
Abstract
Community-based surveillance can be an important component of early warning systems. In 2016, the Côte d'Ivoire Ministry of Health launched a community-based surveillance project in 3 districts along the Guinea border. Community health workers were trained in detection and immediate reporting of diseases and events using a text-messaging platform. In December 2017, surveillance data from before and after implementation of community-based surveillance were analyzed in intervention and control districts. A total of 3,734 signals of priority diseases and 4,918 unusual health events were reported, of which 420 were investigated as suspect diseases and none were investigated as unusual health events. Of the 420 suspected cases reported, 23 (6%) were laboratory confirmed for a specific pathogen. Following implementation of community-based surveillance, 5-fold and 8-fold increases in reporting of suspected measles and yellow fever clusters, respectively, were documented. Reporting incidence rates in intervention districts for suspected measles, yellow fever, and acute flaccid paralysis were significantly higher after implementation, with a difference of 29.2, 19.0, and 2.5 cases per 100,000 person-years, respectively. All rate differences were significantly higher in intervention districts (p < 0.05); no significant increase in reporting was noted in control districts. These findings suggest that community-based surveillance strengthened detection and reporting capacity for several suspect priority diseases and events. However, the surveillance program was very sensitive, resulting in numerous false-positives. Learning from the community-based surveillance implementation experience, the ministry of health is revising signal definitions to reduce sensitivity and increase specificity, reviewing training materials, considering scaling up sustainable reporting platforms, and standardizing community health worker roles.
Community-based surveillance is the systematic detection and reporting of events of public health significance in a community by community members.1-5 Community health workers play an important role in early warning of emerging events by engaging with their communities to detect potential public health events and connecting individuals to health services.6-11 Community health workers are particularly valuable in areas of the world with limited access to health care. 12 A recent World Health Organization (WHO) technical meeting recommended that a strong community-based surveillance program have the following characteristics: It should be integrated in a formal surveillance structure and be actionable and timely, and it should have perceived benefits to the community, well-defined reporting mechanisms, a feedback mechanism, and a monitoring and evaluation process. 1
In April 2016, the Côte d'Ivoire Ministry of Health, in collaboration with the International Rescue Committee (IRC), a nonprofit organization, launched a community-based surveillance project in 3 health districts located along the border with Guinea, building on an existing framework for detecting cases of Ebola virus disease. This project was designed to fit within the structure of the Integrated Disease Surveillance and Response (IDSR), a surveillance platform used in most of Africa13-15 to strengthen the International Health Regulations (IHR 2005). Almost 2 years after the implementation of community-based surveillance, a team from the US Centers for Disease Control and Prevention (CDC), at the request of the Ministry of Health, performed a rapid review of the community-based surveillance project to understand its successes and challenges. The review consisted of collection and analyses of data from the national electronic surveillance system and ad hoc interviews with the Ministry of Health and IRC. This article describes the process of implementation of the community-based surveillance project in Côte d'Ivoire and results from the data review.
Methods
Selection of Health Districts
Côte d'Ivoire's Ministry of Health selected 3 health districts in the northwestern health region of Kabadougou-Bafing-Folon for the community-based surveillance implementation: Odienné, Touba, and Minignan districts (Figure 1). These districts were considered vulnerable to potential emergence of a public health threat because of their location on the country's frontier with Guinea and their limited access to and use of health services.
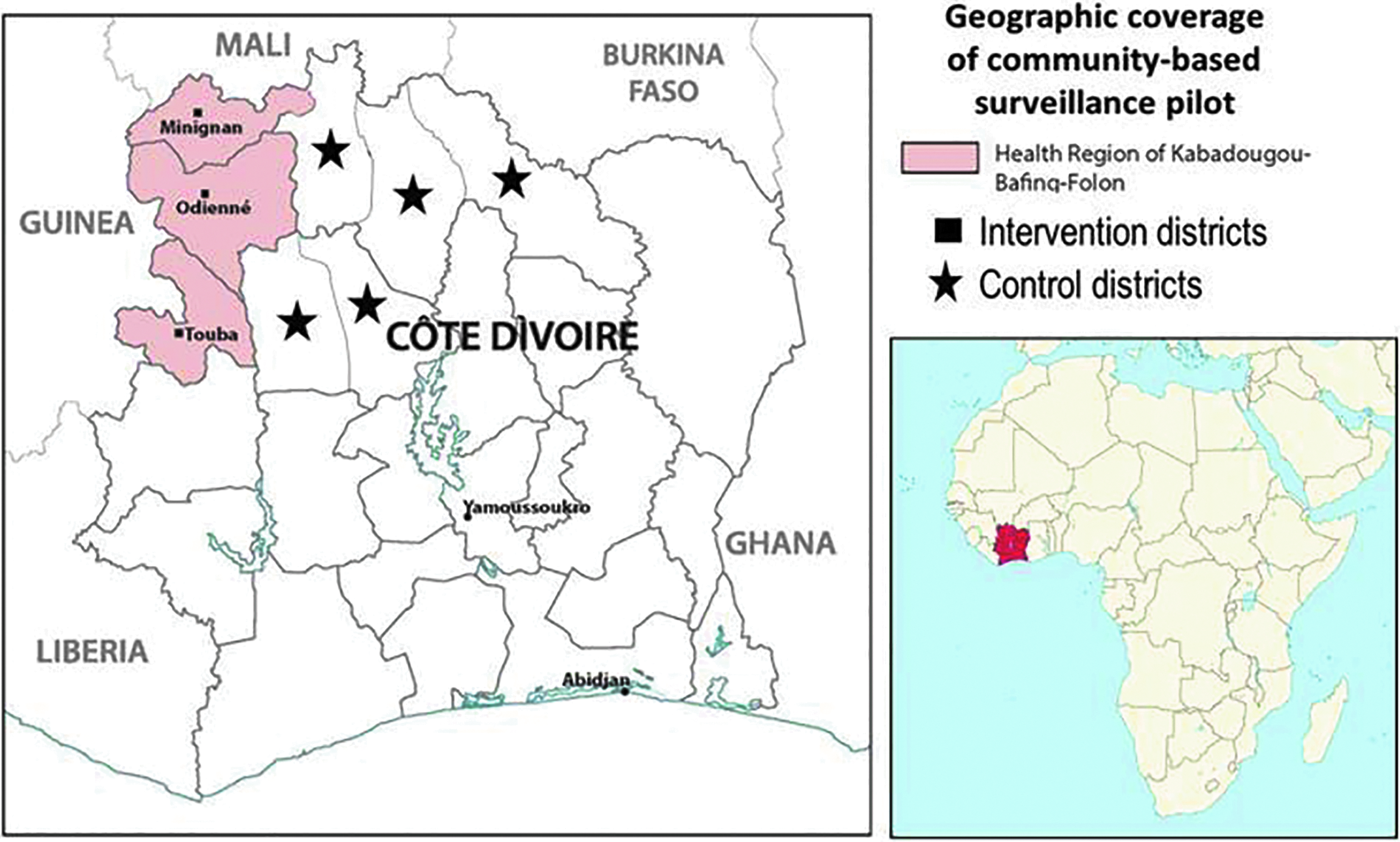
Map of Côte d'Ivoire with the health region of Kabadougou-Bafing-Folon highlighted, and the 3 intervention health districts for community-based surveillance denoted. The black stars represent the 5 control districts in the health regions of Poro-Tchologo-Bagoue and Worodougou-Bere. Inset: Map of Africa with Côte d'Ivoire highlighted in red.
Signals for Diseases and Health Events
Côte d'Ivoire's Ministry of Health selected 5 priority diseases—polio, cholera, measles, meningitis, and yellow fever—and 5 unusual health events: illness in a healthcare worker, death of a healthcare worker, unexpected animal or fish deaths, a sudden or unexplained death in the community, and arrival in the community of any person coming from a country or region experiencing an epidemic. Signals were defined as any information representing a potential acute risk to human health, and signals were designed to be broad and simple so that community health workers and community members with limited technical training and backgrounds could participate in community-based surveillance. 16 Signals for priority diseases were based on IDSR technical guidelines. 13
Workforce Training
A total of 541 community health workers participated in community-based surveillance: 498 were already providing services in communities either for Integrated Management of Childhood Illness (IMCI), Home Management of Malaria (HMM), or Ebola with the organizations IRC and Save the Children. An additional 43 community health workers were newly recruited for the pilot community-based surveillance program. Community health workers, health facility staff, and district and regional epidemiologic surveillance officers were trained on community-based surveillance. Training focused on detection of priority diseases and unusual health events, with instructions on how to complete data collection and notification forms. Community health workers and health facility staff were also trained in how to code signals transmitted by text message.
Data Collection and Reporting Tools
As part of community-based surveillance implementation, a text-based reporting system for immediate notification by the community health workers was implemented using FrontlineSMS, an open-source platform that enables epidemiologic information to be sent from texts on mobile phones. The FrontlineSMS software was installed on surveillance computers for data processing so that texts could be received. Data collection tools were adapted from those created for surveillance during the Ebola outbreak in early 2015. 17
Resources
Mobile phones with text messaging capability were provided to community health workers along with phone credits to use for reporting. Communication materials, such as hand-held flip charts with simple pictures of priority diseases and health events, were developed and distributed to community health workers and health facilities for community-wide education and sensitization. Community health workers were paid a small financial incentive to participate in implementation. Notification forms from Côte d'Ivoire's IDSR manual were printed and distributed to community health workers for manual data entry of aggregate data. In addition, IDSR case investigation forms were distributed to health facility staff. Laptop computers were provided to epidemiologic surveillance officers at district and regional levels.
Information Flow
The existing IDSR reporting structure was enhanced as follows: At the community level, community health workers were trained to actively look for signals, and either by home visits or through notifications, community health workers received information from informant networks in the community. Community health workers identified and selected people who were highly regarded in their community to serve as community informants, for sensitization and inclusion in the informant network. These informants included community leaders such as youth representatives, women's representatives, traditional healers, administrative authorities, and religious leaders.
As soon as community health workers identified a signal, they sent a text message with the code of the signal detected, which simultaneously notified staff in the health facility and epidemiologic surveillance officers in district and regional offices. Community health workers were instructed to send daily text notifications, even when there were no signals to report. In addition, every week, community health workers completed notification forms with the total number of signals identified during the past 7 days. Community health workers also completed a check-in form for each detected signal. On a weekly basis, community health workers sent both notification and check-in forms to health facilities.
When staff at health facilities received text notifications from community health workers, the supervising nurse was responsible for initial triage and verification, either via telephone or by visiting the community. For triage, nurses first called community health workers to obtain additional data. If the signal met the criteria for a priority disease or unusual health event, nurses visited communities and verified whether signals represented public health events necessitating further investigation. If investigation was needed, nurses reported the situation to the district epidemiologic surveillance officer by phone and entered it into the FrontlineSMS database.
Following standard IDSR guidelines (not part of the community-based surveillance project), the district epidemiologic surveillance officers conducting the investigation determined if the case should be classified as a suspected case and whether specimens should be collected in collaboration with health facilities. Specimens were sent to the Pasteur Institute of Côte d'Ivoire (IPCI) in Abidjan for laboratory testing when appropriate. The epidemiologic surveillance officer entered suspected cases of diseases into the Côte d'Ivoire Ministry of Health's Magpi website server, which operated as a private cloud-based mobile application (https://home.magpi.com/). Magpi is the national electronic IDSR surveillance reporting system in which all investigated cases are reported. Districts coordinated response for all confirmed cases. The Magpi database served as the source of data for this article (Figure 2).
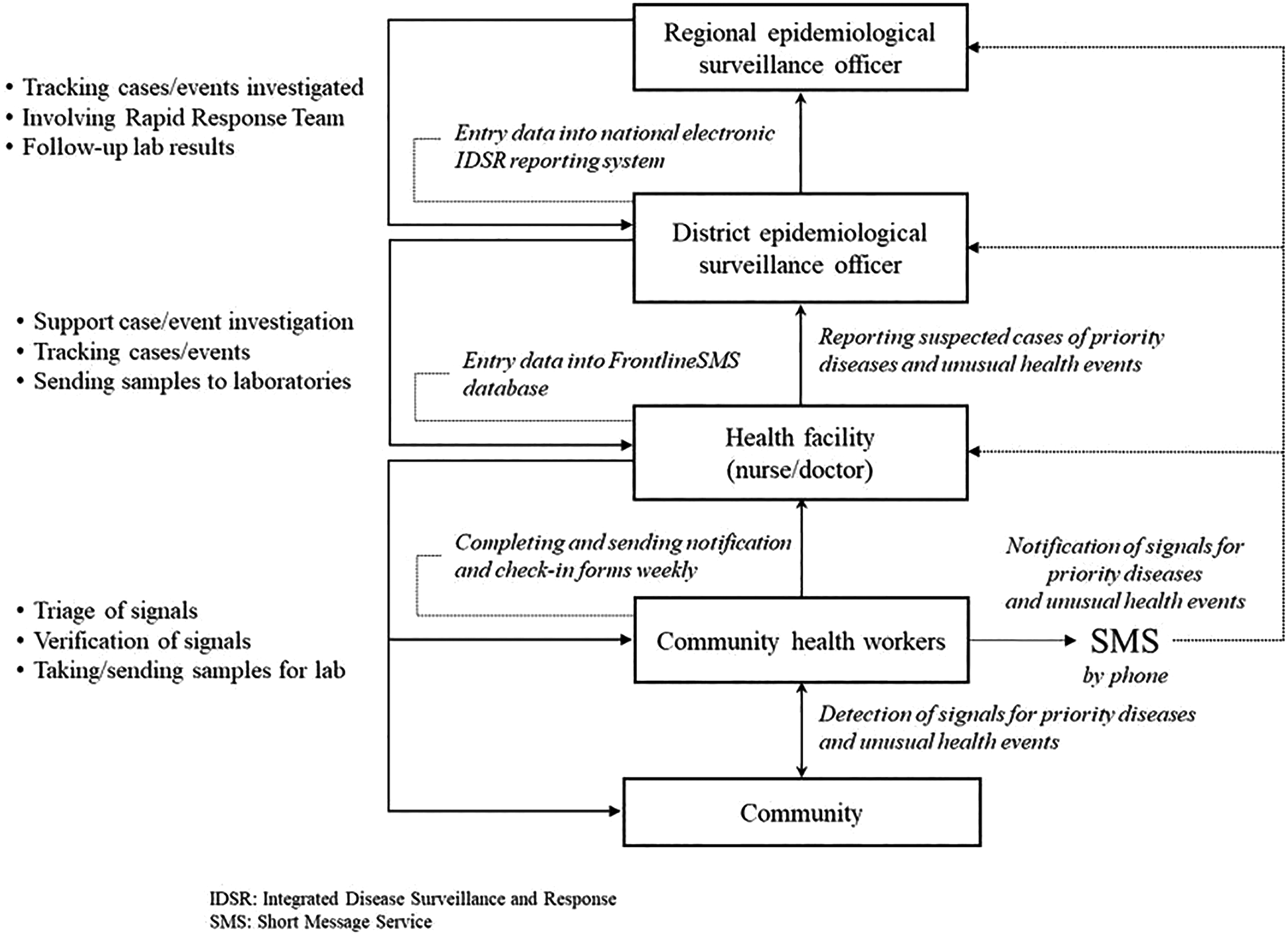
Flow of information from the community to the regional level in Côte d'Ivoire community-based surveillance. Community health workers report to health facilities, who report to the health district and ultimately the health region.
Supervision of Community Health Workers
A team consisting of IRC and district-level health staff conducted supportive supervision of community health workers. During these supervisory visits, the team ensured knowledge of signal definitions and checked that community health workers correctly coded and entered diseases and events by text message.
Data Analysis
Community-based surveillance implementation started in April 2016 and continued until December 2017. Demographic data for these analyses were obtained from the Population and Housing Census of Côte d'Ivoire from 2014, and training and signal definition data were provided by IRC. Surveillance data were extracted from Côte d'Ivoire's electronic IDSR surveillance reporting system from January 2014 to December 2017. Signal data were retrieved from the text message database through IRC.
The total number of signals reported by community health workers was calculated as well as the number of suspected cases of priority diseases. To represent the number of potential outbreaks reported by intervention districts, clusters of suspected cases of priority diseases were identified from 2014 to 2017. A cluster was defined as 2 or more suspected cases occurring in the same community in the same 7-day period. Assuming they were Poisson variates, the number of clusters reported for 2017 (observed) was compared to the number of clusters in 2015 (expected) to evaluate differences in cluster reporting before and after implementation of community-based surveillance.
Incidence rates of reporting of suspected cases of priority diseases were calculated by dividing the number of suspected cases of disease reported from the districts to the IDSR each year by the district's population from each year from 2014 to 2017. All incidence rates and 95% Mid-P exact confidence intervals for the incidence rates were reported per 100,000 person-years.
Incidence rates of reporting of suspected cases of diseases were compared in the intervention districts for the calendar years before and after implementation of community-based surveillance (2015 vs 2017). The rate difference was computed by subtracting the incidence rate in 2015 from the incidence rate in 2017. The same analysis was performed on IDSR data extracted from 5 health districts neighboring the intervention districts (control districts) (Figure 1). Specifically, 2 of the 4 health regions, Poro-Tchogo-Bagoue (PTB) and Wodoroguou-Bere (WB), neighboring the intervention districts were randomly selected, and the districts of Korhogo, Ferkessedougou, and Bagoue were selected from PTB, and Mankono and Seguela from WB as controls. Rate differences were compared between intervention and the control districts. Statistically significant differences in the rates were determined using the Mid-P exact test with a p < 0.05 as a threshold for statistical significance. Data analysis was conducted using OpenEpi 3.01 (2013).
No ethical approval was required for this study as data used in this article were obtained from routine public health surveillance.
Results
Demography of Intervention Districts
The 3 intervention districts were comprised of 508 communities with a total of 501,328 inhabitants, representing 2% of the country's population. Population sizes ranged from a total population of 101,403 inhabitants in Minignan district to 203,368 in Odienné district. Population density was higher in Touba district (23 per km2) than Odienne and Minignan district (15 and 14 per km2, respectively) (Table 1). Odienné district is urban, whereas Minignan and Touba are rural.
Implementation of community-based surveillance in Côte d'Ivoire: Demographics and workforce trained, by implementation district
Workforce Trained on Surveillance
A total of 649 persons were trained in community-based surveillance, of which 541 (83%) were community health workers. At the health facility level, 83 registered nurses, 7 doctors, and 13 other health facility workers were trained in community-based surveillance. Five district and regional epidemiologic surveillance officers received community-based surveillance training as well (Table 1).
Signals and Events Reported
From April 2016 until December 2017, a total of 3,734 signals for priority diseases were reported by community health workers. Of these, only 420 (11.2%) were suspected disease cases: 198 measles, 166 yellow fever, 33 acute flaccid paralysis, and 23 meningitis. No suspected cases of cholera were reported (Table 2). Percentages of signals verified as suspected cases of disease was 16% for meningitis, 18% for measles, 29% for yellow fever, and 49% for acute flaccid paralysis. There was a significant difference between different priority diseases (p < 0.01), except for meningitis and measles (p = 0.551) (Table 2). Specimens from 412 suspected cases of priority diseases were tested by the laboratory at IPCI in Abidjan, of which 23 (6%) were positive for a specific pathogen. Positivity rates were 7% for measles, 6% for yellow fever, and 5% for meningitis. No confirmed cases of polio were reported.
Signals, suspected cases of priority diseases, and unusual health events reported by intervention districts after implementation of community-based surveillance, April 2016 to December 2017
A total of 4,918 unusual health events were reported. For unusual health events, the most common signals reported were 886 unexpected animal or fish deaths and 658 instances of people arriving in the community from a country or region experiencing an epidemic (Table 2). None of these signals was recorded as an event in IDSR.
Clusters of Priority Diseases
Following implementation of community-based surveillance, there was an increase in reporting of clusters for both suspected measles and yellow fever in intervention districts (Figure 3). A nearly 5-fold increase in reporting was observed in suspected measles clusters after implementation of community-based surveillance (14 clusters in 2017 vs 3 clusters in 2015). There were 8 suspected yellow fever clusters detected in 2017 compared to only 1 in 2015. Both increases in reporting were statistically significant (p < 0.01).
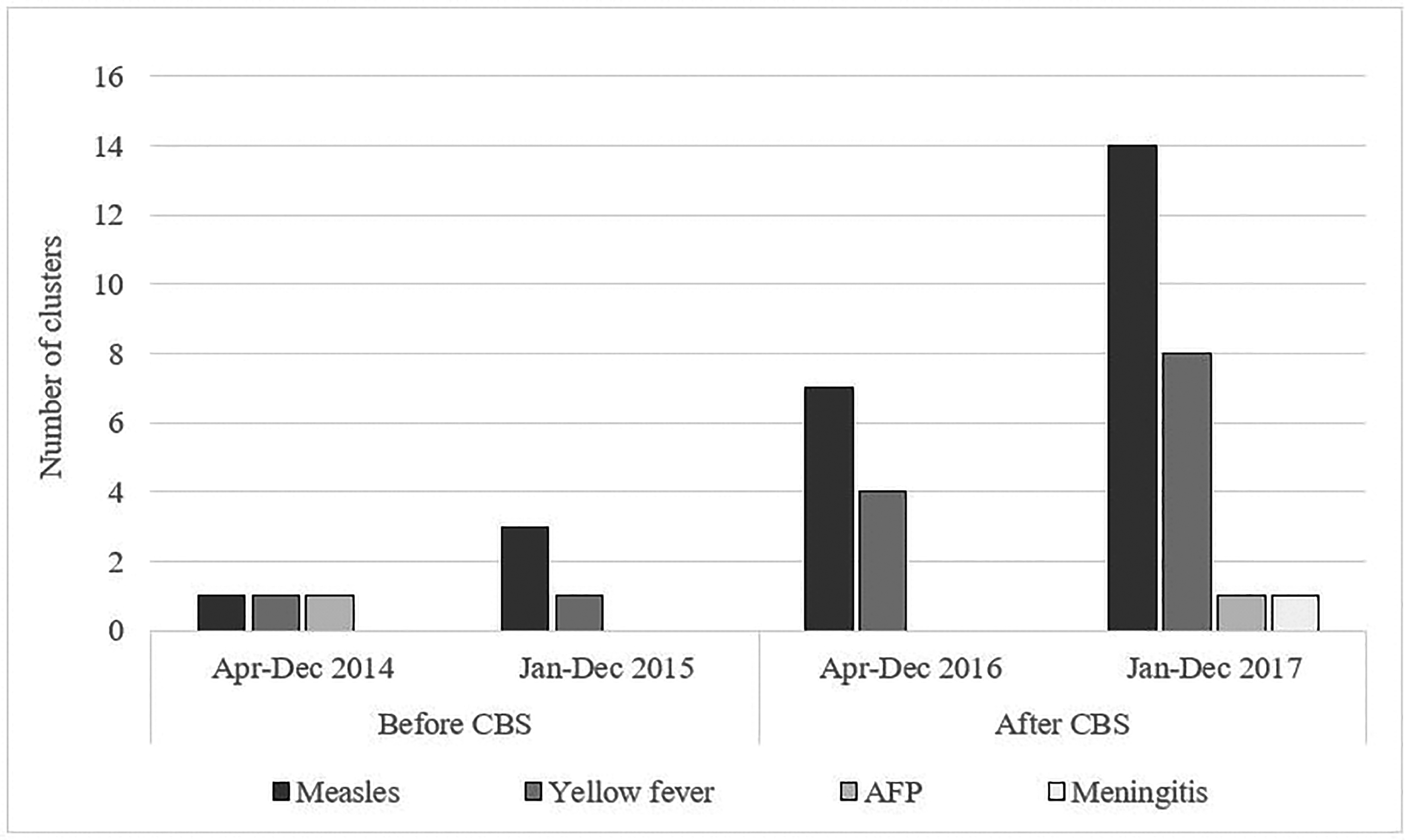
Number of clusters of suspected cases of priority diseases identified before and after implementation of community-based surveillance in intervention districts, Côte d'Ivoire, 2014-2017. CBS = community-based surveillance.
Incidence Rates
On average, control districts were more densely populated than intervention districts (36 persons per square km vs 17 persons per square km), but the percentage of people living in urban areas was the same in both groups (43%). The ratio of primary care health facilities per 10,000 individuals was higher in intervention than control districts (1.8 primary care health facilities per 10,000 population vs 1.1 primary care health facilities per 10,000 population) as was percentage of healthcare use (individuals using healthcare services each year) (52% vs 44%).
Regarding geographic accessibility, the proportion of people living less than 5 km from a health center was higher in control districts compared to intervention districts (59% vs 50%) (Table 3). Figure 4 shows an upward trend in incidence rates of reporting of suspected cases of measles and yellow fever in the intervention districts over time. This trend started in 2016, after implementation of community-based surveillance, with an increase in 2017. In comparison, incidence rates remained notably lower and virtually unchanged in the control districts. For acute flaccid paralysis and meningitis, a slight upward trend was detectable in the intervention districts, with corresponding incidence rates remaining low and without major changes in the control districts.
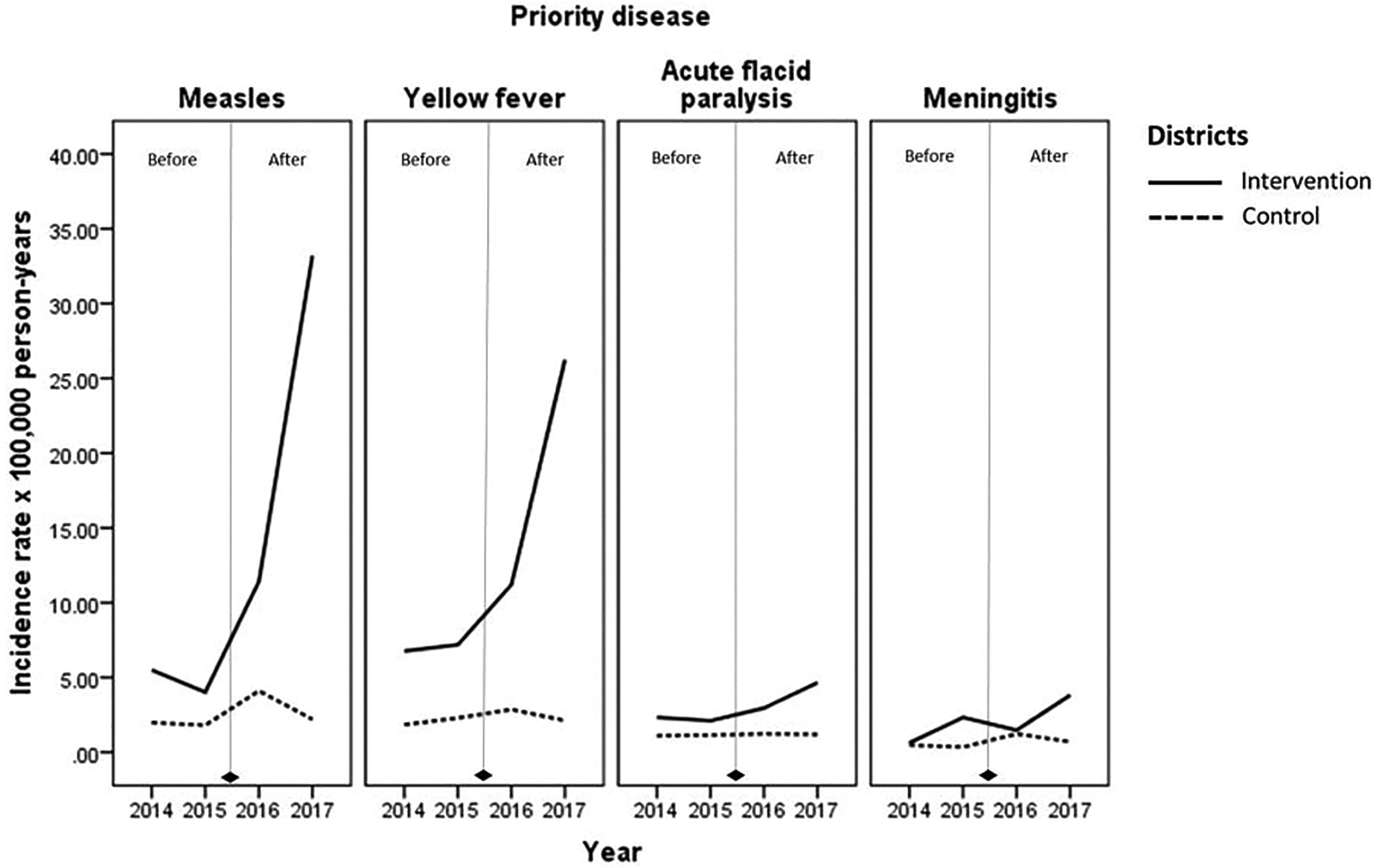
Incidence rates of suspected cases of priority diseases reported through IDSR from the intervention and control districts from 2014 to 2017, Côte d'Ivoire.
Demographics and healthcare coverage profile of intervention and control health districts, CBS implementation in Côte d'Ivoire, 2014 to 2017
Note. PCHF = Primary care health facility (établissements sanitaires de premier contact).
Incidence rates of reporting suspected measles, yellow fever, and acute flaccid paralysis were significantly higher in 2017 than 2015 in the intervention districts (Figure 4). The rate difference was 29.2 (95% CI 23.7, 34.7; p < 0.01) per 100,000 person-years for measles, 19 (95% CI 13.8, 24.2; p < 0.01) per 100,000 person-years for yellow fever, and 2.5 (95% CI 0.2, 4.9; p = 0.035) per 100,000 person-years for acute flaccid paralysis. The rate difference was not significant for meningitis in intervention districts. None of the rate differences were statistically significant in control districts. All rate differences were significantly higher in intervention than control districts (Table 4).
Comparison of incidence rates of suspected cases of priority diseases before and after community-based surveillance implementation, and between intervention and control districts, Côte d'Ivoire, 2014 to 2017
CBS = community-based surveillance.
The CBS intervention started in April 2016.
Significance at p < 0.05.
Discussion
Community-based surveillance has been an integral part of the IDSR strategy to improve public health surveillance and response, linking communities with local health facilities. 5 However, prior to pilot implementation in Côte d'Ivoire, IDSR primarily included collection of aggregated data from healthcare facilities and weekly reporting. Recognizing this gap, during and after the West African Ebola outbreaks the Côte d'Ivoire Ministry of Health moved to enhance community-based surveillance within the IDSR framework in 3 intervention districts by (1) condensing the reportable disease list to 5 diseases; (2) defining and providing a list of unusual health events that needed to be reported; (3) training community health workers, health facility staff, and district- or region-level epidemiologic surveillance officers in community-based surveillance, including triaging and verifying the signals; and (4) providing community health workers a text-based reporting system for immediate notification. With these enhancements, an increase in reports from the communities in the intervention districts was recorded. This reporting was significantly higher than reporting in control districts. This finding is similar to other recent studies demonstrating the value of community-based surveillance as an early warning system.3-5,9,10
The study has limitations. The first limitation was heavy reliance on the electronic IDSR database for data analyses. As designed and implemented, the community-based surveillance program detected events that did not fall into the published list of IDSR reportable diseases; accordingly, the IDSR electronic database had no provision to record these events nor the elements of response once the case investigation began. Thus, although the study was able to collect the signals reported by community health workers through the SMS program and information from the IDSR database, data on suspected cases and events of non-IDSR diseases that occurred and were responded to by districts were not captured. For example, 1,097 signals were reported in the SMS database under the signal “anyone suffering with fever with pimples on the body.” Of these, the IDSR database had 198 entries as suspected measles cases, of which 13 tested positive for measles. No data were available for the remaining 899 of 1,097 reports of fever and rash. In informal interviews with district epidemiologists and IRC staff, it was understood that some of the fever and rash cases may have been chickenpox or other non-measles childhood diseases and were not all false alerts by the community health workers. This challenge was greater for unusual health events data: Since most of these reports had no detailed entries (as they did not fit into the IDSR list), there were no data on whether these signals were investigated or responded to, limiting the scope of our analyses.
For this pilot project, the Ministry of Health designed simple descriptions or “signals” that could be understood by community health workers; this approach combined disease-specific definitions with broader pattern recognition definitions, such as animal deaths and healthcare worker sickness, to recognize emerging events resulting in a highly sensitive system. For example, the Ministry of Health designed the signal definition for detection of cholera cases as “anyone who has 3 abundant liquid stools during the day.” Using this criterion, more than 1,500 signals were reported, but after verification and/or investigation, the districts found that there were no cases of cholera. If the intent was finding cholera, then all these signals would be considered false alerts and need to be redesigned to be more specific, thereby reducing background noise.
Any kind of reporting from community health workers requires some kind of response from the public health system to rule in or rule out events; this requires significant resources in terms of time and money from the system. Thus, while it is important to have vigilant community health workers, it is also important to design the signal definition to be less sensitive to reduce the burden on the public health system. A recent study from Vietnam used the following definition for cholera in community-based surveillance: “any person ≥5 years old with 3 or more rice watery stools in 24 hours, with dehydration severe enough to require admission to hospital or cause death.” 10 A similar signal definition could be considered by the Ministry of Health to reduce the high number of reports of cases that are not cholera.
Another example that illustrates the use of very broad signal definitions that may result in increases in false reporting are the signals “any death of a healthcare worker” or “healthcare worker illness.” This signal was likely designed for the reporting of diseases such as Ebola virus disease or Middle East respiratory syndrome; however, none of these signals resulted in detection of these diseases. Adding a severity qualifier such as “needing to be hospitalized” or “resulting in death” may add more specificity to this signal. It is interesting that although the West African Ebola outbreak propelled the Ministry of Health to strengthen community-based surveillance, the list of signals did not include reporting Ebola disease.
The Côte d'Ivoire community-based surveillance project piloted a text-based reporting system to enable real-time reporting of signals. Before the introduction of the text-based system, community health workers had to travel significant distances with limited transportation capacities to health facilities for notification. These practical challenges greatly hindered notification, particularly in rural settings. The availability of a text-based system appears to have helped remove some reporting obstacles and may account for the increase in the number of notifications (review of available field visit reports, data not shown). In spite of the benefits of text-based reporting, this system does pose challenges in resource-limited environments. First, in intervention districts, while cellular coverage was not a problem in most areas, many rural villages had limited electricity. Community health workers relied on charging their phones at health facilities during their visits for weekly reports. To mitigate this challenge, IRC is working to provide community health workers with solar-powered cell phones in intervention districts. Second, community health workers initially found it difficult to understand and use the code-based text system required to report signals for priority diseases and unusual health events. This led to numerous wrong entries and false alerts but was corrected by continuous mentorship and refresher training led by the IRC and district team during their bimonthly supervisory visits. Lastly, there were significant costs associated with operating the text-based system. These costs may have implications for the Côte d'Ivoire Ministry of Health when they expand community-based surveillance and launch it nationally.
The present study suggests that community health workers may help to improve reporting of suspected priority diseases and events, and that they serve as a foundation of community-based surveillance. In this study, the community health workers who were part of several nongovernmental organizations charged with specific tasks were trained to take on additional responsibilities for community-based surveillance and were given financial incentives to participate. Motivation of community health workers is an important consideration, but incentivizing these workers may not be sustainable when scaled up nationally. Other countries have integrated community health workers into their health system or provided nonfinancial incentives to encourage community health workers.18-20 The Côte d'Ivoire Ministry of Health is currently considering publishing a national terms of reference for community health workers, allowing for these health workers to be incentivized uniformly and perform polyvalent functions (ie, these community health workers would perform universal reporting for all diseases and events, instead of disease-specific activities).
For this project, IRC and district health staff engaged in intense supervision and monitoring activities to help the program succeed. The intense supervision used in this study may not be practical for a national surveillance program since it requires time, a dedicated workforce, and money. A solution would be to integrate this community-based surveillance supervision into the routine monitoring functions of IDSR. Additionally, a robust monitoring and evaluation plan should be in place prior to implementation to enable systematic data collection that will guide implementation and assess impact.
In spite of these challenges, implementation of community-based surveillance demonstrated that increased community involvement and innovative communication strategies can help to improve signal detection and reporting. By integrating community-based surveillance into an existing IDSR surveillance and reporting platform, the program was able to strengthen public health foundations already in place.
This study has shown that careful consideration should be given to the design of signals to provide sufficient specificity so that reporting does not overwhelm the system. The Ministry of Health is currently reviewing the signal definitions used for detection to find a balance between sensitivity and specificity, synthesizing lessons learned from implementing the text-based reporting system, and working to elucidate the potential role(s) of standardized polyvalent community health workers. This review and lessons learned will help guide the next steps for scaling up community-based surveillance in Côte d'Ivoire and other countries.
Footnotes
Acknowledgments
This work was funded by a Global Health Security cooperative agreement from the Centers for Disease Control and Prevention (CDC) to the International Rescue Committee. The authors would like to recognize the contributions from the United States Agency for International Development (USAID) for their additional support of Côte d'Ivoire's community-based surveillance program.