
Abstract
The International Health Regulations (2005) dictate the need for states parties to establish capacity to respond promptly and effectively to public health risks. Public health rapid response teams (RRTs) can fulfill this need as a component of a larger public health emergency response infrastructure. However, lack of a standardized approach to establishing and managing RRTs can lead to substantial delays in effective response measures. As part of the Global Health Security Agenda, national governments have sought to develop and more formally institute their RRTs. RRT challenges were identified from 21 countries spanning 4 continents from 2016 to 2018 through direct observation of RRTs deployed during public health emergencies, discussions with RRT managers involved in outbreak response, and during formal RRT management training workshops. One major challenge identified is the development and maintenance of an RRT roster to ensure deployable surge staff identification, selection, and availability. Another challenge is ensuring that RRT members are trained and have the relevant competencies to be effective in the field. Finally, the lack of defined RRT standard operating procedures covering both nonemergency maintenance measures and the multistage emergency response processes required for RRT function can delay the RRT's response time and effectiveness. These findings highlight the importance of planning to preemptively address these challenges to ensure rapid and effective response measures, ultimately strengthening global health security.
The International Health Regulations (IHR 2005) dictate the need for states parties to establish disease outbreak response capacity and prepare to detect and respond to public health threats and emergencies. 1 Despite the commitment of 196 countries to fulfilling IHR requirements, many countries are not fully compliant, exposing all countries to potential threats in the modern global economy.2,3 Large-scale epidemics in the past 5 years, such as those seen in West Africa and the Republic of Korea, are reminders of the global potential of any outbreak.4,5 The 2014 Global Health Security Agenda (GHSA) outlined 11 discrete measurable activities, or Action Packages, to assist countries in achieving IHR compliance for public health emergency preparedness.5-8 In addition, voluntary Joint External Evaluations (JEEs) have been conducted in countries to assess health security capacity. 9 In response, national governments have sought to develop and more formally institute their emergency response capacity.10,11
Public health rapid response teams (RRTs)—interdisciplinary teams of trained individuals ready to deploy for public health emergencies—can help meet the goals set out by the GHSA when included as part of a larger public health emergency infrastructure. RRTs relate to 4 of the 2014 GHSA Action Packages: workforce development, emergency operations centers, linking public health with law and multisectoral rapid response, and medical countermeasures and personnel deployment. 11 These Action Packages highlight 3 key characteristics of RRTs: sufficiently and regularly trained, interdisciplinary or multisectoral composition, and rapid functional mobilization as part of a larger public health emergency infrastructure.
In 2015, the US Centers for Disease Control and Prevention (CDC) established the Global Rapid Response Team (GRRT). Although CDC has established mechanisms for mobilizing response teams for domestic emergencies, GRRT's mandate was to focus on enhancing CDC's global response capacity. 12 Without a preexisting, standardized approach to establishing and maintaining a rapid response workforce for international response, the GRRT had to create innovative systems and develop protocols and operations as it sought to develop a trained and ready-to-respond surge staff. 12 The lessons learned during this process provided a foundation for GRRT staff to begin working with other countries interested in building their own rapid response capacity.12,13
Historically, RRTs or their equivalents have long been used in public health emergencies.14-17 Despite this, to our knowledge, there has been no systematic or standardized guidance document on the establishment and management of a public health RRT workforce that is not limited to a particular disease. Thus, as countries and organizations have sought to develop and formalize their RRTs with the capacity to tackle a diversity of public health emergencies in alignment with IHR and the more recent GHSA initiative, a number of challenges have become apparent. Based on GRRT's experiences supporting RRT capacity in other countries, this article aims to elucidate common challenges in establishing and managing RRTs, so that countries can preemptively address these challenges, ensuring rapid and effective response measures and furthering their contribution to global health security.
Methods
From 2016 to 2018, in collaboration with ministries and other international partners, GRRT deployed staff to more than 40 countries to provide support for public health emergencies. During that time, 9 countries on 4 continents (3 African, 3 Asian, 2 Central American, and 1 South American) requested support in establishing and managing RRTs. In addition to direct country requests, GRRT also facilitated RRT management training workshops for RRT managers or their national equivalents, representing 12 additional countries (6 African, 6 Asian). Collectively, among the 21 countries that received GRRT support in establishing and managing RRTs, challenges were identified by GRRT staff through (1) direct observation of RRTs deployed during a national outbreak response, (2) discussions with RRT managers or their equivalents involved in public health emergencies, and/or (3) a formal RRT management training workshop. GRRT staff compiled challenges and gaps related to establishing and managing RRTs and evaluated the data for trends evident among countries, regardless of geographic location and local context. To ensure full disclosure of challenges and gaps, countries' anonymity has been maintained.
Results
Although the 21 countries faced a number of challenges unique to their context when establishing and managing an RRT, 3 fundamental challenges emerged across countries that led to delays in responder deployment and response activities. One major challenge involved the development and maintenance of a functional RRT roster. An RRT roster, or list of RRT members from multiple disciplines, provides up-to-date contact information and facilitates the rapid identification of personnel with the training and skills needed to effectively respond in a particular emergency. Without a roster, countries noted the lack of a pre-identified surge staff pool, rendering it especially difficult to quickly augment response activities when emergencies exceeded the full-time emergency staff's capabilities. Additionally, without a roster, the same responders were often selected to deploy based on institutional knowledge of subject matter experts and personal contacts, limiting the potential responder pool. For countries with an established roster, there were issues with keeping it up-to-date with changing data such as responder contact information, on-call availability, staff turnover, and changes in job status, as well as tracking training sessions and other administration readiness requirements to deploy for that country (eg, supervisory approval to participate, medical clearance, insurance, etc).
Training and deployment readiness underlie another major challenge: achieving a surge workforce that is ready to deploy and is properly trained to ensure fast mobilization and effectiveness during the response. Countries noted the lack of an internationally recognized, standardized competency model, curriculum, and overall approach to training RRTs to respond to public health emergencies that were not disease specific. Lack of a training paradigm led to RRT members deploying without understanding emergency response processes, key deliverables, or how to translate their subject matter expertise into timely, actionable, and data-driven objectives. Countries that did implement RRT trainings had questions regarding the most relevant content and the frequency of administering training.
Finally, the lack of defined and comprehensive RRT standard operating procedures (SOPs) addressing RRT management and emergency response mechanisms led to issues in RRT deployment and effectiveness. Countries noted that SOPs, if established at all, did not delineate all aspects of RRT maintenance and operations, commonly focusing exclusively on deployment mechanisms. Additionally, RRT SOPs were often developed in isolation, without being incorporated into countries' larger public health emergency response structure.
Discussion
Under the IHR framework, along with recent large-scale outbreaks as well as the 2014 GHSA and JEEs, countries have sought to formalize and standardize their approaches to public health emergencies and thus strengthen global health security. In building emergency response capacity, countries face a range of challenges often dictated by their socioeconomic and geopolitical status; however, certain difficulties were shared across a variety of country contexts. In the 21 countries GRRT supported from 2016 to 2018, 3 common challenges in establishing and managing RRTs were: (1) roster development and maintenance, (2) training and readiness, and (3) SOP development.
The challenge of developing and maintaining a functional RRT roster to ensure the availability of a deployable, trained, and ready-to-respond workforce was particularly difficult for countries first attempting to implement a standardized RRT model. More specifically, staff selection, establishment of a large enough surge pool (ie, enough surge staff in the event of a large-scale emergency that overwhelms preexisting response staff), and information management processes were often unexpectedly complex and time-consuming to implement. Selecting appropriate staff goes beyond simply having a process for the identification and recruitment of personnel who can fill specific roles (eg, epidemiologists, health communicators, etc), but also considers personnel who possess key skills needed for common emergencies. Not all staff will have the skillsets required—for example, an epidemiologist does not necessarily have contact tracing skills; rather, that particular epidemiologist may be more appropriate for a data management or analysis position, having never performed contact tracing.
Once relevant roles and skillsets have been determined, potential candidates need to be identified. If possible, RRT managers may consider personnel outside their immediate sector to ensure a large and diversified surge pool. This may include personnel with expertise that is critical for outbreaks commonly faced in that country but who may not work in the disease control or outbreak response units—for example, environmental health experts during cholera outbreaks, geographic information systems experts to map public health emergencies and response efforts, and animal health experts for zoonoses.
With RRT members identified, their information needs to be collected and organized in the roster to facilitate staff selection during an emergency. Relevant database headers that can ensure fast and appropriate RRT member selection during an emergency can include member name, contact information, role, key skills, languages spoken, supervisor contact information, response experience, training completion, and any administrative deployment readiness factors dictated by a country (eg, travel documents, medical clearances, insurance, etc). Planning for and undergoing regular updating is critical to account for staff turnover and changes in contact information. If data are not kept up to date, the roster will be rendered unusable when a public health emergency occurs.
Without a standardized model for RRT training, countries faced challenges in ensuring they had a deployable and effective workforce. Challenges highlighted the need for RRT members to go through an onboarding training session that addressed topics beyond public health core competencies, including an overview of the country's emergency response infrastructure and deployment processes, as well as content and exercises that assist responders in translating their subject matter expertise to an emergency response setting. As competency models are developed, role-specific training, such as RRT leadership training, can be included in the curriculum. Additionally, continuing education training or refresher training can be considered at regular intervals during a responder's tenure on the team, ensuring they are aware of any changes in the country's emergency response operations and their technical response skillset is maintained. During an emergency, just-in-time training, training that is abbreviated and tailored to the specific emergency occurring, can be considered before responder mobilization to the field.
In addition to these considerations, countries could leverage existing disease-specific response training by adapting the content to their local context and extracting response components that can be modified and expanded upon for applicability to public health emergencies in general. GRRT is aware of and supports international organizations with initiatives to define competencies and potential curricula for RRTs, such as the Global Outbreak Alert and Response Network, the West Africa Health Organization, the African Union's Africa Centres for Disease Control and Prevention, the World Health Organization Health Emergencies Programme, and Field Epidemiology Training Programs and their networks.18-23 Of particular note, WHO's Health Emergencies Programme has developed and validated open-access, standardized RRT member training for use at the national and subnational levels and, since early 2015, has trained close to 2,000 public health professionals.24,25
As RRTs are one component of a larger emergency response framework, coordination with other emergency processes in the country increases the likelihood of a successful response. Having an emergency coordination body with well-defined SOPs, as well as additional elements of a functioning public health system (eg, surveillance, laboratory, etc), are all critical to ensuring there is a framework for RRT implementation and support.10,26,27 In cases where these fundamental processes are still developing, RRT establishment can progress successfully, as long as these gaps are identified and considered in the RRT SOP. As these other processes become strengthened, their incorporation into the RRT SOPs is critical to ensuring coordination with the country's overall response mechanism.
In addition to depending on these other processes to be effective, RRTs require SOPs that go beyond simply a deployment mechanism, considering both nonemergency maintenance and emergency response phases (Figure 1). During nonemergency periods, RRTs require maintenance through staffing, maintaining rosters, training, and exercises. As discussed previously, these processes can be quite complex, requiring a substantial amount of time and effort to manage, and, thus, the size of the RRT (ie, the number of RRT members) needs to be weighed against the resources required to sustain an RRT mechanism.
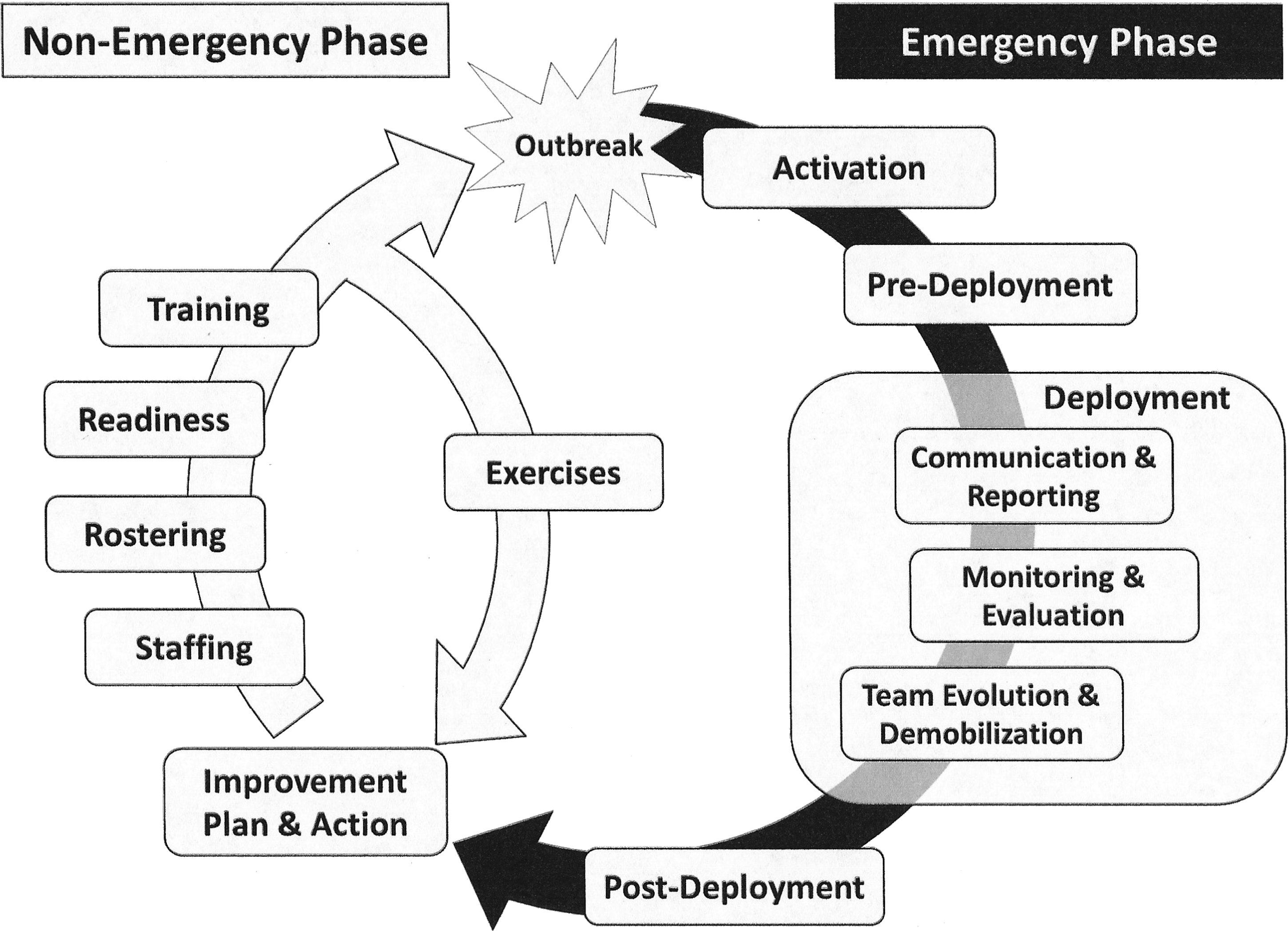
Potential Framework for Public Health Rapid Response Team Management Processes in Nonemergency and Emergency Phases
During an emergency, RRT processes include activation, predeployment, deployment, and postdeployment operations. RRT activation SOPs define the criteria to be met to justify the RRT being deployed and, once met, how members will be selected from the roster and notified. Predeployment processes can include a predeployment briefing (addressing mission objectives, status of the emergency, recent response activities, and reporting expectations), just-in-time training, and equipping team members so they are effective when they reach their target destination. Deployment SOPs consider how the RRT will fit into the larger command and control structure, how the RRT itself will be structured (including team leadership), what communication and reporting is expected or required (ie, what modality and how often), how the RRT's needs will be monitored (staffing, resources, etc), what indicators and metrics will be used to measure the RRT's effectiveness, and what criteria will be used for RRT demobilization and/or team member rotation. Postdeployment SOPs can include RRT member debriefings, evaluation of the RRT's impact, responder well-being resources (mental health, medical, etc), and formal after-action reviews.
Overall, these SOPs require a number of support elements in order to be effective, such as dedicated human resources, logistics support, transportation access, and supply and equipment availability, as well as pre-allocated funds or an established funding mechanism that can quickly disburse funds during an emergency. These elements need to be addressed in the SOPs to ensure an effective and efficient response. It is this complexity and level of detail required for the RRT SOPs covering nonemergency and emergency processes that underscores the importance of delineating these mechanisms prior to an emergency.
This analysis has a number of limitations. First, challenges were compiled by GRRT staff from observations during outbreak response, information obtained during training workshops, and discussions with RRT managers. Observational analysis is inherently biased—in this case, relying on the GRRT staff's previous response experience and singular perspective of the emergency response. Although the management workshops used a standardized approach to develop RRT SOPs and challenges were captured in a systematic manner, challenges were not documented by a formal interview or questionnaire. Second, challenges were identified specifically for RRTs being developed at the national level and responding to emergencies within their country and, thus, cannot necessarily be extrapolated to subnational, international, or regional RRT development. Although there are certainly elements of national RRT development that can assist in framing international and regional RRTs, cross-border considerations (eg, cultural awareness, passports, vaccinations, etc) and associated challenges were not included. Third, this article examined challenges for RRTs involved in outbreak response and did not encompass other public health emergencies. Finally, suggestions presented here are solely those of GRRT staff involved in supporting these countries and, thus, are not comprehensive of all possible challenges and solutions.
Even in light of these limitations, the 3 challenges identified were evident in 21 countries spanning 4 continents, emphasizing the importance of considering these particular challenges when establishing and standardizing the management of an RRT to ensure a rapid and effective response. Overall, these challenges highlight the need for pre-emergency planning for RRT implementation and management, specifically defining and delineating the mechanisms and processes for an effective RRT before a public health emergency occurs to ensure activities are proactive rather than reactive. The fact that RRT development is related to 4 of the 11 2014 GHSA action packages underscores the potential impact of addressing these RRT challenges in strengthening global health security. 11
As no standardized framework or guidance on RRT management currently exists, countries can utilize preexisting disease-specific response mechanisms and training as a foundation for developing an RRT, expanding its relevance to tackle a diversity of public health emergencies while integrating solutions to the challenges outlined here, to ensure they can effectively respond. Future work should consider the development of RRT management guidelines and standardized training. For the RRT member training packages that do exist, an evaluation of their impact and utility would be critical for informing future capacity-building efforts. Additionally, as emergencies do not respect borders, incorporating a regional perspective into these guidelines and training for RRT establishment and management will be vital for effective emergency response measures and strengthening global health security.