
Abstract
On May 12, 2017, the Democratic Republic of Congo (DRC) publicly declared an outbreak of Ebola virus disease (EVD) in the Likati District of the Bas-Uélé Province, 46 days after the index case became symptomatic. The delayed EVD case detection and reporting highlights the importance of establishing real-time surveillance, consistent with the Global Health Security Agenda. We describe lessons learned from implementing improved EVD case detection and reporting strategies at the outbreak epicenter and make recommendations for future response efforts. The strategies included daily coordination meetings to enhance effective and efficient outbreak response activities, assessment and adaptation of case definitions and reporting tools, establishment of a community alert system using context-appropriate technology, training facility and community health workers on adapted case definitions and reporting procedures, development of context-specific plans for outbreak data management, and strengthened operational support for communications and information-sharing networks. Post-outbreak, surveillance officials should preemptively plan for the next outbreak by developing emergency response plans, evaluating the case definitions and reporting tools used, retraining on revised case definitions, and developing responsive strategies for overcoming telecommunications and technology challenges. The ongoing EVD outbreak in the North Kivu and Ituri provinces of DRC, currently the second largest EVD outbreak in history, demonstrates that documentation of successful context-specific strategies and tools are needed to combat the next outbreak. The lessons learned from the rapid containment of the EVD outbreak in Likati can be applied to the DRC and other rural low-resource settings to ensure readiness for future zoonotic disease outbreaks.
On May 12, 2017,
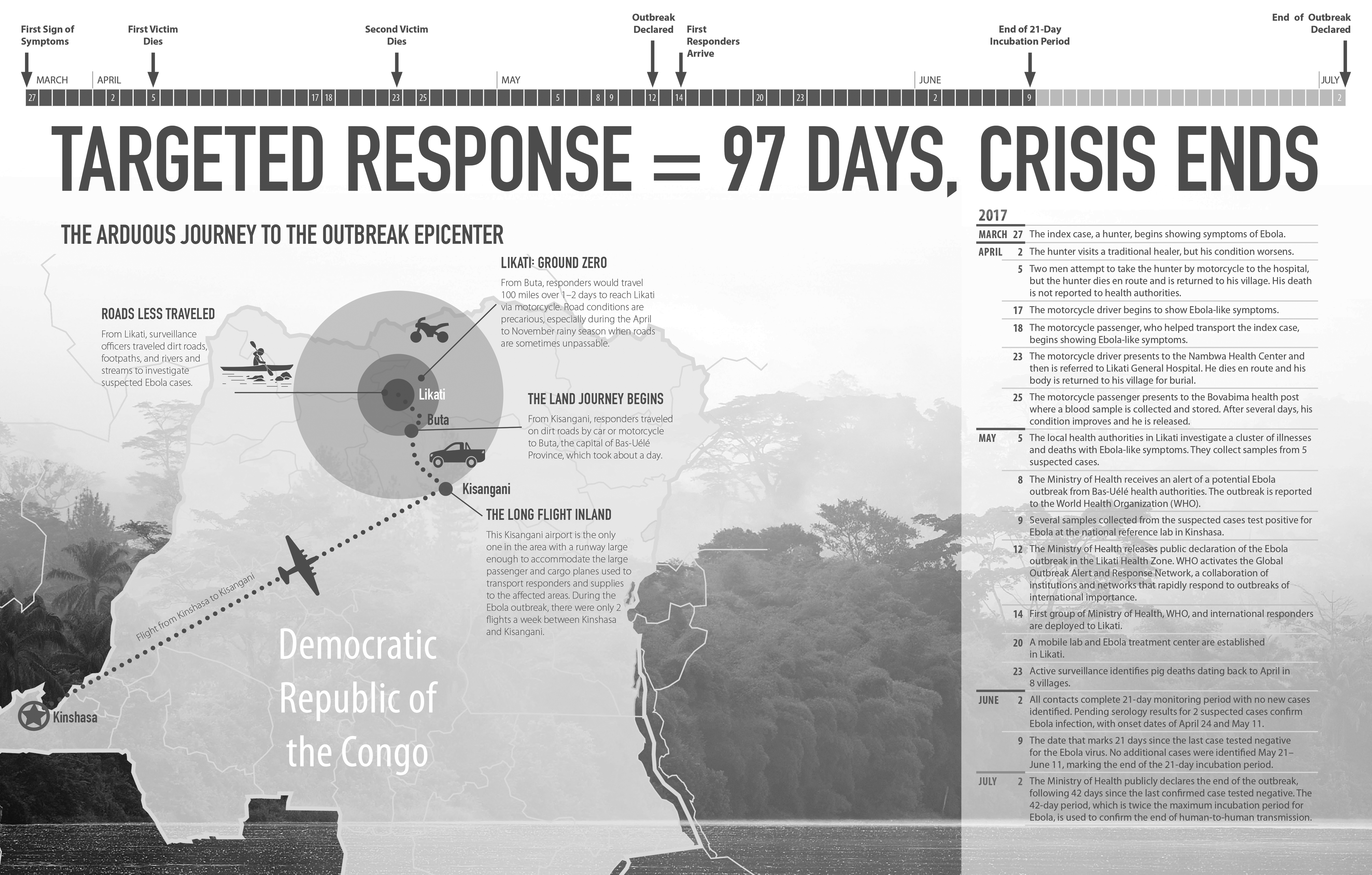
Targeted Response: Map and Timeline of the Ebola Outbreak in Likati District, DRC, March to July 2017
The occurrence of 3 EVD outbreaks in less than 18 months points to an urgent need for proven strategies that can be adapted to future outbreaks in similar settings and leveraged for preemptive outbreak response. The Global Health Security Agenda provides a framework for strengthening both global and individual nations' capacity to prevent, detect, and respond to infectious disease threats. This multilateral and multisectoral agenda focuses efforts for countries to achieve compliance with the International Health Regulations (IHR), an agreement among all World Health Organization (WHO) member states. The IHR provide a common understanding of global expectations to mitigate potential public health threats.9,10 A systematic review of lessons learned from implementation of IHR core capacities found very little documentation of applicable lessons for Africa and none in the DRC. 11
In response to this knowledge gap, we draw from our experience supporting the Likati EVD outbreak response to describe the specific surveillance and investigation strategies that contributed to rapidly containing the outbreak within 51 days of the public declaration. 2 To meet the growing need for proactive plans to address emerging infectious disease threats,12,13 we document lessons learned and practical recommendations to help policymakers and first responders prepare for future zoonotic disease outbreaks in the DRC and similar resource-limited rural settings. Further, we aim to advance the goals of the Global Health Security Agenda by describing how these recommendations can prevent avoidable epidemics, detect threats early, and enable a rapid and effective response to infectious disease outbreaks.
Materials and Methods
Background, Location, and Population
The DRC is an epicenter for emerging zoonotic diseases and is considered one of the most vulnerable countries in the world for disease outbreak. 14 Its tropical ecosystem is favorable to zoonotic disease development, with well-documented emergence and reemergence of infectious disease pathogens.15-20 Many people rely on bushmeat as a source of food and income, contributing to a high risk of zoonotic spillover by putting humans in direct contact with wildlife, the main reservoir for emerging infectious diseases such as EVD, other viral hemorrhagic fevers, and monkeypox.15-17,20 Bushmeat was identified as the source of the Likati outbreak, with evidence that the index case was infected in a spillover event from contact with a carcass from a wild boar or nonhuman primate. 2
The Likati district is heavily forested and largely rural, with a population of 70,858 and 6 inhabitants per square kilometer. The economy is based primarily on agriculture, fishing, and hunting, resulting in a highly mobile population, which increases risk of exposure to zoonotic threats and presents challenges for breaking chains of transmission. Health activities in the Likati district are managed by ministry of health staff at the district health office in the town of Likati, with additional oversight and support from the provincial health office in the provincial capital of Buta, approximately 100 miles away. Health services are provided at the general reference hospital in the town of Likati and 11 health centers, each with a distinct geographical catchment zone called a “health area.” The Likati district lacks essential health infrastructure, with many people seeking care outside of the formal health structure. At the outbreak onset, the ministry of health reported that 50% of the population had health coverage and 60% could access the minimum package of public health services. At the health-center level, there were no health workers with post-baccalaureate education, and tools and equipment were insufficient for primary care provision and disease surveillance. 7 These common infrastructure deficiencies, identified in previous EVD outbreaks, 13 likely contribute to delays in detecting and reporting unusual health events.
Outbreak Response
Within 48 hours of the outbreak declaration, the DRC government mobilized a team of experts and enacted a comprehensive response plan to define the critical activities, coordination structure, and required resources to rapidly and effectively contain the outbreak. 8 The National Coordination Committee, based in Kinshasa, managed central response activities and provided support to the rapid response teams in Likati. Response activities were organized into 7 pillars: (1) surveillance and investigation, (2) medical management, (3) water/hygiene, (4) laboratory and research, (5) psychosocial support, (6) communication and social mobilization, and (7) logistics. Rapid response teams, composed of more than 30 experts from government and international agencies, were assembled for each response pillar and deployed to the epicenter to implement targeted activities. Daily coordination meetings were held in Kinshasa and Likati to monitor and adapt to the outbreak's evolving needs.
The surveillance team was led by the Ministry of Health's Division of Disease Control (Direction de Lutte contre la Maladie, or DLM), with support from field epidemiologists and information and communication technology specialists from RTI International, Médecins Sans Frontières, and WHO. Primary tasks included: (1) identifying the outbreak origin and chain of transmission; (2) collaborating with local health workers to detect and actively investigate reported cases and implement procedures for contact tracing and monitoring; (3) managing case, contact, and alert data; and (4) compiling and disseminating daily situation reports. We provide lessons learned during the support of these surveillance activities, drawing from the collection and analysis of outbreak surveillance data, direct observation, development of training materials, implementation of procedures for case detection and contact tracing, and documentation of the epidemiologic investigation.
Surveillance Methods
During the outbreak, the surveillance team investigated a total of 106 suspected cases and 583 contacts to trace the chain of transmission and identify the outbreak origin. They visited remote villages throughout the district to interview cases, contacts, health workers, and community members; review health records; investigate unexplained deaths and illness in humans and animals; and look for evidence of animal-to-human transmission.
Suspected cases were detected through active surveillance at health facilities and in the community, contact tracing activities, community-initiated alerts, and reports from other pillars. To support active case finding, facility-based health workers were trained on the outbreak-specific definitions for suspected, probable, and confirmed cases. When a suspected case was identified, a surveillance team member traveled to the reported location and, together with the local health worker, completed the case notification form and collected specimens for laboratory diagnosis. This provided epidemiologic and clinical data to assess and classify each case as suspected, probable, confirmed, or non-case, according to the outbreak-specific case definitions. By directly engaging health workers in case investigation activities, the surveillance team reinforced local capacity to document, manage, and report suspected cases in line with ministry of health surveillance guidelines.
To reinforce case ascertainment, the surveillance team also established a community alert system, which was publicized during community awareness campaigns and investigative activities (Figure 2). Alerts were investigated within 24 hours of receipt, classified as a suspected or non-case, and documented on the appropriate reporting form.
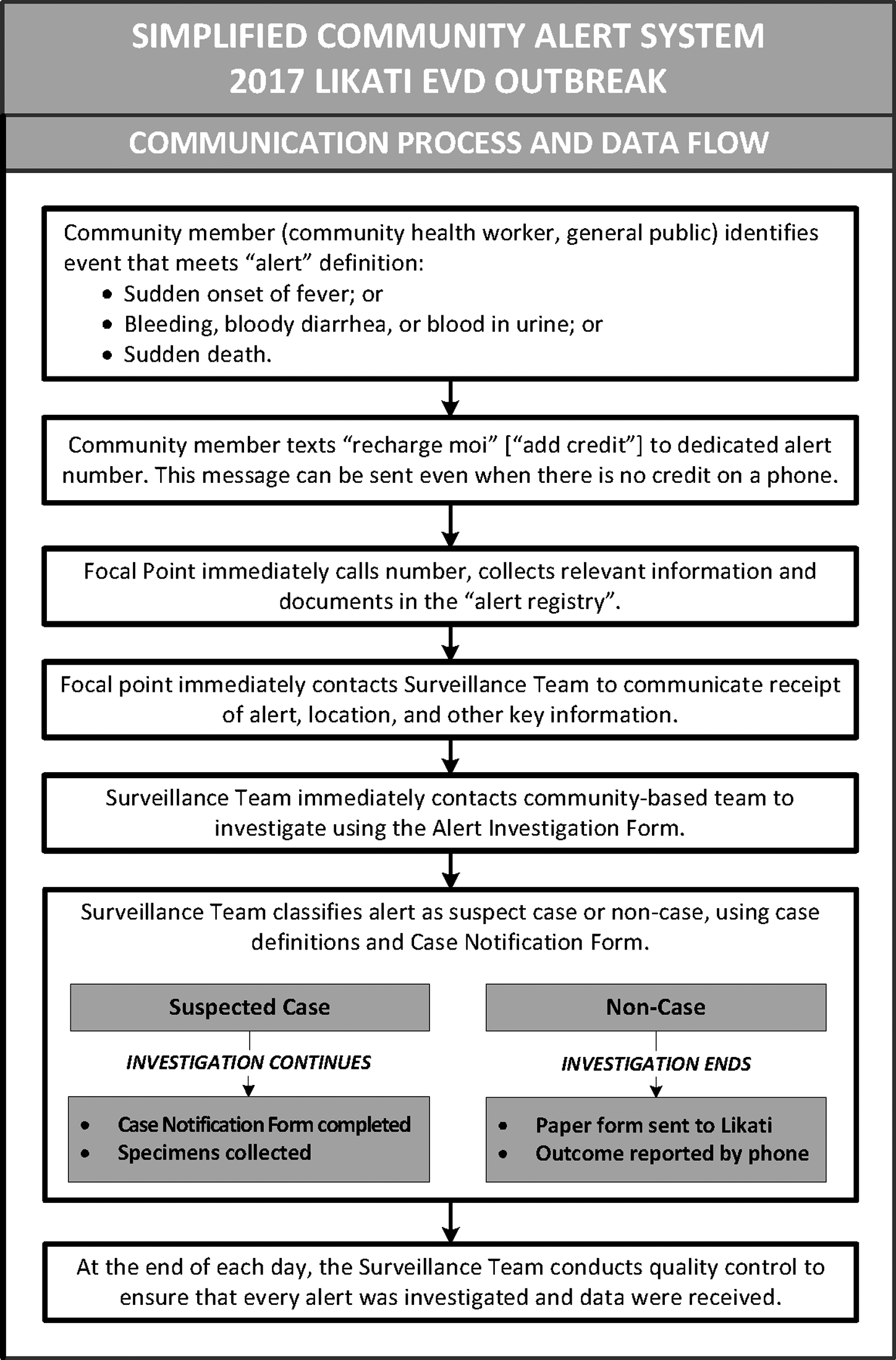
Communication Process and Data Flow for the Community Alert System Used During the Ebola Outbreak in Likati District, DRC, March to July 2017
Community health workers supported case finding and contact monitoring activities. To improve detection of suspected cases by community health workers, a community case definition was developed by broadening the standard EVD case definition to include: (1) any person with sudden onset of fever, OR (2) any person with bleeding, bloody diarrhea, or blood in urine, OR (3) any sudden death. The purpose of the broadened case definition was to facilitate ascertainment of all illnesses or deaths potentially attributable to EVD for further investigation.
The surveillance team used participatory methods to train 98 community health workers on the community case definition, EVD signs and symptoms, case reporting procedures, and contact monitoring procedures. All contacts were monitored by community health workers for 21 days, using a standardized contact tracing form. A member of the surveillance team also visited the contact during the monitoring period to capture geolocation using an Android-based application. At each health center, the head nurse was responsible for daily reports by phone to the response headquarters on the number of contacts being monitored and exiting 21-day follow-up. If EVD signs or symptoms were reported during contact monitoring, the head nurse immediately notified the surveillance team by phone so that an active case investigation could be initiated.
All case and alert data were collected on paper forms and sent to the Likati response headquarters for centralized data entry, with essential information sent by text message or reported verbally by phone while the paper forms were en route. For contacts, only paper records from the first contact interview were sent to the Likati response headquarters for centralized data entry; data for the remaining follow-up period (eg, temperature tracking) were maintained only on paper due to limited data entry personnel. Data were managed in Excel and the viral hemorrhagic fever case management system, an open-source software tool developed by the Centers for Disease Control and Prevention (CDC) to manage case and contact data during outbreaks. 21 The surveillance team compiled all case, alert, and contact data and produced a daily situation report, which was subsequently distributed to the national coordination committee and primary response partners. Moreover, the report was reviewed at the daily coordination meetings to monitor progress, evaluate effectiveness, identify problems, plan or modify activities, allocate resources or staff, and identify epidemiologic trends.
The surveillance team conducted additional investigative activities to determine the origin of the outbreak, identify the index case, and trace the chain of transmission. The epidemiologic investigation included analysis of surveillance data (eg, the case notification forms, case line listings, and contact registers), as well as interviews with surviving EVD cases, relatives of deceased cases, contacts, health workers, traditional healers, and community members in the areas where cases were identified.
The findings of the epidemiologic investigation suggest that all confirmed and probable cases originated from a single chain of transmission. The index case was found to have direct zoonotic exposure through contact with the carcass of a wild boar or nonhuman primate on March 15, 2017, followed by onset of symptoms on March 27, 2017. All subsequent cases resulted from human-to-human transmission. 2 The investigative activities further revealed contextual factors that contributed to the 46-day delay between the index case's symptom onset and the official outbreak declaration on May 12, 2017, including insufficient knowledge of EVD case definitions at the health center and among community health workers, lack of community-based surveillance systems and tools, and the use of traditional healers for first-line care and treatment.
Lessons Learned
Drawing on the surveillance team's experience in conducting outbreak response activities in Likati, we describe 6 critical lessons learned and offer practical recommendations to improve case detection, epidemiologic investigation, and the supportive information and communication technology infrastructure during zoonotic disease outbreaks in rural DRC and other resource-limited rural settings (Table 1).
Lessons Learned and Practical Recommendations from the Ebola Outbreak in Likati District, DRC, May to June 2017
Assess and Adapt Case Definitions and Reporting Tools to the Outbreak Context
At the outbreak onset, the surveillance team reviewed and updated case definitions and reporting tools (last updated in 2015) to facilitate effective case detection and management. The standard EVD case definition was broadened for community use to improve ascertainment of all illness and deaths that were potentially attributable to EVD and warranted further investigation. 22 More detailed criteria were developed for facility-based health workers and the surveillance team to assess and classify alerts and suspected cases as probable, confirmed, or non-cases. Reporting tools were updated to improve the quality of case and contact data. This included registries and forms for case notification and investigation, contact tracing and monitoring, patient monitoring, and alert investigation. To reinforce accuracy and standardization, the surveillance team trained health workers at the facility and community level on the modified case definitions and reporting tools, monitored daily for correct usage, and provided corrective guidance as needed.
Rapidly Deploy a Community Alert System Using Context-Appropriate Technology
A well-publicized, low-resource community alert system can enhance timely and widespread detection of suspected cases in resource-limited areas. The surveillance team quickly identified the need for community-initiated alerts and established a simple system for use with basic (voice and SMS only) mobile phones, providing the following advantages: (1) they were capable of rapid deployment, (2) they required minimal resources and financial support, and (3) they used appropriate technology for Likati's resource-limited setting (Figure 2). The system proved to be an effective and well-used tool for rapid identification of potential cases and was cited by WHO as a critical factor for improved early detection of suspected cases. 23 However, the Likati model may not be the most effective strategy for outbreaks that are larger in scope or situated in areas with better information and communication technology capacity. A situational analysis is required during each outbreak to assess if there are other, more contextually appropriate mechanisms for community members to quickly and inexpensively communicate alerts (eg, call centers).
Build Local Capacity for Case Detection and Reporting
Effective surveillance and rapid detection of emerging health threats requires an adequately trained public health workforce capable of identifying, investigating, and reporting essential information about public health threats. 24 During the Likati outbreak, delayed detection and reporting resulted in a 46-day period between the date of symptom onset for the index case and the notification from provincial health authorities to the ministry of health of a potential EVD outbreak. Subsequent investigation showed that detection was hindered by the use of traditional healers as first-line health providers, a challenge that was also well-documented in the 2014-2016 EVD outbreak in West Africa. 25 Case detection and reporting can be further delayed by community health workers' insufficient knowledge of EVD signs and symptoms and poor comprehension of EVD case definitions. By engaging community health workers in the surveillance process through participatory training and direct supervision from local health authorities, the timeliness of both disease detection and reporting is improved.17,26
Develop Context-Specific Plan for Outbreak Data Collection, Management, and Use
Procedures for managing case and contact data should be well documented to improve timely and accurate data sharing among contact tracers, supervisors, and the surveillance team.21,27 To understand the local environment and develop context-appropriate outbreak data management procedures, the surveillance team rapidly assessed the existing data management systems and information and communication technology infrastructure in Likati district. This included an assessment of data management processes and data flow from the Likati district health office to the Bas-Uélé provincial health office and to the ministry of health in Kinshasa. Specifically, the team reviewed how the current information system managed Ebola case investigation, case reporting, case management, contact tracing, contact follow-up, laboratory testing, laboratory results, daily situation reports, and contact mapping, then developed responsive strategies for improving outbreak data management. For example, community health workers lacked the technology to collect global positioning system coordinates at the homes of case contacts or places they visited, which is important for daily contact tracing and prompt management of potential cases. 28 Therefore, a team was sent to the field to collect geolocation information via an Android-based application.
The surveillance team further improved management and use of outbreak data by implementing quality assurance procedures and promoting data-driven decision making. They established procedures to review data received for accuracy and completeness, returning to the source for data validation as needed. For example, when critically important data were identified as missing from case notification forms, a member of the surveillance team traveled to the location where the form originated to obtain the missing information. Furthermore, the team established daily meetings to review outbreak data, monitor progress, evaluate effectiveness, identify problems, plan or modify activities, allocate resources or staff, and identify epidemiologic trends. For example, data on the geographical distribution of cases and contacts were used to determine where to send essential equipment, such as satellite telephones, to rapidly report suspected cases and target community awareness campaigns.
Strengthen Operational Support for Essential Communication and Information-Sharing Networks
As part of the rapid assessment of the information and communication technology infrastructure available for outbreak response activities, the surveillance team assessed availability and functionality of information and communication technology networks and equipment, including computing hardware, software, and technical support systems in the outbreak epicenter. The assessment identified inadequate functionality of existing infrastructure at the district health office—specifically, damaged solar system kit or batteries, lack of electricity, no staff trained to resolve connectivity issues, and lack of vendor support to assist with maintenance of very small aperture terminal (VSAT) satellites, which are used for 2-way communication. Although 2 generators were installed to provide power to the district health office, lack of fuel remained a problem. The absence of a suitable system to automatically manage internet access led to disruptions in connectivity due to overloaded bandwidth, which had to be resolved by limiting the number of users at any given time and regularly changing the wifi encryption key. Two major national telecommunications networks (Vodacom and Orange) were available in Likati; however, they were slow and unstable and covered only 4 of the 11 health areas.
In response to identified constraints, the surveillance team purchased 2 satellite phones to facilitate communication and reporting of suspect cases and contact tracing information between the surveillance team and health areas without network coverage. Solar panel kits were also purchased and installed in remote health areas to charge mobile and satellite phones. Additionally, the surveillance team advised on information and communication technology resource management, helped troubleshoot functionality issues, and assisted outbreak partners, laboratory staff, and local health workers with hardware and software issues.
Conclusions and Recommendations
The public declaration of the 2017 Likati EVD outbreak came 46 days after the index case became symptomatic and 19 days after the first patient reported to a health center with Ebola-like symptoms.
2
This delay in detection and reporting reveals possible weaknesses in the existing surveillance system for epidemic-prone diseases. In the Global Health Security Agenda, improving real-time surveillance and reporting of epidemic-prone diseases is a critical strategy for rapidly detecting and responding to public health threats.
10
In areas such as Likati, where there is an elevated risk of exposure and transmission of zoonotic diseases, a well-functioning system for real-time surveillance and reporting serves as a critical early warning system and provides essential information for assessing the scale and distribution of a potential outbreak. However, this will require significant investment in building public health workforce capacity and healthcare infrastructure. The lessons learned during the Likati outbreak provide insight into interventions for improving outbreak response in the DRC and other rural resource-limited settings and can be used to build foundational surveillance capacity, in alignment with the Global Health Security Agenda objectives, for real-time surveillance and reporting. Our recommendations are: