and equity by appointing a chief race and equity officer, conducting training and dialogues with staff across departments, and facilitating conversations in the community.
Responding to Challenges During Pandemic
Research on the effects of COVID-19 has shown a disproportionate impact on vulnerable populations in terms of COVID-19 incidence and mortality rates and economic consequences. 13 For populations in Arlington who already experienced poverty and systemic racism before the pandemic, COVID-19 exacerbated their challenges, resulting in disproportionate impacts to health, economic security, basic needs, and behavioral health. Arlington worked to identify early indicators of disproportionate impact, mobilize resources, and adapt services to ensure access and support for those most at risk.
Research on Use of Safety Net Services and Disparities
We analyzed data on COVID-19 cases, hospitalizations, and deaths; unemployment; food insecurity; housing instability; and behavioral health outcomes in Arlington County from a variety of public data sources—including the American Community Survey by the US Census Bureau, the Virginia Department of Health, and the Virginia Employment Commission. 14,15 In addition to public data sources, we analyzed administrative data, which was aggregated and deidentified, 16 on usage of safety net services during the pandemic. Results were disaggregated by race and ethnicity wherever possible.
While the race and ethnicity categories varied across some data sources, we used the US Census Bureau groupings whenever possible—White, Black, Asian, Latinx, and non-Latinx. Because Arlington's Native American and Native Hawaiian/Pacific Islander populations are estimated by the Census Bureau to be very small (1,127 individuals, 0.5% of the population), data for these populations were not reported separately for most measures.
COVID-19 Cases, Hospitalizations, and Deaths
Through January 11, 2021, Arlington County reported 10,117 COVID-19 cases (4.3% of the population), 17 687 hospitalizations (6.8% of cases), and 186 deaths (1.8% of cases, 27.1% of hospitalizations).18,19 Similar to national trends, older adults in Arlington were more likely to require hospitalization and more likely to die of COVID-19. 20 Adults aged 20 to 59 years made up 56.8% of Arlington's population in 2020 and accounted for a disproportionately large share of COVID-19 cases (69.9%); however, adults in this age group accounted for only 11.4% of deaths. Adults ages 60 years and older made up only 16.9% of Arlington's population and 14.7% of COVID-19 cases, but they accounted for 48.4% of hospitalizations and 88.6% of deaths. 19
Holtgrave et al 21 developed a framework for assessing the incidence and outcomes of COVID-19 infection among communities of color. Applying this framework to Arlington shows that Black and Latinx individuals were more likely to contract COVID-19 and be hospitalized than White and Asian individuals (Figure 1). The death rate for Black individuals was more than twice as high as the death rate for any other racial/ethnic group. Non-Latinx Black individuals accounted for only 8.7% of Arlington's population, but they accounted for 22.8% of Arlington's COVID-19 deaths (Figure 2). 19
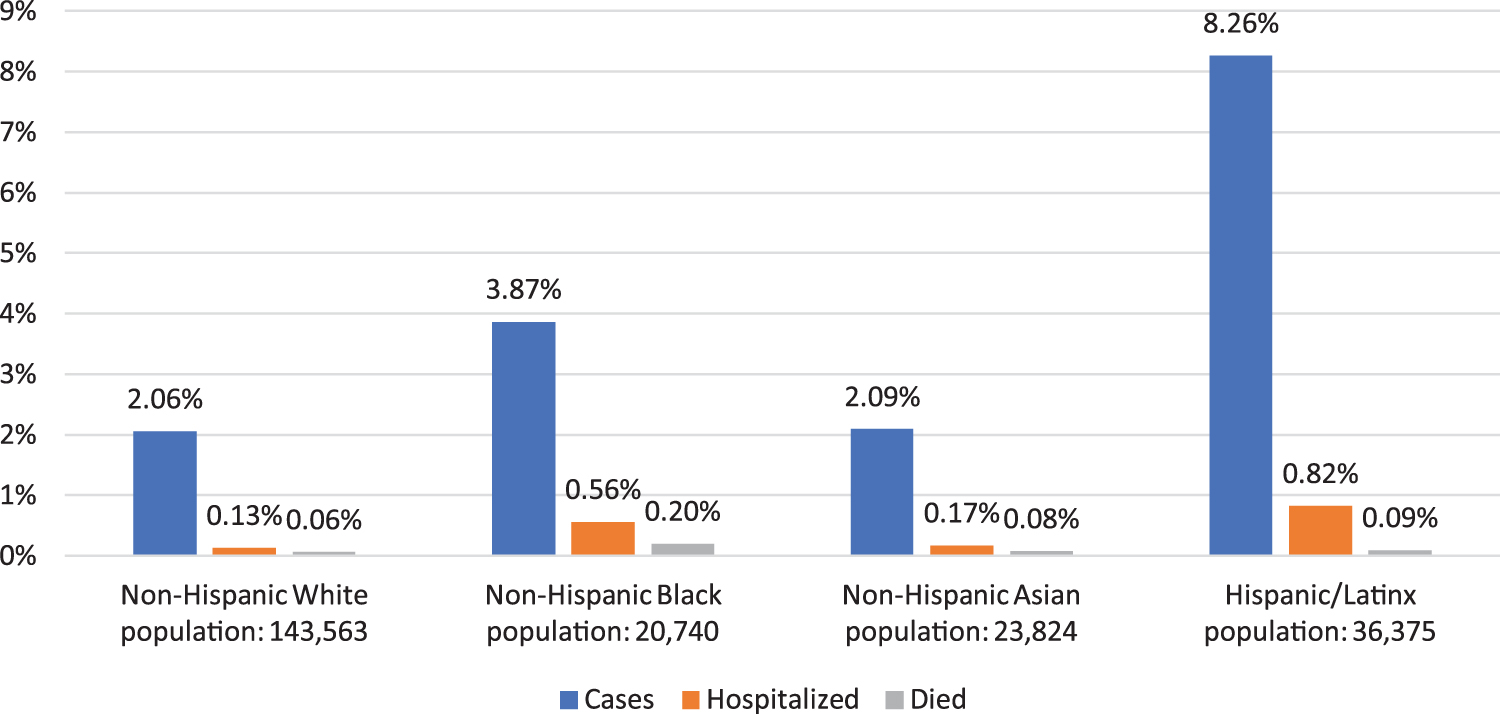
COVID-19 cases, hospitalizations, and deaths as percentages of population by race and ethnicity. Data derived from the Northern Virginia Regional Commission. 19
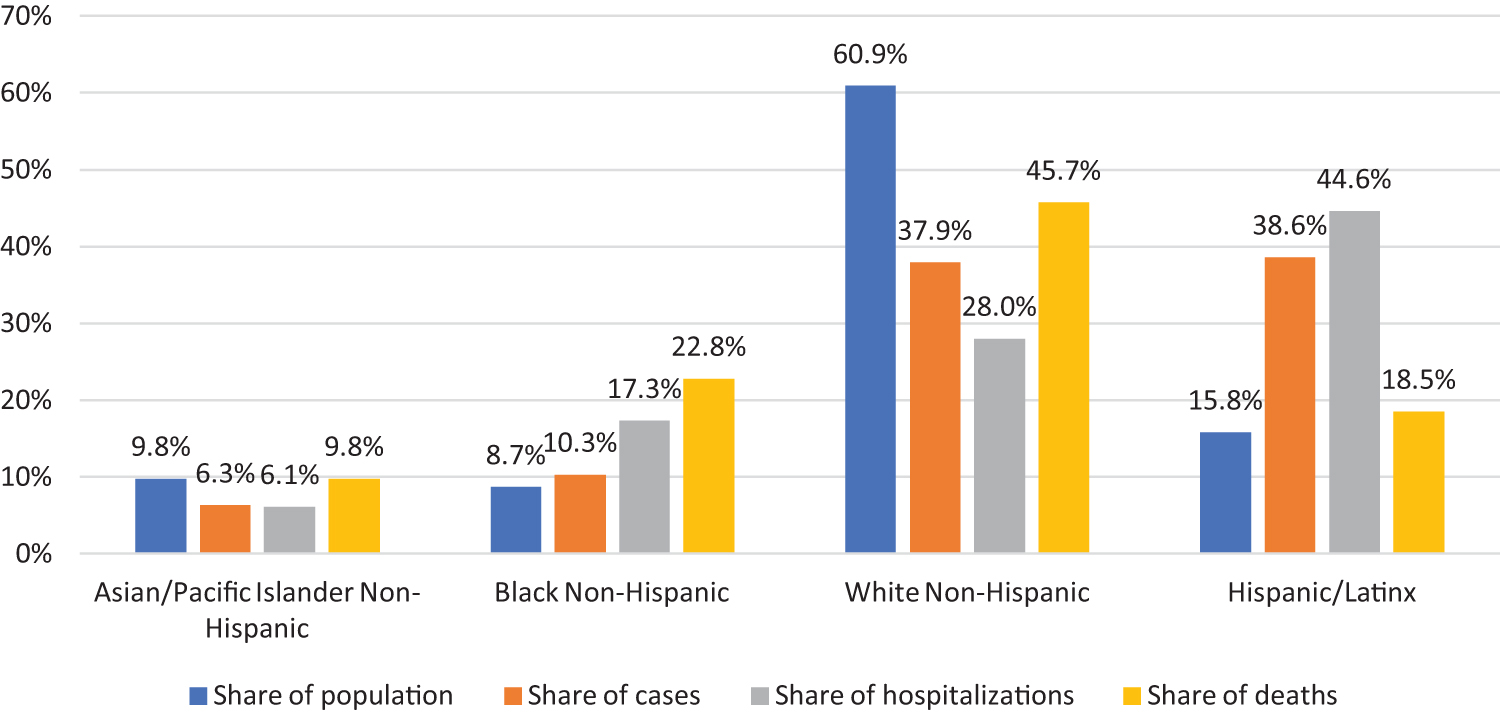
Percentages of population, COVID-19 cases, hospitalizations, and deaths by race and ethnicity. Data derived from the Northern Virginia Regional Commission. 19
Unemployment
The Northern Virginia region experienced a sharp increase in the level of unemployment at the start of the COVID-19 pandemic—from 2.2% in February 2020 to 10% in April 2020 (Figure 3). 22
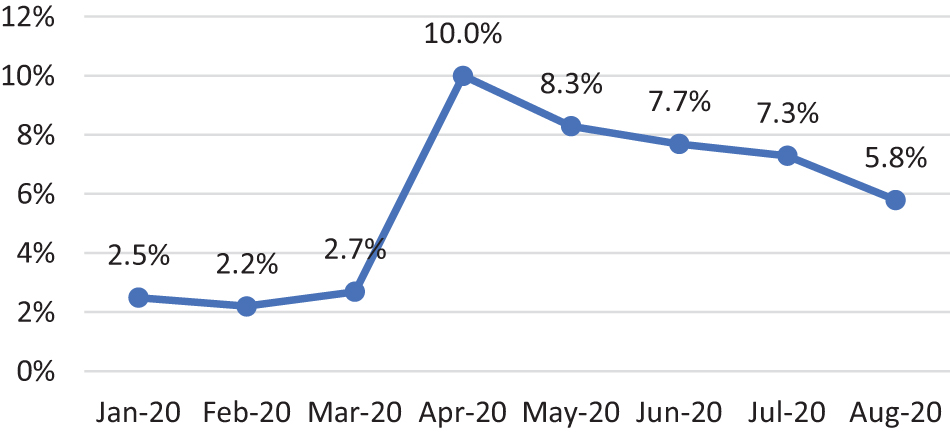
Northern Virginia unemployment rate, January to August 2020. Data derived from Northern Virginia Community College. 22
According to data from the Virginia Employment Commission (VEC) and the American Community Survey, approximately 12% of Arlington residents in the workforce filed an initial unemployment claim between March and August 2020. 15 Workers aged 16 to 24 years and workers aged 65 years or older were more likely to file an unemployment claim than workers aged 25 to 64 years. Unemployment claims were geographically concentrated in ZIP codes with higher levels of vulnerability as measured by the US Centers for Disease Control and Prevention Social Vulnerability Index (SVI). 23 Disparities were apparent when the data were disaggregated by race and ethnicity. While 7.5% of White employees filed an unemployment claim, the rate for Asian, Native American, and Latinx employees was 14.7% to 16.2%. The highest unemployment rate was seen among Arlington's Black employees, 37.3% of whom filed an unemployment claim. 15 Figure 4 shows areas of high SVI and the concentration of unemployment claims in high-SVI communities (also see Supplemental Table 1, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041).
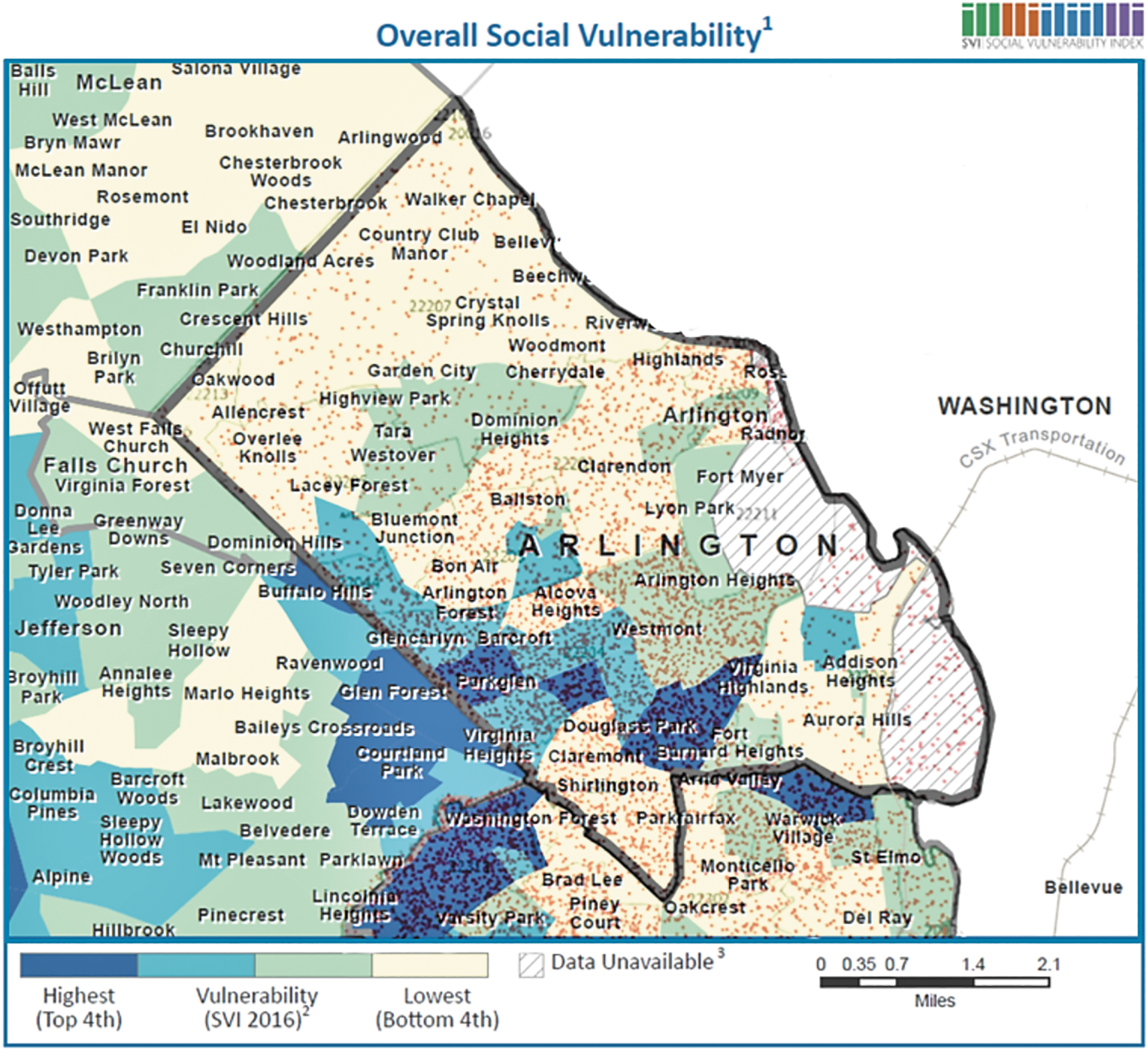
Unemployment claims and social vulnerability in Arlington County. Teal and blue areas indicate communities with a high Social Vulnerability Index. Red points, derived from the Virginia Employment Commission, 15 indicate the concentration of unemployment claims in communities with a high Social Vulnerability Index. Base image from CDC's Social Vulnerability Index 2016. 23
Frontline service occupations experienced the highest volume of unemployment claims. Between March 1 and December 5, 2020, 46,331 new initial unemployment claims were filed in the Arlington-Alexandria City Workforce Development Area, and VEC data indicates that 17% of these claims were in occupations related to food preparation and serving. 15 The 3 occupations experiencing the highest unemployment rate during this time period were food preparation and serving, personal care and service, and healthcare support. All 3 had a workforce in which 50% or more of Arlington resident workers identified as people of color and had an average salary of less than $40,000. 25-27 Further analysis by race and ethnicity was not possible due to the limited data available from the American Community Survey for small geographies (see Supplemental Table 2, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041).
Food Security
The largest sources of food assistance in Arlington County include the federal Supplemental Nutrition Assistance Program (SNAP), the nonprofit food bank Arlington Food Assistance Center (AFAC), and home-delivered meals serving senior citizens and people with disabilities. These programs are complemented by multiple food pantries, county citizen associations, and volunteer organizations that coordinate additional efforts to ensure food security among Arlington County residents.
Feeding America estimated that 6.7% of Arlington residents experienced food insecurity in 2018. 28 In 2020, Feeding America projected that Arlington County would experience a 36% increase in overall food insecurity and a 216% increase in child food insecurity due to COVID-19—the second-highest projected increase in child food insecurity in the country.29,30
As predicted, the need for food assistance in Arlington has increased during the COVID-19 pandemic. Between March and September 2020, an average of 6,351 individuals per month received SNAP benefits, and AFAC served an average of 8,184 individuals per month. Enrollment rates varied across the 2 programs, however. SNAP enrollment rose steadily between 2019 and 2020: SNAP served 3% fewer clients in March 2020 than March 2019, but by September 2020 SNAP enrollment was 22% higher than it had been in September 2019. AFAC enrollment, on the other hand, peaked in May 2020, when AFAC served 25% more clients than in May 2019. As a locally administered program, AFAC's application requirements are streamlined, enabling AFAC to respond more rapidly than SNAP to emerging food insecurity; however, SNAP provides eligible recipients with more sustainable support for long-term needs.
Studies have shown that food insecurity increased significantly among racial and ethnic minorities during the COVID-19 pandemic.31-34 Increasing the percentage of eligible residents—those with incomes less than 125% of the federal poverty level—who participate in SNAP is an effective approach to reducing food insecurity in the community. 35 The state of Virginia made significant SNAP policy changes to increase access during COVID-19, which included waiving interviews, extending eligibility time frames to ensure uninterrupted participation, issuing the maximum benefit allotments, and issuing separate Electronic Benefits Transfer cards to students eligible for free and reduced lunches.
Following these changes, SNAP participation increased. Between 2017 and 2019, approximately 25% to 30% of potentially eligible Arlington residents participated in SNAP, with the highest participation rate seen among Black residents and the lowest among Asian and Latinx individuals—potentially due to the higher percentage of residents who may not meet SNAP's citizenship or residency requirements. During the pandemic, participation rates increased across all demographics, especially in Black communities where the percentage of potentially eligible residents participating in SNAP increased from 48% in September 2019 to 62% in September 2020. 36 These results suggest that Virginia's policy changes have been effective in increasing SNAP participation and reducing food insecurity in communities who were hit the hardest by economic consequences of the pandemic (see Supplemental Table 3, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041).
Across both SNAP and AFAC, participation among Latinx clients experienced the greatest percentage increase during the COVID-19 pandemic—SNAP served 28% more Latinx clients in July 2020 than in July 2019, and AFAC served 36% more. Morales et al 36 found that there is a long-standing food security gap between Latinx and White households and identified deportation fears as a potential driver of food insecurity for the Latinx population. While Latinx clients made up only 15% of Arlington SNAP recipients in September 2020, they represented 55% of AFAC recipients. 16
Food insecurity also increased significantly among older adults. Arlington's home-delivered meals program for seniors saw year-over-year increases of up to 136% in the total number of clients served each month between March and September 2020. 16 The program adjusted its services rapidly to meet the increase in demand by recruiting new volunteers, nonprofit partners, and staff to deliver meals; setting up direct delivery of meals to affordable-housing communities; using CARES Act funding 37 to provide meals at no cost to vulnerable older adults in targeted communities; and recruiting volunteers for a friendly caller program to provide social contact and wellness checks to vulnerable adults. These efforts resulted in increased enrollment across all racial and ethnic groups, particularly among Latinx, Asian, and Black clients. 16
To address escalating food security needs, Arlington County established the Cooperative for a Hunger Free Arlington in April 2020, a collaborative task force coordinating food assistance for Arlington residents in need. The task force has collected and mapped information on food resources from government, schools, nonprofits, and the faith community. The cooperative established new community food distribution sites in Arlington. In partnership with Arlington Public Schools, free grab-and-go meals were provided for children aged 2 to 18 years at 22 schools and 7 community sites across the county. Other successful measures included a grocery card pilot program, which provided a total of $400,000 in funding to qualifying families in need of food. With an additional $200,000 contribution from the Arlington Community Foundation, the county anticipates serving up to 500 families for 6 months, at a projected cost of $200 per family per month. 16
Eviction Prevention
According to the Pew Charitable Trust, households spending more than 30% of their annual pretax income on rent are considered rent-burdened. 39 These families are at increased risk for eviction and more likely to rely on safety net programs to meet other basic needs. In Arlington County, 57% of households rent their homes, and 38% of renters are rent-burdened.40,41 Among households earning $74,999 or less, however, the percentage who are rent-burdened rises to 81%. The proportion of renters is higher among people of color: 69% of Latinx households and 85% of Black households are renters, whereas 52% of White households are renters.40,41
According to a policy paper from the Urban Institute, COVID-19 relief measures such as eviction moratoria, tax relief payments, and enhanced unemployment benefits have helped renters affected by COVID-19, 42 but the most sustainable solution to meet the needs of renters and landlords during the pandemic has been the use of CARES, Community Development Block Grant, and other funding sources to provide direct rental assistance payments to landlords. To help households avoid eviction, Arlington County leverages a variety of state, federal, and local funding sources to provide eviction prevention assistance, including short-term rental assistance and case management to connect households to sustainable sources for addressing basic needs.
Before the COVID-19 pandemic, between July 2019 and March 2020, an average of 145 households per month received eviction prevention assistance. Assistance was funded primarily through local sources. During the pandemic, the average number of households assisted increased to 342 households per month (a 136% increase). Between April and July 2020, demand for eviction prevention funding increased from approximately $75,000 per month before COVID-19 to an average of $550,000 per month. 16 Arlington met this need through leveraging new sources of federal and state funding—including federal CARES funding, Virginia's COVID Homelessness Emergency Response program, and Virginia's Rent and Mortgage Relief Program. Each of these funding sources had its own eligibility guidelines and payment caps, which were not always sufficient to prevent eviction. By blending federal, state, and local funds, however, DHS was able to bridge gaps in funding needs with local dollars when federal and state caps were insufficient for impacted residents to pay their full rent each month, and successfully stabilized the majority of households assisted. 16
A survey of over 4,000 US households conducted by Washington University showed that Black and Latinx respondents were more likely to fall behind on rent and utility payments during the pandemic than White respondents, putting them at risk of eviction. 42 The majority of households applying for eviction prevention assistance during the pandemic cited COVID-19-related temporary or permanent job loss as their reason for application. As previously discussed, COVID-19-related job loss was most pronounced among people of color, in particular Black workers and workers of color in direct service-related jobs. Between July 2020 and September 2020, the largest populations served by Arlington's eviction prevention assistance funding were Latinx (49%) and Black (38%).
Isolation Hotels
Isolation hotels (noncongregate shelter) can prevent the spread of COVID-19 among individuals who lack housing or resources to isolate themselves. 43 In Arlington, the number of individuals experiencing unsheltered homelessness increased by 91% during the COVID-19 pandemic between February and May 2020, placing unsheltered individuals at higher risk of contracting the virus. Black individuals experienced the highest increase of unsheltered homelessness at 88%, compared with a 48% increase for White individuals.
In April 2020, Arlington rented 2 hotels to provide isolation space for low-income individuals who lived in overcrowded or congregate settings and were unable to effectively quarantine or isolate. Individuals served were COVID-19 positive, presumed positive, directly exposed, or at high risk of complications due to health conditions. A total of 91 individuals were served across the 2 hotels through May 31, 2020. The demographics of individuals served by the isolation hotels are consistent with those of Arlington's overall unsheltered homeless population (see Supplemental Table 4 (www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041).
Mental Health and Substance Use
The pandemic has negatively affected the lives of many individuals suffering from mental illness and substance use. Research conducted by the Kaiser Family Foundation showed that social restrictions and self-isolation associated with the pandemic increased stress for individuals with preexisting behavioral health challenges due to disturbance of everyday routine, lack of social contact, increased anxiety, job loss, and income insecurity.44,45
Among clients with serious mental illness or substance use diagnoses served by DHS behavioral health programs, there has been an increase in self-harm during the pandemic. The number of suicide attempts increased sharply early in the pandemic: between January and June 2020, suicide attempts increased 157% compared with the same period in 2019 (Figure 5). Opioid overdoses also increased, particularly during the second half of 2020. Among Arlington residents, non-fatal overdoses increased 44%, from 27 individuals in 2019 to 39 in 2020. Fatal overdoses increased from 5 to 11 during the same period, with 72% occurring between July and December 2020 (see Supplemental Figure 1, (www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041).
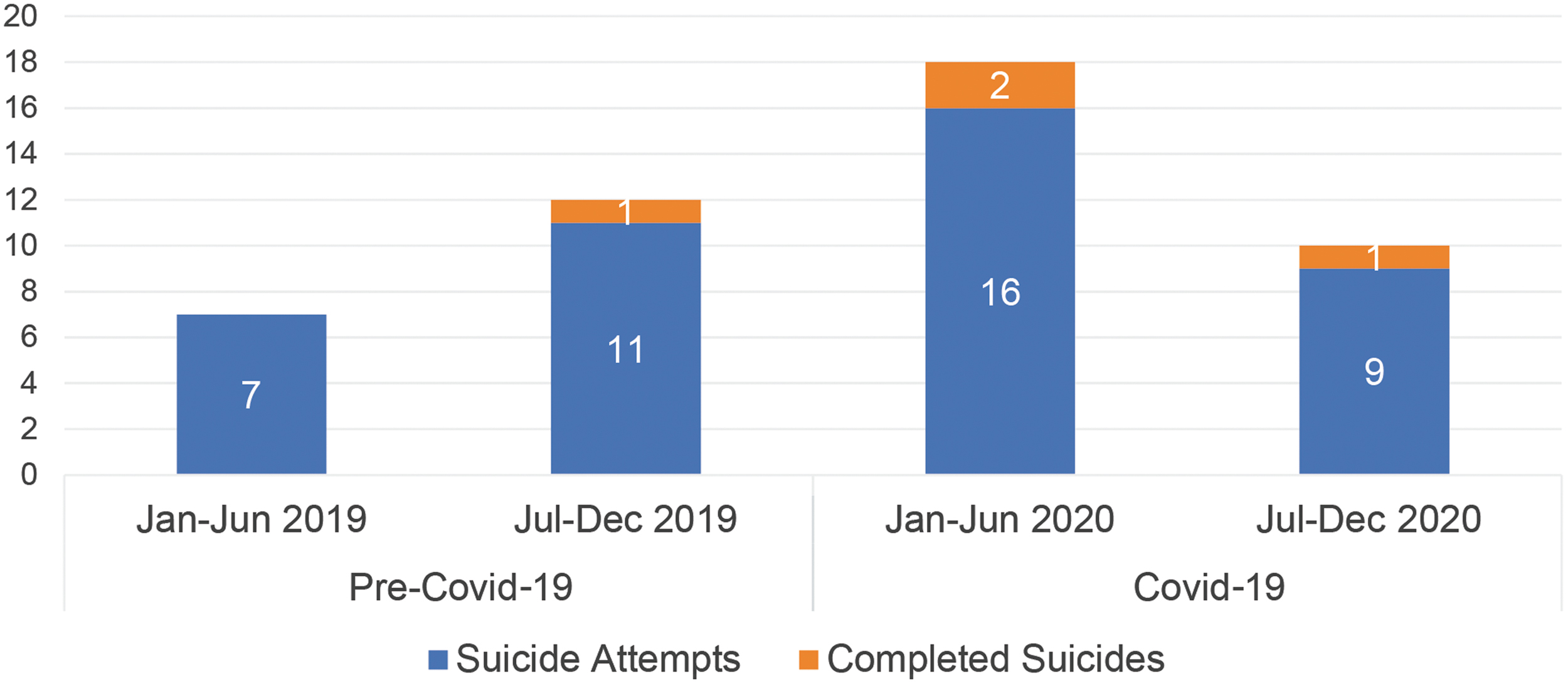
Percentage of suicide attempts and completed suicides among DHS behavioral health clients in Arlington County, January 2019 to December 2020.
DHS clinicians use the Columbia Suicide Severity Rating Scale monthly to monitor behavioral health risk among clients. If a client is determined to have an elevated or acute risk of self-harm, a risk management plan is developed to lower the risk of harm. From April to December 2020, the number of active risk management plans increased by 34% compared with the same period in 2019. The percentage change varied by race—the number of Black clients with risk management plans increased by 85%, the number of clients of other races with plans increased 31%, and the number of White clients with plans remained constant 16 (Table 1). This data suggests that among individuals with preexisting behavioral health vulnerabilities, Black individuals experienced more severe behavioral health impacts during the pandemic.
Number of Behavioral Health Clients Whose Risk Levels Required a Risk Management Plan, 2019-2020
Abbreviation: RMP, risk management plan.
To meet the behavioral health challenges of the community while maintaining safe COVID-19 practices, DHS shifted most case management and therapy services to telehealth in March 2020. Over a 1-week period, Arlington County used an emergency purchasing process to obtain video telehealth software and developed implementation materials including user guides and legal consents. To maximize accessibility for clients, both phone and video services were offered. Telehealth services made up over 40% of the total service hours in 2020. Without the shift to telehealth, many individuals would have been unable to access behavioral health services due to restrictions on in-person service capacity to protect the safety of clients and staff. 16
Telehealth implementation was not without its challenges. Compared with prepandemic service levels, use of telehealth was 15% to 31% lower from March through May 2020. 16 A range of factors affected telehealth effectiveness, including language barriers, regulatory restrictions, and technology and resource limitations. Additionally, some clients expressed concerns about technical issues, privacy, and overall quality of care. Although telehealth increased access for many clients, individuals with lower household income, immigration status concerns, and intellectual disabilities faced additional challenges. 46 To bridge this gap, DHS purchased mobile devices with prepaid minutes that were given to eligible behavioral health clients, including people experiencing homelessness. This effort enabled a greater proportion of clients to stay connected and participate in telehealth services.
As clinicians and clients adapted to the technology, telehealth services enhanced access and outcomes for behavioral health clients. In August, September, and October 2020, service hours returned to levels at or above those delivered in the same months of 201916 (see Supplemental Figure 2, www.liebertpub.com/doi/suppl/10.1089/hs.2021.0041). No-show rates, a key measure of client engagement, improved 41% in 2020 compared with 2019. No-show rates improved most substantially for Black clients. Clients have provided feedback indicating that telehealth removed some barriers to engagement such as the need to obtain transportation to services, take time off from work, and arrange childcare. In addition to improved no-show rates, the rate of psychiatric hospitalization remained stable in 2020. This suggests that, while risk factors for behavioral health clients increased due to the stresses of the pandemic, telehealth services have enabled many clients to address their behavioral health needs.
Digital Equity
Internet access became an essential resource during the pandemic. A lack of internet connection “limits the ability of residents to take advantage of telemedicine services for the sick, telecommuting to prevent layoffs, and distance education for youth.” 47 Additionally, it has been shown that seeing online information about COVID-19 preventive techniques leads to use of those techniques. 48 Demographic analyses of access to the internet show disparities along racial lines, in particular among people with preexisting health conditions. 49
To address digital inequities, the Arlington County government set up over 20 outdoor Wi-Fi hotspots in the community. While indoor spaces such as community centers and libraries already had wireless access, these places were closed due to the pandemic. Wi-Fi hotspots were set up in parking lots where residents could drive up and access online services. Use of these hotspots was high, with over 17,000 monthly users in October and November 2020. In December 2020, several new hotspots were added in high-need areas. These hotspots generated a substantial proportion of total Wi-Fi usage—for example, a hotspot placed in a parking lot near the highest concentration of Arlington's affordable-housing units saw the fourth highest usage of all hotspots in December. The 2 Arlington ZIP codes with the most hotspot usage in December have the highest and third-highest percentages of people of color. 50
Arlington County also partnered with Arlington Public Schools to create a grant program for families with students who qualify for free and reduced meals to access free basic internet service. As of January 2021, 499 families representing over 900 students have participated in the program—approximately 11% of students eligible for free and reduced meals. While this program has not yet met its goal of serving all families with students who receive free and reduced meals, it has been a key resource to previously unconnected families during the pandemic.
Discussion
In Arlington, as in other communities across the nation, the COVID-19 pandemic exacerbated challenges for residents who were already experiencing poverty and systemic racism before the pandemic. The pandemic resulted in poorer health outcomes, decreased economic security, reduced ability to meet basic needs, and increased behavioral health risk factors. To mitigate these impacts, Arlington both repurposed existing resources and leveraged new funding sources and technologies to meet the community's historic and emerging needs.
Many of the interventions first used during the pandemic will continue after the crisis has ended. In addressing the ongoing challenges affecting low-income residents, communities of color, and others disproportionately impacted by the pandemic, Arlington's experience suggests the following approaches:
Repurpose existing resources and adjust staffing to align with postpandemic needs. To address the county's increased food insecurity, Arlington has continued its Cooperative for a Hunger Free Arlington task force and created a new food security coordinator position that will guide the development of food distribution sites in emerging areas of need. Maximize flexibility in tools and procedures. Teleservices opened doors for residents who faced barriers to coming in person to a government agency and streamlined application processes enabled more residents to rapidly access safety net services. Combine funding streams when client needs exceed the limitations of any single funding source. To stabilize households facing eviction, Arlington DHS will continue to assess all available funding sources holistically rather than using a narrow, program-focused view. Rapidly identify disproportionate impacts on the most vulnerable residents. Through timely root cause analysis of serious behavioral health incidents such as overdose and suicide, DHS was able to identify the factors associated with overdose or suicide among behavioral health clients, enabling the system to rapidly target outreach and treatment to clients with similar risk factors. Address digital inequity. During the pandemic, internet access was essential to access healthcare, benefits, education, and information about the pandemic. Arlington's development of outdoor public Wi-Fi hotspots and funding for low-income students provided an important lifeline to digital supports during the pandemic. Commit to addressing racial inequity. Before the pandemic, Arlington had begun to measure and address racial inequity. Due to this work, Arlington leadership had established the capacity to analyze disaggregated data to identify communities who were disproportionately impacted or underrepresented during the pandemic. By being mindful of systemic inequities and targeting services in that direction, Arlington DHS can more effectively meet the needs of the community. Targeting inequity and broadening agency outreach are not contradictory goals. By better meeting the needs of communities of color, DHS will increase the number of people it reaches.
Conclusion
Strengthening resilience and protective factors in communities impacted by systemic racism requires new approaches to policy development, funding, and staff and community engagement. During the COVID-19 pandemic, Arlington DHS identified the communities most impacted by the health and socioeconomic effects of the pandemic, and repurposed resources to meet emerging needs across multiple life domains. This integrated response enabled a holistic approach to the direct and indirect effects of the pandemic, which disproportionately impacted health and economic wellbeing among Arlington's Black and Latinx residents, low-income residents, and vulnerable communities.
Footnotes
Acknowledgments
In addition to the many staff who have been a part of the Arlington County response to the pandemic, we would like to thank our colleagues Talisha Williams and Tiffany Lee for their extensive support and consultation on this project. We would also like to acknowledge contributions from our colleagues Thomas Wallace, Jennifer Plaster, and Sarah Bannister. Their analysis, edits, and ideas strengthened this paper. In addition, we would like to thank the leadership of Arlington DHS for their support of this project.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.