
Abstract
Introduction:
Female veterans are the fastest growing group of new Veterans Health Administration (VA) users, and 40% identify as belonging to a racialized group. It is unclear if racial/ethnic disparities in reproductive health care and outcomes observed among nonveterans are present among veterans. The purpose of this scoping review was to characterize patterns of racial/ethnic disparities in reproductive health care and outcomes among female veterans.
Methods:
A structured PubMed search was performed to extend a prior systematic review (from 2008–2017 to 2018–2023). We included original research on reproductive health care and outcomes in female veterans that also included a measure of association to race or ethnicity. Four hundred thirty-eight articles were identified for potential inclusion. Following PRISMA guidelines, titles and abstracts were screened in duplicate, and full articles were reviewed using a standardized abstraction form. Articles were sorted into six categories by topic (contraception, infertility, pregnancy, reproductive health screenings, gynecology, and menopause) and outcomes characterized as structural (e.g., organization of care), process (e.g., access to services), or clinical/behavioral (e.g., low birthweight) measures per Donabedian’s model.
Results:
After title and abstract screening, 53 articles were reviewed in full. Four additional articles were excluded for a final sample of 49 articles. All articles described results from observational studies, which were almost exclusively focused on veterans using VA care (94%, n = 46). Topics with the greatest number of articles included pregnancy (43%, n = 21) and contraception (24%, n = 12). Racial/ethnic disparities were detected more frequently for clinical and behavioral outcome measures than for process measures.
Conclusion:
Consistent with literature regarding other types of VA care, racial/ethnic disparities were more prevalent for clinical and behavioral outcome measures versus process measures, highlighting that access is necessary but not sufficient for reaching health equity. Understanding the racial/ethnic health disparities and their relationships with different measures of health care quality is essential for achieving health equity for female veterans.
Introduction
Racial and ethnic health disparities are ubiquitous in the United States, including unacceptably wide disparities in reproductive health care and outcomes across the life course for women and those assigned female at birth. 1 For example, Black and American Indian/Alaska Native (AI/AN) birthing people have 2–3 times higher rates of pregnancy-related mortality than White birthing people. Additionally, among those with a uterus, Black and Hispanic people are less likely than non-Hispanic White people to receive any infertility treatment, have higher prevalence and symptom severity of uterine fibroids, and have higher incidence and mortality from endometrial cancer compared with White people.2–8 As race and ethnicity are cultural constructs, racial and ethnic disparities in reproductive health care and outcomes are a product of the historical, social, structural, and political context in which individuals live their lives in the United States.9–12 Concerning female reproductive health care and outcomes, racial and ethnic disparities further reflect the intersection of racism and sexism.13–15 Health equity, or “the state in which everyone has the opportunity to attain their full health potential and no one is disadvantaged from achieving this potential because of social position or other socially determined circumstances,” as a core component of health care quality is not new; however, in 2022, Nundy et al. proposed that health equity be added explicitly as a fifth component of the quintuple aim for health care improvement.1,16–18 Health equity is also a core component of the mission of the Veterans Health Administration (VA).19,20 Understanding where racial and ethnic disparities in health and health care exist and factors contributing to these disparities is a first necessary step toward reducing and eliminating them in VA care.
Racial and ethnic health disparities in reproductive health among female veterans are important to understand, given the rise in the number of female veterans using VA, and that this growing group of veterans is younger and more racially diverse than their male counterparts. 21 ,a Forty percent of female veterans using VA identify as belonging to a racialized group, and there is a small but growing population of female veterans who identify as Hispanic or Latina.21,22 Additionally, the majority of female veterans are under age 65, with approximately 40% in their childbearing years (18–45 years old), underscoring the need for VA to provide a full range of reproductive health services over the entire life course.21,22 Female veterans receive care through designated women’s health primary care providers, increasingly in the context of VA women’s health clinics, which may incorporate gynecology care and mental health care.23,24 Specialty care other than gynecology (e.g., endocrinology and orthopedics) is available in mixed-gender settings. While all VA sites offer basic reproductive health care services, and a growing number of VA sites offer both basic and specialized reproductive health care services, some services, such as obstetric care, continue to be purchased from the community due to limited demand at any one site and the resultant inability to ensure availability of necessary specialized services.22,24,25 Specifically, VA pays for veterans to receive obstetric care outside VA from community providers. Finally, since 2019, veterans may also more easily opt to use community care purchased by VA following passage of the (Maintaining Internal Systems and Strengthening Integrated Outside Networks) MISSION Act. 26 Notably, the majority of veterans using VA care qualify for free care or reduced co-pays due to disability resulting from their service or low income. VA also provides benefits for veterans traveling long distances for needed care particularly veterans residing in rural areas. Thus, within VA, there are fewer financial barriers to accessing care compared with other health care systems, although veterans may still have to contend with other costs associated with time off work and costs associated with additional childcare.
Concurrent with the growth in the female veteran population and increased availability of reproductive health services in VA, there has been significant growth in the peer-reviewed literature addressing the reproductive health of female veterans.27,28 While a 2016 article by Carter et al. summarized the overall prevalence of racial and ethnic health disparities reported among female veterans, this review did not focus on reproductive health and precluded the recent growth in the literature. 29 Understanding racial and ethnic disparities in reproductive health among female veterans is critical for ensuring that VA meets its goal of providing high-quality, equitable care to all veterans.
The Donabedian model of health care quality measures provides a framework for examining and reporting racial and ethnic disparities across a variety of health care metrics. 30 This model categorizes quality measures such as reflecting structures, processes, or outcomes of health care (Fig. 1). Structural measures consider the settings and systems in which health care occurs (e.g., availability of providers in the surrounding community and models of care), whereas process measures are concerned with the components of care (e.g., access, services, and treatments). Importantly, structural measures in this framework are measured at the health care system level or at the level of a geographic catchment area. Clinical and behavioral outcome measures reflect the effect of health care on recovery, restoration of function, and survival (e.g., maternal mortality and perinatal depression). 30 Using this framework for health care quality to assess racial and ethnic disparities in VA can help us understand the causes of these disparities and inform strategies for achieving health equity. For example, if Black pregnant veterans are more likely to live in areas with fewer obstetrics providers (structure), they might be less likely to receive timely prenatal care (process). Additionally, bias might lead their providers to be less attentive and less likely to ensure they receive all necessary prenatal care and testing (process). Independently and cumulatively, these factors could result in an increased risk of maternal morbidity and mortality among pregnant and birthing Black veterans (clinical outcome). Such findings would suggest a need for programs and policies to improve pre-pregnancy health and increase access to obstetric providers as well as ensure that the content of this care and patient experience meets specific quality measures with the goal of reducing racial and ethnic disparities in maternal morbidity and mortality. Therefore, the purpose of this scoping review was to examine the evidence concerning racial and ethnic disparities in reproductive health among female veterans, applying Donabedian’s framework to characterize patterns in these disparities and their implications for policy and practice and identifying critical topical and methodologic gaps in the existing literature. 30
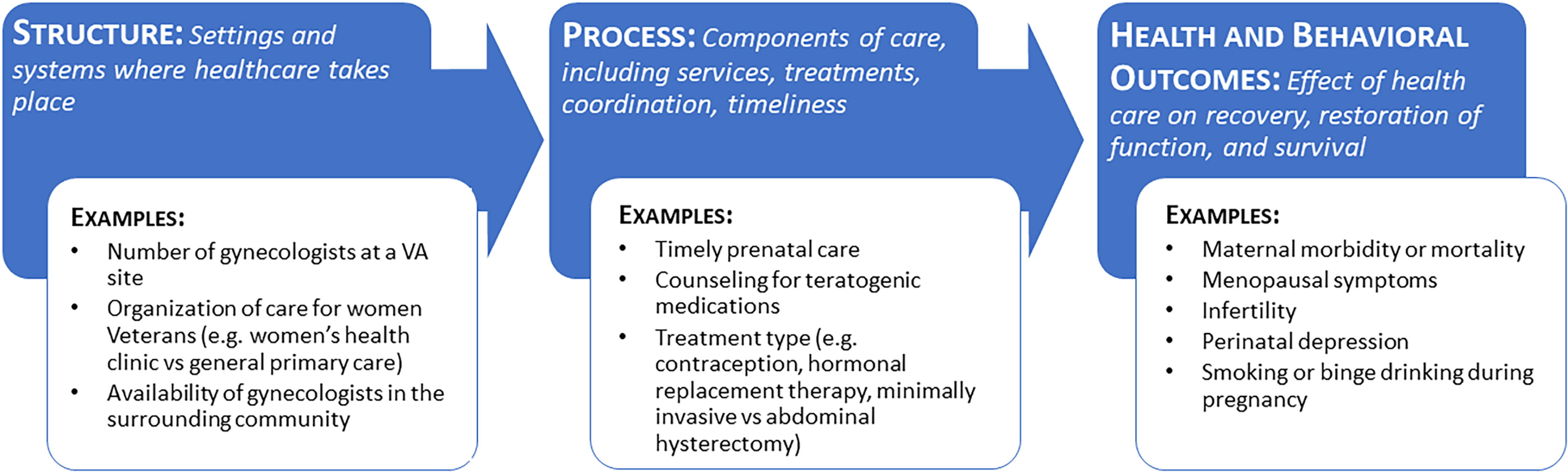
Adaptation of the Donabedian’s model of health care quality metrics for examining reproductive health care and outcomes.
Methods
We used a search strategy adapted from an earlier systematic review of the literature on the reproductive health of female veterans led by Dr. Katon.27,28 We included all articles from the prior systematic review that included articles from 2008 to 2017. 28 Based on our prior knowledge of the literature, we initially searched the literature to identify any articles addressing the reproductive health and health care of women veterans. We then reviewed titles and abstracts to identify those that potentially included findings regarding racial or ethnic disparities. We did not search the literature before 2008, as the earlier evidence report and systematic review indicated only three articles addressing reproductive health of women veterans were published between 2008 and 2011 and a review of the literature prior to 2008 found even fewer articles on this topic.27,31 We ran a structured search in PubMed using identical terms as the prior systematic review to update the article list to include those published between 2018 and 2023 (search run August 14, 2023). We also ran a second modified version of the first search in PubMed, adding the term “female.” Finally, we reviewed editorials, case reports, review articles, and reference lists to identify any additional articles. In this way, we could capture articles that included findings on racial or ethnic disparities even when this was not the primary focus of the article. Our final sample included all original research articles, published between 2008 and 2023, addressing reproductive health care or outcomes of female veterans that also included outcome frequencies by race or ethnicity or measures of association for race or ethnicity with the outcome of interest. Following Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, once the complete list of articles was identified, two co-authors (JK and KN) reviewed titles and abstracts to identify a subset of articles for full review. 32 When there was disagreement regarding inclusion/exclusion, a third author was brought in to adjudicate (LS). Articles were reviewed in full using a standardized abstraction form (see Supplementary Data) with 59% undergoing review from two or more co-authors to ensure consistency. While details such as assessment of study quality and findings were beyond the scope of this review, we collected these data as part of the abstraction process to enable future systematic reviews and meta-analyses if enough studies on a given topic were identified. We used Covidence software to track search results and exclusions. 33
For synthesis, articles were sorted into six categories based on topic (contraception, infertility, pregnancy, reproductive health screenings, gynecology, and menopause), and outcomes were defined as structural, process, or clinical or behavioral outcome measures. 30 Given the growing call to acknowledge the role of racism in determining racial and ethnic health disparities, we also carefully reviewed article texts to determine if the term racism was used in any part of the article and whether race or ethnicity was the primary independent variable of interest. 34
Results
After combining the article list from the prior systematic review with the results from the two searches and removing duplicates, 438 articles remained. Our final sample included 49 articles (Fig. 2). All studies included were observational, including one qualitative study, and nearly all exclusively focused on veterans using VA (94%, n = 46; Table 1), with half relying solely on VA administrative data (51%, n = 25). Among the three studies not focused on veterans using VA, two relied on a sampling frame generated by combining VA and Department of Defense data35,36 and one used data from a Centers for Disease Control and Prevention (CDC) national US population-based survey that included veterans and nonveterans. 37 Among those focused on veterans using VA, the period of use varied significantly between studies ranging from 2001 to 2020. The topics with the greatest number of articles included pregnancy (43%, n = 21) and contraception (24%, n = 12). Only two articles included at least one structural measure (8%), and the remainder were split nearly evenly between process measures (53%, n = 26) and clinical and behavioral outcomes (53%, n = 26). Five articles (10%) included process and clinical or behavioral outcome measures. Only 35% of articles included race and ethnicity as the primary independent variable (n = 17) and 27% (n = 13) named racism as a cause for racial disparities. Additionally, few if any articles included measures of racism at the interpersonal, institutional, or systemic level. These factors limited discussion of potential mechanisms underlying racial disparities, particularly how racism might operate at multiple levels (e.g., individual, institutional, and systemic) to produce health disparities among female veterans. Racial or ethnic disparities were reported more frequently for clinical and behavioral outcome measures (96%) versus process measures (65%). Below we summarize results by topic and type of measure. Notably, there was tremendous heterogeneity in terminology and categorization of racial and ethnic groups throughout the articles reviewed; when describing results in published articles, we have tried to stay consistent with terms used in the original articles; this includes terminology that is no longer widely accepted. However, we use the more widely accepted language when discussing and synthesizing findings.

PRISMA diagram of inclusions and exclusions.
Characteristics of Included Articles (n = 49)
Includes five articles with both process and clinical or behavioral outcomes.
VA, Veterans Health Administration.
Pregnancy
Table 2 details the articles addressing pregnancy by measure type (n = 21). Two articles are listed twice as they included both process and clinical or behavioral measures.45,46 Forty-three percent (n = 9) of the articles used data from the Center for Maternal and Infant Outcomes Research in Translation 39 study, a prospective cohort study that enrolled female veterans early in pregnancy.
Articles that Addressed Measures of Health Care Quality for Pregnancy, by Measure Type and Year
Used data from the Center for Maternal and Infant Outcomes Research in Translation (COMFORT) study.
Study included multiple types of measures.
aOR, Adjusted odds ratio ; COMFORT, Center for Maternal and Infant Outcomes Research in Translation study; EPDS, Edinburgh Postnatal Depression Scale; 95% CI, 95% Confidence Interval; PPA, Postpartum anxiety; PPD, Postpartum depression; PPPTSD, Postpartum posttraumatic stress disorder.
Pregnancy | process measures (n = 13)
Process measures examined included measures of patient-reported access, patient-reported and electronic health record-determined health care use, and measures of content and type of care. Patient-reported access measures included timely access to prenatal care (initiation before the end of the first trimester), 45 perceived timely access to prenatal care (got prenatal care as early as desired),39,45 access to mental health care during pregnancy, 45 and infant insurance coverage. 46 Measures of patient-reported health care use included intent to use VA care during pregnancy 40 and attendance at a 6–8-week postpartum visit, 45 whereas electronic health records were used to determine whether a veteran had a VA primary care visit in the 12 months postpartum. 42 In terms of content and type of treatment, measures included sufficiency of health information received during pregnancy, 44 receipt of an opioid prescription 38 or one for other risk medications during pregnancy, 43 and having a cesarean section versus a vaginal birth.41,45 Studies relying on patient-reported measures varied in terms of sampling frames (convenience versus population-based), study designs (prospective cohort versus cross-sectional survey), and population size.39,45 Not incorporated into any included study were measures of patient-reported experience, particularly measures of obstetric racism or mistreatment during birth, which in the general population are disproportionately reported by Black birthing people.57–59
Pregnancy | behavioral or clinical measures (n = 14)
A wide variety of maternal behavioral health measures were used, including perinatal depression symptoms;48,56 diagnosed perinatal depression, anxiety, or post-traumatic stress disorder;36,51 prenatal smoking;52,53 binge drinking during pregnancy; 37 and breastfeeding.45,50 Maternal clinical outcomes included preterm birth,45–47,55 nontraditional cardiovascular risk factors during pregnancy, 54 and severe maternal morbidity. 49 The only clinical infant measure reported was maternal report of low birth weight.45,46 Studies regarding racial disparities in behavioral and clinical measures varied widely in terms of how measures were operationalized, the population size, sampling frames, and operationalization of racial categories.
Contraception
Table 3 details the articles addressing contraception by measure type (n = 12). Fifty percent (n = 6) of the articles relied on data from the Examining Contraceptive Use and Unmet Need, a national cross-sectional survey of a random sample of women veterans of childbearing age (18–45 years old). 72 Notably, the majority of these articles were conceived of and published prior to or in the midst of a paradigm shift in contraceptive care to an approach emphasizing patient-centered communication and an increasing understanding of the limitations of assessing pregnancy intention and harms of focusing solely on provision and uptake of long-acting reversible contraception.73–76
Articles that Addressed Measures of Health Care Quality for Contraception, by Measure Type and Year
Used data from the Examining Contraceptive Use and Unmet Need (ECUUN) study.
Contraception | process measures (n = 4)
Process measures related to contraception included self-reported preconception counseling regarding teratogenic medications, 61 receipt of any contraception 60 and type of emergency contraception as documented in the electronic health record, 63 and self-reported contraceptive preferences. 62 While not traditional process measures, findings regarding differences in contraceptive preferences by race provide important context for understanding findings regarding racial disparities for behavioral and clinical.
Contraception: behavioral or clinical measures (n = 8)
In terms of behavioral and clinical measures, there was an emphasis on contraceptive adherence, unintended pregnancy, and use of long-acting reversible contraception. Three separate articles used various electronic health record-based operationalizations of adherence,64–66 while one study examined self-report of lifetime history of unintended pregnancy, 71 and another looked at the use of an intrauterine device (IUD) or contraceptive implant at last intercourse. 69 Two separate studies focused on differences by race and ethnicity in contraceptive knowledge 67 and concordance between self-reported ideal contraceptive method and current method. 70 Finally, one study examined self-reported experiences of reproductive coercion. 68
Gynecology
Of the seven articles on gynecology, two addressed structural measures,77,78 and five addressed process measures (Table 4).79–83 None addressed behavioral or clinical measures. The majority of measures were derived from a combination of electronic health record data and VA organizational data.77,78,80,81,83 Exceptions included one article that relied on survey data 79 and a qualitative article based on semistructured interviews with Black veterans with symptomatic uterine fibroids. 82
Articles that Addressed Measures of Health Care Quality for Gynecology, by Measure Type and Year
Gynecology | structural (n = 2) and process (n = 5) measures
Structural measures included residing in a “gynecology desert” where the closest VA did not offer gynecological care and supply in the community was minimal 77 and having a hysterectomy at a VA site with organizational characteristics thought to promote access to minimally invasive hysterectomy. 78 In terms of gynecology process outcomes, all of the articles focused on hysterectomy or uterine fibroids,79–83 with all but one article 79 coming from a single research group. This was the only topic area that included a qualitative study. The single qualitative article focused on the experiences of Black veterans with uterine fibroids, highlighting challenges in receiving timely and appropriate uterine fibroid care, particularly if they wished to avoid hysterectomy. 82 These qualitative findings potentially provide additional context and explanation for results from the quantitative articles.
Reproductive health screenings, menopause, and infertility
Table 5 includes findings from other topic areas with fewer than five articles each, including reproductive health screenings (n = 3),84–86 menopause (n = 3),87–89 and infertility (n = 3).35,90,91
Articles that Addressed Measures of Health Care Quality for Reproductive Health Screenings, Menopause, and Infertility, by Topic, Measure Type, and Year
Study included multiple types of measures.
Reproductive health screenings, menopause, and infertility | process measures (n = 9)
Data on reproductive health screenings, including being up to date on cervical cancer screening or mammography 84 and frequency of screening for sexually transmitted infection (STI) screenings,85,86 were derived from electronic health records. Articles on menopause examined receipt of a prescription for hormone therapy (HT)87,89 and discontinuation of HT following publication of the initial findings from the Women’s Health Initiative study, which indicated that HT use was associated with increased risk for breast cancer and cardiovascular disease.88,92 Articles examining process measures related to infertility included receipt of infertility evaluation or treatment and highlighted challenges of comparing measures for infertility care derived from electronic health records versus survey data, as frequencies varied considerably depending on how these measures were operationalized.90,91
Reproductive health screenings, menopause, and infertility | behavioral or clinical measures (n = 4)
Articles in this category included one that measured diagnosed menopausal symptoms documented in the electronic health record 89 and three articles addressing infertility, including two using self-reported diagnosis of infertility35,90 and one that relied on documentation in the electronic health record. 91
Discussion
Using Donabedian’s model for the measurement of health care, 30 this scoping review examined racial and ethnic disparities in reproductive health care and outcomes among female veterans and found that, despite a growth in the literature, there were significant limitations in published data. A minority of studies included race or ethnicity as primary independent variables or explicitly mentioned racism. Fewer still provided any data or explanation for the mechanisms through which racism operated to generate the observed disparities. Additionally, almost no articles examined structural measures, and none included measures of systemic racism. Significant topical gaps in the literature were identified, with few articles that addressed reproductive health screening, menopause, or infertility and none that examined racial disparities related to breast or gynecological cancer, sexual function, or pelvic floor disorders, reflecting overall gaps in the literature with respect to these topics and female veterans. 93 Finally, there was significant variation in study design and operationalization of outcome measures across all topics.
VA studies examining a variety of health care settings and specialties suggest that while the enhanced access to health care afforded to veterans in VA can reduce racial and ethnic disparities in process measures, racial and ethnic disparities in clinical outcomes are not necessarily reduced.94–96 Consistent with this literature, we found that across reproductive health topics, racial and ethnic disparities were less frequently detected for process measures versus clinical and behavioral outcome measures. While veterans using VA care have enhanced access due to minimum or no co-pays and travel assistance, access alone cannot undo the impact of a lifetime of exposure to structural and interpersonal racism or prevent harm due to biased or discriminatory treatment.9,57,97–100 Additionally, access is a multidimensional construct consisting of more than just financial facilitators or barriers and is distinct from utilization. 101 Thus, to more deeply examine potential racial disparities in process measures, studies are needed that operationalize measurement of access across multiple dimensions, such as temporal (are appointments available at conventional times) or cultural (trust in the health care system or providers), which likely vary by race and ethnicity. 101
Study findings also highlight the need to explore process measures in terms of patient preferences and experience, particularly to provide context and to identify culturally competent for racial and ethnic disparities in process and clinical and behavioral outcomes. For example, Black and Hispanic veterans, compared with White veterans, were less likely to have a documented contraceptive method and less likely to report using an IUD or implant at last intercourse.60,69 However, a separate article reported that Black and Hispanic veterans were more likely than White veterans to prefer nonhormonal methods and methods that also prevented STIs. 62 Veterans of minoritized racial and ethnic groups were also more likely than White veterans to report a mismatch between their ideal and current contraceptive method and had lower contraception knowledge scores. 67 Thus, inclusion of data on patient preferences and experiences suggests that access as measured by availability of a full range of contraceptive methods at every VA may be less of an issue than lack of access to culturally competent patient-centered care. Nevertheless, there was a significant gap in the literature regarding veterans’ preferences and experiences with VA reproductive health care, whether these varied by race/ethnicity, and how or if they impacted clinical and behavioral outcomes.
Strengths of this scoping review included a group of co-authors with expertise in reproductive health and women veterans’ health research, using an established set of search terms, and applying the Donabedian’s framework for measuring health care quality to inform the synthesis of results. However, several limitations are important to consider. Most articles did not include race or ethnicity as primary predictor variables; thus, models and study designs were not necessarily designed to specifically address issues of racial and ethnic disparities and health equity and may have had limited power to detect racial and ethnic disparities. Authors also frequently relied on categorizations such as “non-White” or “racial minority” rather than more specific groupings. Relatedly, the conceptualization of race or ethnicity and how it was incorporated into the analyses and discussion of results was frequently limited, with few studies explicitly addressing racism as a root cause or incorporating measures of structural, systemic, or interpersonal racism. Nearly all articles focused exclusively on veterans using VA care, limiting generalizability to the broader population of veterans. The majority of articles on contraception and pregnancy relied on data from two large VA studies. While these studies provide rich data sources for secondary analyses, they also have their own limitations, raising questions regarding the robustness of some findings, as was highlighted by conflicting results from studies using different methodologies or sampling frames. Additionally, no studies examined differences in racial and ethnic disparities in services provided by VA versus those purchased from the community. Finally, due to the heterogeneity in study measures and racial and ethnic group categorizations, the data were not well suited for quantitative synthesis or meta-analysis. Nevertheless, our findings in this review provide important information suggesting areas where VA may need to focus efforts to improve health equity in reproductive health care and where more research is needed.
Implications for equity
Concurrent with the growth in the female veteran population and increasing availability of reproductive health care in VA, there is a steady growth in the literature regarding racial and ethnic disparities in this care and outcomes.21,22,102 While not amenable to meta-analysis due to heterogeneity of outcome measurement, there is sufficient literature to warrant systematic reviews for some topic areas (e.g., contraception and pregnancy). Notably, much of this literature results from secondary analyses from a relatively small number of datasets, many of which were not explicitly designed to address questions of health equity. Thus, there is a need for multidisciplinary studies of reproductive health among female veterans that are intentionally grounded in principles and frameworks of health equity and engage with veterans to understand the causes of racial and ethnic disparities in reproductive health care and outcomes among veterans.103–107 Research is also needed that measures multidimensional aspects of access as well as veterans’ preferences and experiences. Findings from such studies can provide deeper understanding of racial and ethnic disparities in reproductive health care and outcomes among veterans and inform the development and testing of interventions to reduce or eliminate disparities.
Conclusions
Understanding the causes of racial and ethnic health disparities and their relationships with different measures of health care quality is essential for achieving health equity for female veterans. Despite the rapid growth in the literature regarding women veterans’ health, there are significant gaps in understanding racial and ethnic disparities in reproductive health and outcomes of women veterans and substantial heterogeneity in the literature in terms of study designs and how outcomes are defined and measured.
Footnotes
Acknowledgments
We would like to thank Dr. Elizabeth Yano for her work as PI of the VA Women’s Health Research Network, which made this article possible and all of the women veterans who have served our country and contributed to research.
Authors’ Contributions
K.S.M.: Writing—original draft (co-lead), data curation (co-lead), and writing—review and editing (co-lead). S.L.E., N.G., K.O.H., J.I., S.S.I., K.A.K., Q.M., Y.I.N., D.Q., A.R., L.S., and K.C.S.: Data curation (equal) and writing—review and editing (equal). E.V.T.: Project administration (lead), data curation (equal), and writing—review and editing (equal). J.G.K: Conceptualization (lead), data curation (co-lead), writing—original draft (co-lead), and writing—review and editing (co-lead).
Disclaimer
The views expressed herein are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This work was supported by a grant from VA Health Systems Research (SDR 10-012), which funds the VA Women’s Health Research Network. D.Q. was supported by a VA HSR Career Development Award (CDA 20-224).
a
Given that sex refers to biology, and this review deals with preventive care and disease and treatment for female reproductive organs we use the term “female veterans” throughout this article rather than “women veterans.” Where possible, we have also used gender neutral terms.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.