
Abstract
Field simulation exercises (FSXs) require substantial time, resources, and organizational experience to plan and implement and are less commonly undertaken than drills or tabletop exercises. Despite this, FSXs provide an opportunity to test the full scope of operational capacities, including coordination across sectors. From June 11 to 14, 2019, the East African Community Secretariat conducted a cross-border FSX at the Namanga One Stop Border Post between the Republic of Kenya and the United Republic of Tanzania. The World Health Organization Department of Health Security Preparedness was the technical lead responsible for developing and coordinating the exercise. The purpose of the FSX was to assess and further enhance multisectoral outbreak preparedness and response in the East Africa Region, using a One Health approach. Participants included staff from the transport, police and customs, public health, animal health, and food inspection sectors. This was the first FSX of this scale, magnitude, and complexity to be conducted in East Africa for the purpose of strengthening emergency preparedness capacities. The FSX provided an opportunity for individual learning and national capacity strengthening in emergency management and response coordination. In this article, we describe lessons learned and propose recommendations relevant to FSX design, management, and organization to inform future field exercises.
Introduction
Simulation exercises provide an effective means of monitoring, testing, and improving national, regional, and global operational readiness to respond to public health emergencies. 1 With the adoption of the World Health Organization (WHO) International Health Regulations 2005 (IHR), member states agreed to develop, strengthen, and maintain public health core capacities for prevention, detection, and response to health emergencies. This includes response capacities at designated points of entry (eg, ports, airports, ground border posts) as specified in IHR Annex 1, 2 for which specific coordination challenges between countries have to be addressed. Since the IHR monitoring and evaluation framework was implemented in 2016, 3 a mandatory state party self-assessment annual reporting and 3 voluntary components—joint external evaluation, after-action review, and simulation exercises—have been in place. Simulation exercises assess the functionalities of the IHR core capacities, enabling countries to identify preparedness gaps and providing a powerful measure to strengthen national capacities. If countries understand their baseline health capacities, they can be operationally ready to respond confidently when a health emergency occurs, such as the current COVID-19 pandemic. The field simulation exercise (FSX) is an operational exercise, comprising functional exercise elements together with a series of exercise drills. 1
The majority of East African borders are porous and most ground-crossing points are not equipped to detect, prevent, and manage infectious disease as evidenced by previous outbreaks of Rift Valley fever, Marburg virus disease, dengue, and Crimean-Congo hemorrhagic fever.4-9 Cross-border movements are intense across the East African countries due to economic and social activities including migration, livestock breeding practices, trade, tourism, education, job searching, healthcare seeking, and international meetings.10-14
As established by various outbreaks in East Africa and globally (eg, Ebola, COVID-19), the fight against infectious diseases needs a multidisciplinary, whole-of-society approach to be effective. Because 3 in 5 infectious diseases identified in humans are zoonotic, a One Health approach, which is identified as essential for the implementation of the IHR, was adopted for this FSX.13-17
On June 11-14, 2019, the East African Community (EAC) Secretariat conducted a cross-border FSX at the Namanga One Stop Border Post between the Republic of Kenya and the United Republic of Tanzania. This article focuses on lessons learned from the Namanga FSX related to planning, implementation, and evaluation. The authors hope the experiences and lessons learned from this FSX will be useful to other countries and partner organizations considering developing such an exercise. Stakeholders interested in undertaking such a complex exercise may also benefit from the clear methodology, design, and decision process of this FSX experience.
East African Community Decision to Conduct a Field Simulation Exercise
The EAC is the regional intergovernmental organization of Burundi, Kenya, Rwanda, South Sudan, Tanzania, and Uganda, with its headquarters located in Arusha, Tanzania. 18 The EAC has declared the fight against infectious diseases as a health priority for the region. 19 On behalf of the German government, the Deutsche Gesellschaft für Internationale Zusammenarbeit GmbH (GIZ) has been implementing the Support to Pandemic Preparedness in the EAC Region project, which assists the EAC in improving its regional preparedness and response capacity. It contributes to putting the EAC regional contingency plan into practice and implementing the regional risk and crisis communication strategy. 19
At the 11th Ordinary Meeting of the EAC Sectoral Council of Ministers of Health held on March 24, 2015, the council decided that the EAC Secretariat should implement a cross-border FSX at Namanga in Kajiado County, Kenya, and the Longido District in the Arusha Region, Tanzania. 20 This was envisioned as a result of the lessons learned from the West Africa Ebola virus outbreak in which member states were urged to prepare for disease outbreaks and conduct regular simulation exercises to identify preparedness gaps and strengthen their capacities to effectively manage health emergencies. The EAC Sectoral Council urged partner states to establish or strengthen the points of entry health services in line with the One Health approach and based on internationally recommended standards. This directive by the EAC Sectoral Council began the planning of the FSX held in June 2019.19,21
WHO Selected to Lead the Exercise
As part of the WHO Health Emergencies Programme, the Department of Health Security Preparedness focuses on monitoring and evaluating national IHR capacities to support country emergency preparedness as well as planning for and strengthening critical capacities. The department provides essential support to countries in their efforts to assess, monitor, and evaluate the status of IHR implementation including at the animal–human interface. In collaboration with the WHO Regional Office for Africa, the Department of Health Security Preparedness has supported member states in conducting 71 simulation exercises in 27 countries in Africa from 2016 to 2019. 22
Given the expertise of the organization, GIZ contracted WHO as the technical lead to coordinate the planning, design, organization, realization, and evaluation of the exercise, which was convened by the EAC Secretariat and facilitated by GIZ. An exercise of this size required numerous stakeholders and organizations in both the planning and implementation stages. WHO worked with the EAC to plan, implement, evaluate, and report on the simulation exercise for a period of 16 months (May 2018 to August 2019), which involved a series of initial scoping and planning meetings with the Steering Group (SG) and Exercise Management Group (EMG). To commence activities and establish a baseline, the EAC Secretariat conducted a tabletop exercise on September 4 and 5, 2018, in Arusha, Tanzania. 21 The exercise was designed to collect preliminary information from stakeholders that would aid in the design and implementation of the cross-border FSX.
The tabletop exercise demonstrated that some key planning assumptions had not been effectively tested. As such, it was not known if these systems would function in a real situation or during an FSX. For example, there was an assumption that a rapid response team can be deployed at short notice and that the team was clear on their terms of reference and the actions they should take when investigating an outbreak. Undertaking a practical test of this system would enable a validation of this assumption, something that could not be done through a tabletop exercise and that is too complex for a simple drill. Other examples were assumptions of practical measures, such as: (1) people could be effectively screened at the border, (2) health officer training was sufficient for response requirements, and (3) the One Stop Border Post could function as a screening point.
Purpose, Scope, and Objectives
The purpose of the cross-border FSX was to assess and further enhance multisectoral outbreak preparedness and response in the EAC Region using a One Health approach. More specifically, the exercise was designed to:
Test the regional and national contingency plans and standard operating procedures Familiarize participants with the roles and responsibilities of stakeholders from different sectors involved in preparedness, mitigation, and response to a regional public health emergency Assess and identify strengths and weaknesses in coordination and collaboration mechanisms, emergency response deployment, logistics and administrative processes, risk and crisis communication, and emergency management and leadership
As part of the aim to strengthen capacity in the 2 countries, the preparation for the FSX was also designed to train national SG and EMG members in exercise design, planning, and implementation, as facilitators, evaluators, or liaison/safety officers.
The exercise was conducted in a setting as realistic as possible, while the safety of all participants, observers, evaluators, and the general public was ensured through appropriate communication messages to participants and the surrounding community in both countries. It included the deployment of resources, both human and material, required for coordination and response to a public health emergency. The scope was complex, encompassing coordination among regional, national, and subnational levels of government, including the EAC Secretariat and district/subcounty-, regional/county-, and national-level public health emergency operations centers.
The technical objectives of the exercise were to:
Assess the use of early warning and event detection mechanisms, including at points of entry, farms, health facilities, and public health emergency operations centers, with emphasis on the Namanga terrestrial border area between Kenya and Tanzania
Assess coordination mechanisms, command and control systems, and information-sharing channels between multiple sectors and countries
Assess the deployment of rapid response teams
Validate the activation and deployment of 2 mobile laboratories operated by a regional team of 12 laboratory experts from 6 EAC partner states
Assess investigation and management of animal and human cases and functionality of selected veterinary and health facilities in the border area during a large-scale outbreak of a zoonotic disease
Practice regional standard operating procedures for pandemic preparedness, risk management, and crisis communication including community engagement
Evaluate selected preparedness and response measures at the Jomo Kenyatta International Airport and Kilimanjaro International Airport
Capture best practices and ensure transfer of lessons learned to the EAC and other regional economic communities and African regions
Cross-Border and Zoonotic Scenario Used in the Exercise
To promote and practice the One Health approach in the EAC region, an illness with certain similarities to Rift Valley fever, complicated by environmental factors such as rainfall and climate, was selected for the FSX scenario, as its management involves various sectors and professional disciplines. Rift Valley Fever is endemic in the region, with regional outbreak waves about every 8 to 10 years and is therefore a well-known public health threat that countries in the region face. In addition, WHO and the Food and Agriculture Organization of the United Nations (FAO) have a robust experience of multisectoral contingency plans from multiple outbreaks throughout the continent, and the organizations have developed a joint approach to help countries organizing the coordination between the national animal health, human health, and environment authorities through a One Health approach. 23 The WHO and FAO response plan was used to identify the technical areas to test at the human–animal–environment interface. The exercise scenario kicked off with a heavy rain period, which increased the population of vectors and amplification of the Rift Valley fever-like illness. However, to exacerbate the threat and test the operationality of the health sector response, the Rift Valley fever-like illness was presumed also be directly transmitted between humans.
The scenario was implemented in 3 stages:
Event detection: Meteorology, health, and veterinary authorities collect and analyze information from all possible sources including relays on the field, communities, and media
Alert: Real-time monitoring of information and readiness for response in case the situation rapidly deteriorates
Response: Activation of the rapid response teams, which included case investigation, sample collection and testing in farms and health facilities, risk communication community engagement, control and restrictions at points of entry, safety measures at slaughterhouses, communication messages on food safety, and preventive measures related to contact with animals
Detailed scenario outlining the 3 stages can be obtained from the comprehensive exercise report and videos on the Support to Pandemic Preparedness in the EAC Region project website.5,20,21
Development and Management of the Exercise
The planning, design, implementation, evaluation, and reporting of the exercise followed the exercise project management approach described in the 2017 WHO Simulation Exercise Manual. 1 The FSX planning and preparation took over 1.5 years, with the support of many partners and stakeholders either through in-kind or financial contributions. The project was divided into 2 main phases: (1) preexercise planning, material development, and setup; and (2) exercise final preparation, conduct, and postexercise reporting.
Preexercise Planning, Training, Material Development, and Setup
Initial Planning
During the first phase, the following key activities were conducted: exercise site selection, SG and EMG set up, tabletop exercise in September 2018, and 8 planning meetings to develop FSX materials, including a concept note, scenario events, and planning for administrative and logistic needs.
The Namanga border post between Kenya and Tanzania was chosen as the main FSX site, with additional sites selected in each country for field activities. Namanga is near major game parks including the Amboseli National Park, Masai Mara National Reserve, Serengeti National Park, Ngorongoro Conservation Area, and Mount Kilimanjaro, and is therefore a busy tourist point of entry that increases the risk of international spread of disease. For this reason, some activities were conducted in airports, but only sparingly to avoid interrupting their operations.
The setup of the SG and EMG was conducted in accordance with the One Health approach. Overall, 42 SG and EMG members participated in the planning and implementation of the exercise. Members of both groups were national representatives of selected ministries, international organizations (eg, FAO and the World Organisation for Animal Health [OIE]), and representatives of the EAC Secretariat. The following sectors were represented in both groups: human health (33.33%), animal health (19.05%), laboratory (2.38%), intersectoral coordination (40.48%), and points of entry (4.76%). Supplemental Tables 1, 2, 3, and 4 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162) list the SG and EMG members and other partners, including their affiliations and backgrounds, which cover health, agriculture and livestock, environment, trade, tourism and wildlife, security and defense, and the community and media.
Exercise Management Training
The main role of the SG and EMG was to design, plan, and implement the exercise, 1 detailed in the terms of reference included in Supplemental Table 5 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162). Members were nominated from the EAC Secretariat, the countries of Kenya and Tanzania, and international, regional, and local partners. They were required to be available and committed throughout the planning and implementation phases and be willing to learn. Expertise in conducting and implementing simulation exercises and emergency preparedness and response was also preferred. To ensure alignment with the One Health approach, nominators were required to ensure equal distribution of members according to disciplines relevant to the FSX. Both groups were established and mandated during the EAC Simulation Exercise Stakeholder Meeting held on July 12-13, 2018, at the EAC headquarters in Arusha.19,21
A total of 18 SG and 17 EMG members were trained at the Windsor Golf Hotel and Country Club, Nairobi, Kenya, on April 8-12, 2019. WHO experts trained members on exercise management skills as part of the initial planning meetings.19,21 By the end of the FSX, the number of SG and EMG members increased from the initial 35 members to 42 members to accommodate additional needs for expertise, experience, and familiarity with the local context to better guide the FSX.
During the training, members learned exercise management skills, including how to implement exercises smoothly. In particular, members received training on their role as facilitator, evaluator, or liaison/safety officer at the various exercise sites. The training was critical for ensuring national ownership of the FSX and strengthening national exercise management capacity.
Resource Mobilization
The SG was tasked with resource mobilization, including identifying and mobilizing national and partner resources for in-kind support or technical support. They developed terms of reference for partner engagement, which included the use of logos and visibility material for each partner. In addition to engaging national-level ministries, the GIZ project mobilized 17 partners in cooperation with WHO, as presented in Supplemental Table 2(www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162).
Field Visits
The SG and EMG conducted 6 field visits to establish resources, facilities, and sites for use during the exercise. The field visits improved understanding of local exercise site requirements and needs and helped increase support and awareness among local leaders and the communities. The field visits included training for those involved in the exercise (role players/actors), sensitization of stakeholders (leaders and participants) about the purpose and objectives of the exercise, clarification on roles and responsibilities, and community meetings that highlighted the benefits of the exercise to communities. Permission was requested for filming and photographing of the exercise and the use of the One Stop Border Post; using community resources, such as farms and animals; and engaging community members as actors or role players for the exercise. The SG and EMG conducted a rehearsal to familiarize members with the materials and sites.
Exercise Final Preparation, Conduct, and Postexercise Reporting
Participant Preparation
Approximately 300 people were involved in the exercise, either as participants (players), actors/role-players, controllers/facilitators, evaluators, or observers. A total of 189 FSX participants were actively engaged during the 3 days of the exercise, including 87 participants from Kenya, 83 from Tanzania, 11 from the EAC Secretariat, and 8 from the Mobile Laboratory Team from other EAC countries (ie, Burundi, Rwanda, South Sudan, Uganda). Because the exercise adopted a One Health approach, participants represented a wide variety of sectors and government ministries including animal health (23.81%), human health (46.03%), laboratory (9.52%), points of entry (7.41%), and coordination with other sectors (13.23%), as presented in Supplemental Table 6 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162).
Participants were nominated by local authorities based on the objectives of the FSX and their respective professional functions and roles rather than as individuals. They were expected to perform their daily functions and tasks during the exercise as they would perform them during a real emergency response. To familiarize the SG, EMG, evaluators, and actors on the key aspects and roles they would play during the exercise, briefing sessions were conducted 2 days before the exercise (June 8-9, 2019). Guided by WHO simulation exercise mentors, the EMG, SG, and exercise role players reviewed and practiced their actions and roles using a master sequence events list and scripts. Before the exercise began on June 11, 2019, the exercise coordinator provided a briefing for all participants and observers on several aspects of the exercise, which was supplemented by participant and observer guides distributed 2 weeks before the exercise.
Exercise Conduct
The exercise was conducted over 3 days at 23 different sites located in both countries. Most of the exercise sites were located within a 25 km radius of the exercise control site at Namanga, where all planning and operations of the exercise were coordinated; the remaining sites were substantially farther away, including Dodoma (528 km), Arusha (114 km), Kilimanjaro International Airport (159 km), Jomo Kenyatta International Airport (155 km), Nairobi (164 km), and Kajiado (87 km). A map of key locations is presented in Figure 1 and a list of the exercise sites is provided in Supplemental Table 7(www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162).
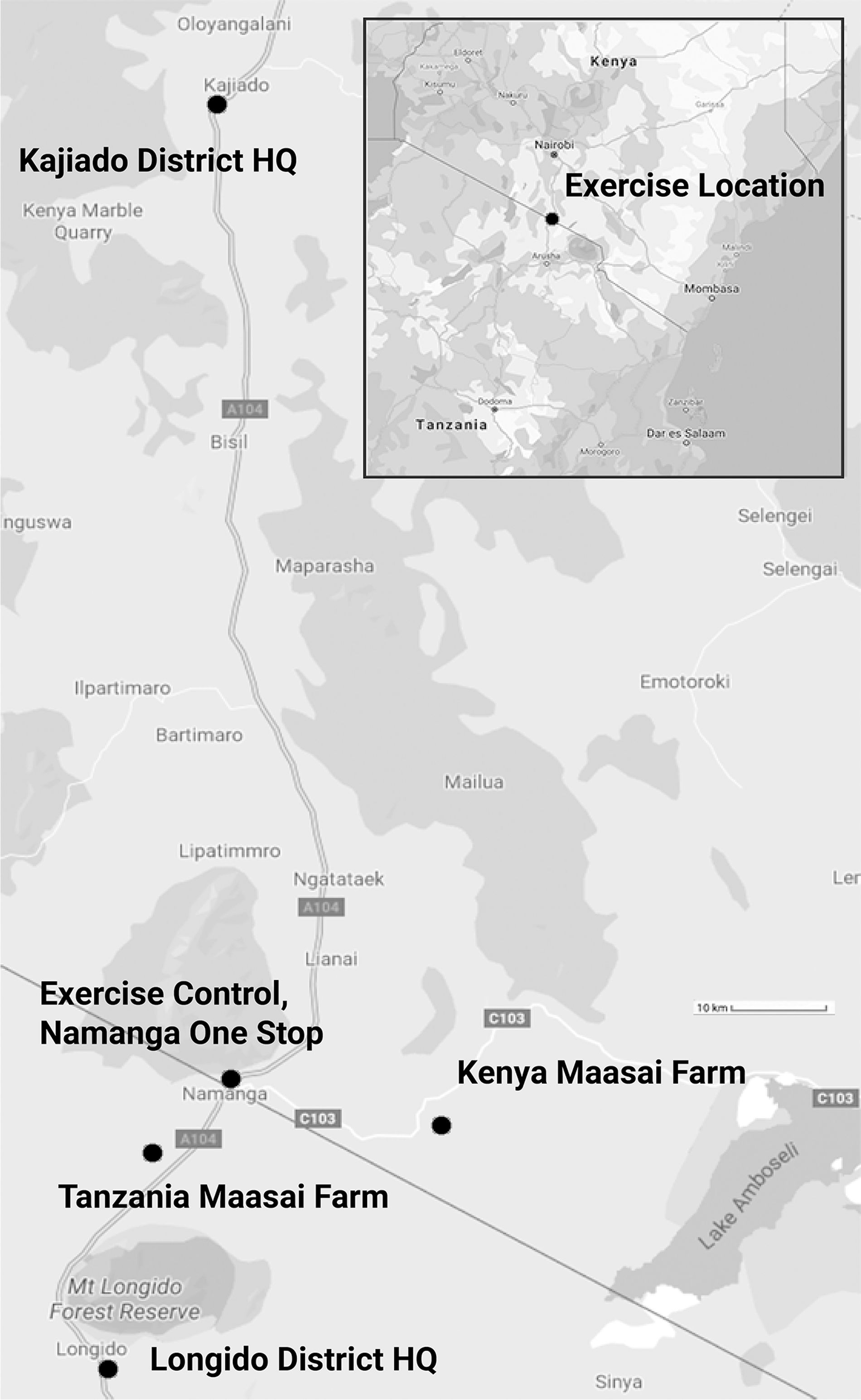
Map of key locations used in the Kenya and Tanzania cross-border field simulation exercise. Abbreviation: HQ, headquarters.
Due to the complexity of the exercise, number of locations, and distances between locations, the EMG and logistics partners, especially the United States Defense Threat Reduction Agency, developed a detailed movement plan for air and road transportation to move participants, the SG, the EMG, evaluators, and observers across the 2 countries. Because of limited communication system capacities in the Namanga area, WHO installed a 2-way radio system to enable teams to communicate in remote parts, especially farms. Namanga is a small town with few service providers, and therefore most of the services, such as bulk printing services, filming, and video crew, were procured from Arusha, Dar es Salaam, and Nairobi.
The exercise coordinator was located at the exercise control site at the Namanga One Stop Border Post, on the Kenyan side. National facilitators and evaluators, reporting to the lead controller, were located at the various exercise sites. Exercise locations and staffing are shown in Supplemental Table 7. A master sequence events list (or “inject matrix”) drove the exercise. It included a description of all simulated events to be injected into exercise play (exercise “injects”) and the expected actions resulting from them. Injects were designed to simulate an outbreak as realistically as possible and to facilitate responses or outputs in line with the objectives defined for the exercise. Figure 2 shows an overview of how the exercise was conducted over 3 days, followed by an additional day for debriefing.
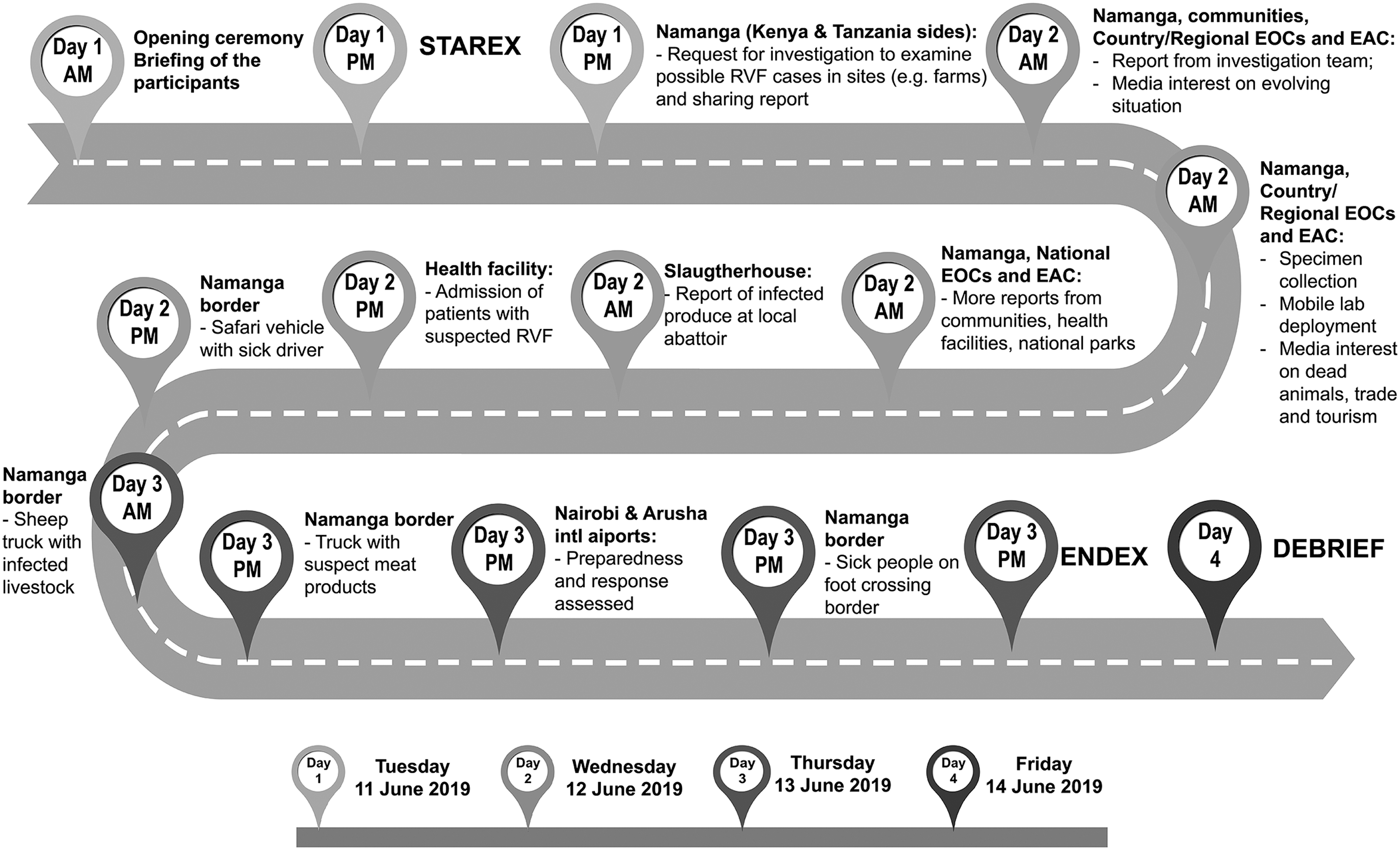
Key milestones from the Kenya and Tanzania cross-border field simulation exercise. Abbreviations: EAC, East African Community; ENDEX, end of exercise; EOC, emergency operation center; Intl, international; RVF, Rift Valley fever; STAREX, start of exercise.
Onsite Participant Debriefing
Directly after the day's activities at any site, the onsite facilitator held a debriefing, or hot wash, to gather immediate feedback from all participants on strengths and weaknesses of the response while the event was still fresh in their minds. This information, together with the completed exercise evaluations forms, was returned to the exercise evaluator for further analysis.
Offsite Participant Debriefing
An offsite participant debriefing was conducted in Longido, Tanzania, on June 14, 2019, to enable participants to provide feedback on the FSX both in terms of fulfilling its objectives and overall organization.
Due to the large number of participants and limited time, the debriefing was organized using the World Café methodology, a structured conversational process for knowledge sharing developed by the World Café Community Foundation. 24 The methodology was adapted to assist participants to identify the most significant strengths and weaknesses revealed by the exercise. Emphasis was placed on the ability of the EAC Secretariat and the 2 partner states to operate together and launch an effective response to a disease outbreak. Participants were organized into 2 groups of 4 tables, each of which represented specific functional areas and partner states or entities from the exercise. Each group was asked to post on a flip chart what they considered to be the 5 most substantial achievements or strengths observed during the exercise response and the 5 most substantial challenges or weaknesses. Detailed results from the debriefing can be found under Annex D in the final FSX report. 25
Participants were also asked to participate in a survey on the design, organization, and conduct of the exercise using an electronic voting system. Full results of the survey are shown in Table 1, confirming a high level of appreciation for the exercise and the relevance and value of this exercise in strengthening emergency preparedness and response. We received positive feedback from participants, which we believe is linked to the continuous engagement and sensitization of participants prior to the exercise.
Results of Participant Survey, Longido, Tanzania, June 14, 2019 (N = 121)
SG and EMG Debriefing
The SG and EMG assessed the exercise planning, management, and organization, including the SG and EMG structure and performance, at a final meeting and debriefing held at the Kibo Palace Hotel in Arusha, on June 17-18, 2019. While the outcome was mostly positive, it was noted that the roles of the 2 groups were not always clear, resulting in delays during the planning phase. We hypothesize that the overall positive feedback can be attributed to the extensive training and mentorship conducted by WHO prior to the exercise, which may have increased confidence among organizers to administer the exercise. Full results of the survey conducted at the end of the SG and EMG debriefing can be found in Table 2.
Results of SG and EMG Survey, Arusha, Tanzania, June 17-18, 2019 (N = 21)
Abbreviations: EMG, Exercise Management Group; FSX, field simulation exercise, SG, Steering Group; TOR, terms of reference.
Internal WHO Evaluation
An internal WHO exercise evaluation was conducted during and after the exercise to determine whether the exercise achieved its original objective of assessing the efficiency of the preparedness and response systems in Kenya and Tanzania. Using the recording of actions during the exercise, the evaluation identified both the achievements and challenges of the exercise with respect to the relevant policies, plans, and procedures of the 2 countries and the EAC Secretariat.
The evaluation scoring system was qualitative, using a 4-point system: performed without challenges, performed with some challenges, performed with major challenges, or unable to perform. Each evaluator was a subject matter expert who had agreed to a set of criteria to evaluate each part of the exercise. The exercise was designed with a series of measurable tasks in mind, which was reflected in the evaluation. An example of the exercise evaluation form used by evaluators can be found under Annex C in the FSX report. 25
The evaluation was based on the collective performance of participants, rather than individuals. The evaluation sought to assess:
Whether the exercise achieved its objectives
What joint response strengths should be built upon
What operating procedures, protocols, and guidelines improvements were needed
What improvements in coordination of management systems were needed
What operational equipment was needed
What additional training and exercises should be required
Postexercise Reporting and Handover
The exercise project was completed in August 2019 and all narrative and financial reports were handed over to relevant EAC, GIZ, and WHO offices. The evaluation technical lead, with support from other WHO experts, prepared the final FSX report and shared it widely. 25
Lessons Learned and Key Recommendations
Four key lessons learned emerged from the planning, design, implementation, evaluation, and reporting of this cross-border FSX. Here, we summarize the lessons learned and recommendations.
Lesson 1: WHO exercise project management approach was effective
The planning, design, implementation, evaluation, and reporting of the exercise followed the WHO exercise project management approach, which was a clear and effective process for managing such a complex and large exercise project. This structured process helped in defining the specific exercise purpose, scope, and objectives needed for large and complex exercises. In addition, it helped identify and define different roles and responsibilities of the various stakeholders and partners required. Furthermore, the time and resource needs were clearly divided into 2 main phases: (1) preexercise planning, material development, and setup; and (2) exercise final preparation, conduct, and postexercise reporting.
The tabletop exercise conducted before the FSX provided an effective base to collect information that supported the design of the complex exercise 9 months later. WHO recommends that member states have progressive exercise programs, starting with simpler exercises, such as tabletop exercises, and then moving to more complex operational exercises, such as drills, functional exercises, and eventually FSXs. 1
Lesson 2: Partnering with stakeholders was essential
Engaging with partners and other stakeholders at all stages, from planning to implementation, was paramount to effectively implementing the FSX. Partnership, commitment, and collaboration are vital to the success of any response, as indicated in various emergency response reports. Partners were selected based on the comparative advantages they brought to a successful FSX, in addition to their possible support in terms of financial or technical expertise. Broad selection and representation of various sectors in the EMG and SG were essential to ensure a realistic exercise scenario and balanced participation of exercise participants, aligned with the One Health approach. This includes members representing health, agriculture and livestock, environment, trade, tourism and wildlife, security and defense, and the community and media, from national ministries, international organizations, and representatives of the EAC Secretariat; see Supplemental Tables 1, 2, 3, and 4 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162).
With multiple sectors and stakeholders involved in the FSX, conflicts of interest and competing expectations introduced challenges. Planning meetings were essential at the beginning of the process to establish a clear and shared agreement on the purpose, scope, and objectives of the exercise. Selecting appropriate partners, defining their roles and responsibilities, and actively engaging with them through regular meetings on progress against targets are critical to ensuring the effective implementation of a complex FSX.
The FSX was unique in its scope, complexity, and magnitude, and therefore political buy-in from the EAC, the countries of Kenya and Tanzania, and relevant stakeholders and partners was vital. As the owner of the exercise, the EAC Secretariat ensured that national and political commitment was achieved and that national emergency preparedness and response capacities among its member countries were strengthened. The EAC's ownership also ensured that a follow-up mechanism was in place for actions identified from the exercise and provided an opportunity for the EAC to use the knowledge and skills gained to support planning and implementation of future exercises within the East Africa region. This is a good example of leveraging regional entities for synergistic capacity strengthening for health security.
The EAC, GIZ, and WHO engaged a total of 17 partners in the planning and implementation of the exercise, including FAO and OIE, that were crucial to ensuring the One Health approach was not lost; a list of partners is presented in Supplemental Tables 1, 2, and 3 (www.liebertpub.com/doi/suppl/10.1089/hs.2020.0162). To ensure success and accountability, partners discussed and agreed upon clear terms of reference and all stakeholders participated in monthly meetings and sensitization meetings. Meetings also provided a forum for updating members on tasks assigned, such as resource mobilization, advocacy with senior management, logistics planning, and development of simulation materials. 21 As a result, funds and in-kind donations for FSX were mobilized successfully, including logistical support, which are crucial because substantial capacity is needed to run the exercise smoothly. Feedback during the evaluation indicated the need for a simulation exercise to have a few objectives and a simple exercise management structure for more efficient planning and implementation.
Communities and media companies are key stakeholders in emergency management. The success of the FSX was centered on good engagement and preparation of communities. A series of sensitization meetings with communities (eg, livestock keepers, local leaders, local traders), media companies, joint border management committees, and various organizations across the 2 countries proved to be a good investment and led to the acceptance of the FSX, commitment by the communities and organizations, and prevention of raising false alarm or rumors during exercise. These activities/actions led to high community participation, commitment, and access to sites. All stakeholders were also involved in FSX roles such as actors/role-players and participants. However, the high number of observers and external partners present in the FSX led to crowd control challenges; future exercises should limit number of observers.
Lesson 3: Engaging national experts ensured capacity strengthening and ownership
The WHO Department of Health Security and Preparedness has been training simulation focal points from member states' ministries of health and WHO country offices for several years, which has led to a steady increase in the number of exercises conducted in the region. At the inception of this exercise project, there was need to develop a group of experts in the EAC who could plan, design, and implement exercises of this magnitude.
To enhance sustainability of exercise programs in the member states, WHO embarked on an initiative to actively engage, develop, and mentor focal points from member states to strengthen their capacity to run such complex activities on their own. 22 Capacity strengthening initiatives and the selection of national technical experts as SG and EMG members was beneficial to the EAC and to member states. Prior training and mentorship experience as well as additional training and practice with simple drills helped members conduct their roles effectively during the main FSX. The combination of guidance and training, multinational and international interactions, exercise experience, and mentorship were essential to further strengthening national capacity to run complex operational exercises.
WHO guided Kenya and Tanzania in selecting the 42 multisectoral experts, who were trained using WHO simulation exercise methodology as described in the WHO Simulation Exercise Manual and exercise training documents.1,20 WHO held a series of planning meetings over 11 months in the 2 countries to actively mentor the SG and EMG to plan and design the exercise story line, master sequence events list, and injects and to organize required complex logistics including sensitization and awareness meetings at the FSX sites. To ensure the team used the skills and knowledge acquired during the project, SG and EMG members were assigned key roles and responsibilities at all 23 exercise sites. To strengthen capacity in their respective exercise management roles, WHO assigned each SG and EMG member an expert advisor to provide advice, mentorship, and support during the exercise. As a result of the success attained by this capacity strengthening initiative, the Tanzania SG and EMG members were involved in developing and implementing an Ebola exercise program from August to December 2019 in Tanzania. The methodology and key lessons learned during the June 2019 exercise will be used to organize future EAC Secretariat exercises. The EAC invited the Namanga FSX SG and EMG members to Entebbe, Uganda, on February 4-8, 2020, to share their experiences with a new EMG tasked with planning a cross-border FSX between South Sudan and Uganda.
The exercise proved to be an excellent opportunity to strengthen emergency preparedness and response capacity in Kenya and Tanzania. It revealed specific strengths and weaknesses, which resulted in 19 concrete recommendations, including recommendations related to One Health coordination mechanisms, command and control systems, and information sharing, which are detailed in the exercise report. 25 The FSX was intended to also to expose participants to a realistic scenario, enabling them to practice the roles they would carry out in a real emergency—such as the current COVID-19 pandemic, where the One Health approach has proved to be paramount. The exercise increased awareness of the benefits of exercises to enable staff to practice in their response roles; validate policies, plans, and procedures; and strengthen interoperability of public health systems and their state of preparedness. Because the exercise included many different organizations that do not work together on a regular basis, participants had an opportunity to network and improve their understanding of each other's roles and responsibilities, which is essential in a real emergency.
Identifying strengths and weaknesses can be achieved through methods that are not as costly as FSX, but the FSX has the advantage of high-level visibility, which often enables senior decision makers to engage with issues that might otherwise not come to their attention through less visible exercises (eg, tabletop exercises).
Lesson 4: Postexercise action plans are critical but challenging
Implementing postexercise findings and recommendations remains a key challenge. Following the FSX, a road map was developed to guide implementation and monitoring of the recommendations in the region to ensure further strengthening of the emergency preparedness and response capacity and support sustainability. WHO and other partners also supported Tanzania to develop and implement an Ebola exercise program, including tabletop exercises and drills, between August and December 2019. Key gaps observed from the Ebola exercises in Tanzania were addressed by the government in collaboration with partners. National capacity strengthening in exercise management was critical; the EAC has adapted this strategy to train and strengthen the capacity of all future EMGs that plan and implement FSXs.
Conclusion
The COVID-19 pandemic has tested and stressed national health systems throughout the world. Many critical skills tested in the Namanga FSX—including identification, isolation, and management of cases; multisectoral collaboration; risk communication; and community engagement—are being used in Kenya and Tanzania as part of their national response to the current pandemic.
Involving national experts throughout the exercise project resulted in both strengthened local simulation exercise capacity and national ownership, which ensured that exercise findings and recommendations were implemented and monitored. The exercise evaluation and individual feedback found that participants improved their knowledge, skills, and understanding of existing national emergency response systems and structures. At the same time, organizations benefitted by, for example, clarifying roles and responsibilities within and between different agencies and organizations and testing existing coordination mechanisms.
FSXs are complex and resource intensive, and this cross-border FSX was no exception. It required expert partner involvement, more than a year of planning, and substantial funding requirements. These exercises can enhance overall preparedness and response capacity when they are properly designed, managed, and implemented using an exercise project management approach with a clearly defined purpose, scope, and objectives. As FSX are resource intensive and require expert involvement, they should be used to address the most critical potential events and should be planned and conducted as part of a broader exercise program to maximize their benefit and value.
Countries need to enhance their preparedness and response capacities and put resources in place. We recommend that countries undertake simulation exercises regularly to prevent outbreaks of diseases that can jeopardize public health, economic stability, and the lives and livelihoods of people in their countries and regions, as observed during the COVID-19 pandemic. Simulation exercises offer a unique opportunity for countries to enhance their capacity to respond to infectious disease outbreaks of both human and animal origin.
Footnotes
Acknowledgments
Almost 300 people participated in the cross-border FSX, with the majority from EAC partner states Kenya and Tanzania. In addition, representatives from the EAC Secretariat, EAC partner states Burundi, Rwanda, South Sudan, and Uganda, and the southern African states of Lesotho, Malawi, Mozambique, and Zambia participated in the FSX. The EAC Secretariat, GIZ, and WHO would like to thank all those who contributed their valuable time and resources in ensuring the success of the exercise project, namely the Namanga community, Namanga Joint Border Management committee, SG and EMG members (a complete list of ministries and departments is provided in Supplemental Table 3 and a list of members is detailed in Supplemental Table 1), EAC Secretariat Mobile Laboratories Rapid Regional Response Team (see Supplemental Table 1), and partners, especially the US Defense Threat Reduction Agency (listed in Supplemental Table 2), among others. The supplemental tables can be accessed at ![]() .
.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.