
Abstract
Purpose:
While several tools measure organizational racial and ethnic equity and multiculturalism, no tool explicitly measures sexual orientation and gender identity (SOGI) equity.
Methods:
Using existing literature, 17 consultants spent 4 days drafting a survey, which was reviewed and edited by two LGBTQ+ (lesbian, gay, bisexual, transgender, and queer) community groups. A purposive sample of at least two people at 37 health and human service organizations were invited to complete the survey. Survey themes were created and questions were mapped to three categories of Internal Equity Coordination, Internal Policies and Education, and Program Development and Support. Descriptive statistics were performed (Stata, v.18).
Results:
We received 88 responses from 35 organizations. Sixty-one percent reported that their organization commits to diversity, equity, and inclusion work regardless of fluctuating finances. Sixty-nine percent agreed or strongly agreed cultural competency expectations did not disproportionately rest on lesbian, gay, bisexual, queer (LGBQ+), transgender, gender nonconforming, and nonbinary (TGNCNB), or Black, Indigenous, People of Color staff. Respondents reported that LGBQ+, TGNCNB, and racial equity were entrenched in their organizational culture (52%, 44%, and 37%, respectively). Respondents also reported that LGBQ+, TGNCNB, and racial equity were entrenched in their organizational policies (56%, 47%, and 48%, respectively). Respondents reported that LGBQ+, TGNCNB, and racial equity were entrenched in their organizational practices (53%, 45%, and 40%, respectively).
Discussion:
SOGI equity was more entrenched than racial equity in organizational policies, practices, norms, unwritten rules, and overall culture. While participants gave examples of equitable decisions and events, room for organizational equity improvement varied at the organizational level.
Introduction
Organizational cultural competency can be defined as “the ability to interact effectively and comfortably with people from different cultures.” 1 An organization’s level of cultural competency has both internal effects, on staff and volunteers, and external effects, on clients, patients, and community members. People from marginalized communities who come into contact with organizations that are not culturally responsive may be harmed by their interactions with these organizations.2,3
Several existing tools measure cultural competency, 1 cultural responsiveness, 2 multiculturalism,4–7 and/or health equity 8 within organizations. The majority of these tools focus on general organizational change or the health equity-related organizational capacity, and include only a few questions that are specific to sexual orientation or gender identity.2,4,5,9 We therefore sought to create a tool to measure organizational equity as it relates to sexual orientation and gender identity (SOGI), and race/ethnicity, to understand organizations’ principles, policies, and practices on cultural responsiveness to the lesbian, gay, bisexual, transgender, and queer (LGBTQ+) community.
Using existing tools for question ideas and a framework for LGBTQ+ equity in organizational change,2,6,10 we worked with LGBTQ+ consultants and community leaders to create a three-part survey that was sent to 37 New York State (NYS) health and human service organizations for staff completion. The survey included internal measures of equity that have the greatest impact on staff (e.g., staff diversity, decision making/power, anti-discrimination policies) as well as external measures affecting clients directly (e.g., pronoun use). The goal was to create a tool that would measure organizational cultural competency in terms of SOGI and race.
Methods
The LGBTQ+ Health Initiative grant
The LGBTQ+ Health Initiative is funded by the NYS Department of Health (DOH)’s AIDS Institute to offer technical assistance and capacity building to 37 health and human service organizations to improve their provision of multicultural and culturally responsive services to LGBTQ+ individuals and communities in NYS. This survey was developed to fulfill our objectives of conducting a formal assessment of the capacity of these organizations to provide culturally responsive services, creating individualized organizational plans that address the findings of the assessment, and providing technical assistance to address organizations’ demonstrated needs.
Community-based participatory research principles were used to underpin the project of developing and disseminating a survey, compiling and sharing results, and providing technical assistance to address identified gaps. The overall structure was to use existing literature measuring organizational change to provide fodder for survey questions. We then built a community of LGBTQ+ consultants who brought experiences measuring and leading organizational change together to create a “unit of identity” from which to build the survey, utilize “strengths and resources within the community” to choose foci of questions, and “facilitate co-learning and capacity building among all partners” by putting consultants into small groups to discuss and refine both survey foci and specific questions asked to measure them. 11
A literature search and the tool Dismantling Racism Works were used to identify existing surveys, the majority of which measured racial organizational equity, without a SOGI focus.1,2,4–7,9,10,12,13 Fortuitously, a recent publication conducted a nonsystematic literature review of the organizational change literature and proposed a conceptual framework for integrating SOGI concepts into organizational change. 10 It defined six concepts encapsulating “elements for success” (i.e., commitment to continuous learning, commitment to diversity and inclusion) and six concepts describing “process for success” (i.e., information exchange, relationship building). Due to the comprehensive nature of the conceptual framework, our team used it as the basis for this project’s survey development.
Survey creation
The goal of this survey was to assess the capacity of health and human service organizations to provide multicultural and culturally responsive services to the LGBTQ+ population and understand organizations’ educational, training, and capacity-building needs to inform our ongoing technical assistance offerings. The survey was intended to measure organizational equity in terms of SOGI, race, and ethnicity in organizations’ principles, policies, and practices.
The survey was developed through a three-phase process. In the first phase, a research team of three people (B.A.L., S.B.R.-M., J.M.) used a framework for implementing LGBTQ+ equity in organizations, focused on their six elements of success: Organizational Champions, Organizational Priority, Depth of Mission, Commitment to Continuous Learning, Commitment to Diversity and Inclusion, and Organizational Resources. 10 We sorted questions from two tools/surveys that measured organizational equity in terms of race and ethnicity and placed them under the most relevant of the six elements2,6 (Table 1).
An Example of How Existing Questions About Organizational Equity Were Adapted Into a Framework for Implementing LGBTQ+ Equity in Organizations, Using the “Element of Success for Organizational Champions” as an Illustrative Example
Wall and Obear. Multicultural Organizational Development (MCOD). Small Group Worksheet.
Wall and Obear. Multicultural Organizational Development (MCOD). Assessing Multicultural Organizations Worksheet.
In the second phase of survey development, we approached 25 consultants through personal and professional networks based on experience with professional leadership in NYS-based health and human service organizations, and/or their expertise in organizational change theory and measuring equity. We prioritized those with relevant lived experience: more than half of the consultants were Black, Indigenous, People of Color (BIPOC), and all but one identified as a member of the LGBTQ+ community. This resulted in 17 consultants (17/25 = 68%) drafting the survey through two in-person, 2-day summits, the first of which had seven participants and the second had 10 participants. Consultants were compensated for their time at an equity rate determined to be at market value for the field and location, regardless of educational background; healthy meals and snacks were provided during the summits in accordance with dietary needs.
Consultants worked in groups of two or three people to reflect on the definitions within the framework for implementing LGBTQ+ equity six elements for success. 10 The advantage of these smaller breakout groups was that each consultant had the opportunity to examine every question and element in depth, while still benefitting from peer collaboration, creative ideation, and diverse perspectives. 14 The consultant groups reviewed questions that research assistants had already categorized under each element, and added, moved, and removed questions and measures when appropriate. Then, the groups of consultants spent 30–45 min with each element, reviewing and sorting measures and questions from an additional six organizational change assessment tools.1,4,5,7,9,13 Next, the consultants were asked to narrow down each element by identifying where questions overlapped, to ensure that the questions in each element reflected both LGBTQ+ and racial equity. Consultants edited and refined language in each question for relevance and clarity.
Finally, consultants reconvened in the larger group to discuss what was missing from the survey. They moved away from the umbrella term of LGBTQ+ equity and added more specific sexual orientation and gender identity lenses to existing racial equity questions. We refined questions to explicitly capture differences between experiences of marginalized groups. As consultants reasoned, lesbian, gay, bisexual, and queer (LGBQ+)-friendly organizations did not always translate to transgender, gender nonconforming, and nonbinary (TGNCNB)-friendly organizations. For example, one open-ended question originally asked “What are examples of the organizational policies, practices, norms, unwritten rules, and overall culture?” In the final version of the survey, we divided this question into three matrix questions capturing differences between LGBQ+, TGNCNB, and racialized groups of people (Table 2).
An Example of How Consultants Divided Out an Existing Question on LGBTQ+ or Racial Equity to Better Understand the Nuances of Sexual Orientation, Gender Identity, and Race
Wall and Obear. Multicultural Organizational Development (MCOD). Small Group Worksheet.
Curry-Stevens, Reyres, and Coalition of Communities of Color. Protocol for Culturally Responsive Organizations. Domain 1: Commitment, governance, and leadership.
LGBQ+, lesbian, gay bisexual, queer; TGNCNB, transgender, gender non-conforming, nonbinary; CAB, Community Advisory Board.
In the third phase of survey development, we used the consultants’ edits, suggestions, and feedback to ensure questions were not repetitive and the survey was not prohibitively long, while still capturing an accurate picture of organizational equity in relation to SOGI and race. We shared the survey draft with two community groups for review, including a community advisory board (CAB) made up of 17 members of the LGBTQ+ community and a committee focused on cultural humility and racial justice (CHRJ) associated with The Lesbian, Gay, Bisexual & Transgender Community Center in New York City. Having community members involved with the creation of and review of research materials helped connect gaps between researchers and the population of interest—previous research has shown that community members have key information to share inherent to their position, can help provide perspective on substructures of the community that are critical to relevancy, and can make participants more comfortable with research by ensuring that the language used in research settings is familiar and relevant to the community. 14
Our CAB broke into groups of two or three people, and each group spent 45 min reviewing one of the three sections in the survey. CAB members were asked to fill out a form with the questions: “What items are unclear?,” “What is missing?,” and “What’s good about the survey?” and to note any changes to language and wording within the survey itself. We shared the updated survey with the CHRJ committee, who offered additional comments on a shared electronic document, including adding more instructions, adding definitions to specific terms such as “equity,” and wording changes. The final version of the survey was approved by the NYS DOH AIDS Institute.
The final electronic survey was hosted on the Research Electronic Data Capture Platform (REDCap). A purposive sample of employees from 37 NYS DOH AIDS Institute-funded health and human service organizations were sent an email including a link to complete the survey and additional directions. These organizations received 5 years of funding from the NYS DOH AIDS Institute to enhance LGBTQ+ focused services. We requested at least one staff member and one director/person in decision-making position complete the survey in order to capture a range of responses representing employees who do and do not have power to make changes regarding cultural competency and organizational equity. We followed up with organizations as needed via email and virtual meetings to promote recruitment. The information sheet at the beginning of the study highlighted the importance of anonymity in collecting candid data. Survey completion constituted informed consent.
Analyses
For analyses, Likert scale questions in Section 1 that ranged from “strongly disagree” to “strongly agree” were recoded as “strongly agree” = 4, “agree” or “This is true in policy and not yet in practice” = 3, “neutral” or “disagree” = 2, “strongly disagree” or “Don’t know” = 1, and “Not applicable” = 0. Pronoun questions in Section 1 were recoded as “yes always” or “yes” = 4, “sometimes” = 2, “no never” or “no” or “don’t know” = 1, and “not applicable” = 0. All variables in Section 2 had six answer options on a range from “Not yet thinking about this” to “This is entrenched across the organization.” They were recoded as “Not yet thinking about this” = 1, “Thinking about this” and “We are assessing this feature in our work” = 2, “We have an initial improvement effort underway” and “We have started to see benefits from implementing this approach/element” = 3, and “This is entrenched across the organization” = 4. All variables in Section 3 that were on a scale of 1–4 were kept or recoded to ensure that 1 was on the end of needing the most growth toward equity and 4 was having achieved the most equity.
While recruitment was ongoing, we worked with a group of six consultants (B.A.L., S.B.R.-M., B.B., F.E., L.B.S.) to create a process for analyzing the organizational-level results, prioritizing results presentation in a clear, concise, and helpful manner. Additionally, because we only required a minimum of two people from each organization to complete the survey, we were aware that confidentiality may be breached if we presented results for each question. To address these two issues, we categorized, grouped, and condensed questions together in a multistep process.
The concepts of equity committees, Board of Directors/executive/staff diversity, decision making/power, general cultural competency, mentoring, trauma informed care, anti-discrimination policies, practices/norms, internal staff development/training, and pronoun use were generated as topics from the organizational survey, which were then mapped to three terminal categories of Internal Equity Coordination, Internal Policies and Education, and Program Development and Support. These categories were created in discussion with our group of six consultants, and were selected to encompass all questions in the survey and represent both internal and external aspects of organizational policy, programming, power, and culture. Internal Equity Coordination included equity committees, Board of Directors/executive/staff diversity, decision making/power, and general cultural competency concepts. Internal Policies and Education included mentoring, trauma informed care, anti-discrimination policies, and practices/norms concepts. Program Development and Support included internal staff development/training and pronoun use concepts.
We then created a 4-point scale of “seed,” “seedling,” “budding flower,” and “full bloom” for each category, recognizing the equity path that organizations travel. We defined what results would look like at all levels of this scale, and created a table that presented aggregate organizational-level results to organizations (Table 3). The mean value of all answers to each question per three final categories was calculated and mapped to the final matrix before distributing to each organization. Specifically, a mean of “1.0” mapped to “seed,” mean of “2.0” mapped to “seedling,” mean of “3.0” mapped to “budding flower,” and a mean of “4.0” mapped to “full bloom.” Descriptive and bivariate statistics, comparing programmatic staff (program coordinator, director, administrator, educator, community outreach, and advocacy roles) and service-provision staff (physical health care, mental health care, and case/care manager roles), were performed in Stata, v.18, using chi-square tests for categorical variables and a p value of 0.05. Means and standard deviations (SDs) were calculated, using pairwise comparisons of means to determine within-group and between-group differences.
Results of Mean Organizational Equity Measures in Three Categories of Internal Equity Coordination, Internal Policies and Education, and Program Development and Support Were Mapped Onto a 4-Point Scale of “Seed,” “Seedling,” “Budding Flower,” and “Full Bloom” for Each Category, Recognizing the Equity Path That Organizations Travel
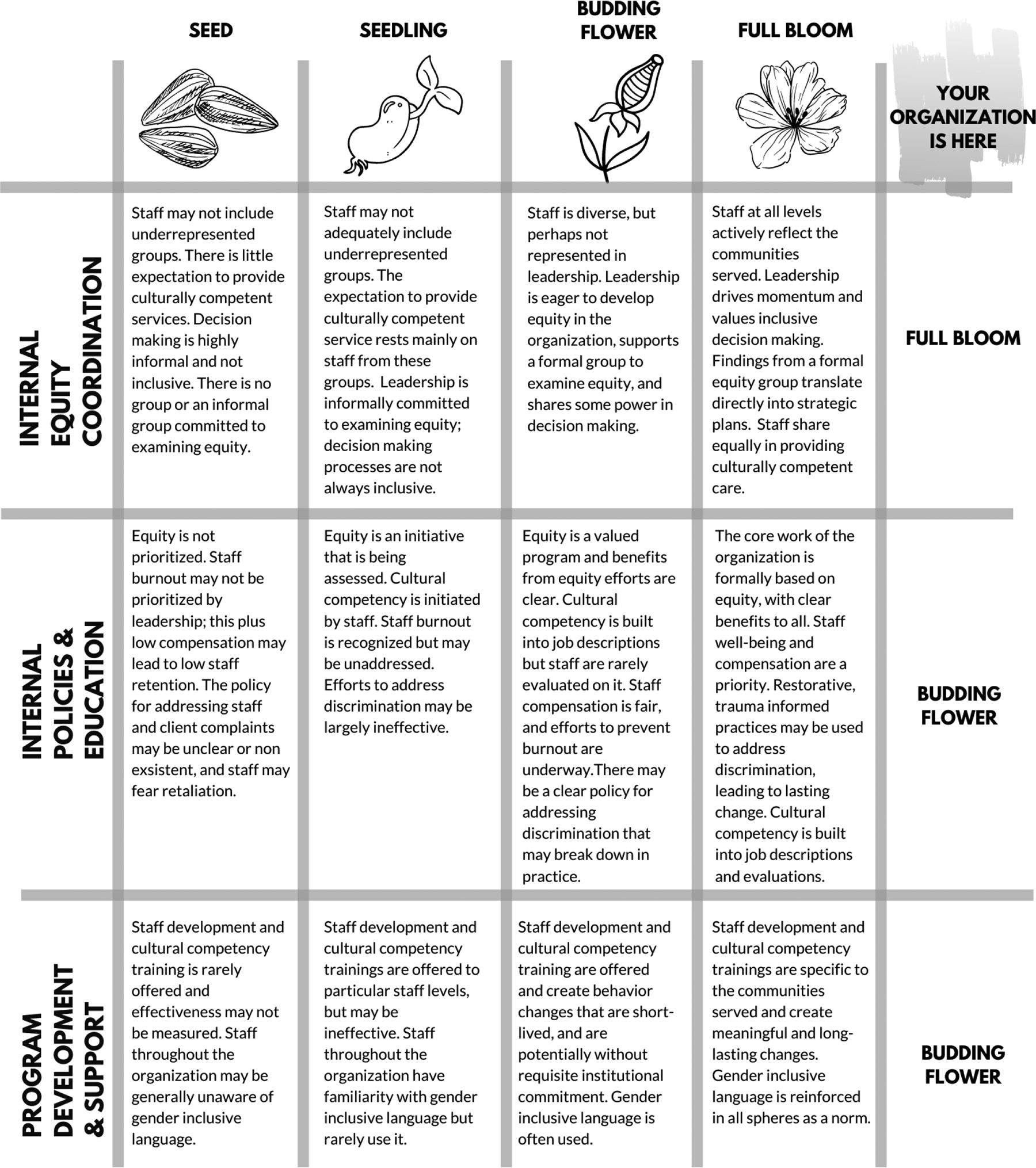
Organizations were presented this table of results.
Results
The final organizational equity survey included three sections. The first section grouped questions with a variety of different answer choices, including information about the respondent’s organization and role, yes/no questions, short answer questions, and Likert scale questions. To mitigate social-desirability bias and highlight our commitment to confidentiality of responses, we did not ask for the demographic information of the participants. Instead, we asked the employee role type to capture differences between internal facing and direct service roles.
The second section included a group of matrix questions on how the organization reflects LGBQ+, TGNCNB, and racial equity in policy, practice, norms, hiring and evaluation practices, staff training, equity committees, and trauma informed care. Respondents chose where their organization fits on a five-point range, from “not yet thinking about this” to “this is entrenched across the organization.” The third section asked respondents to identify an option from a list of four that best describes their organizations’ status or performance; some questions were also broken down to comparing marginalized groups to privileged groups (e.g., comparing LGBQ+ staff and heterosexual staff). Questions in this section asked about the Board of Directors, Executive leadership teams, decision-making frameworks, power and privilege, staff well-being, compensation, and staff development. The survey took participants about 45 min to complete.
We received 88 total responses to the survey, representing 35 NYS-based health and human service organizations. Of the individuals who responded, 34% were primarily in a director role in their organization, 18% were in a program coordinator role, 14% were in an administrative role, 9% were in physical or mental health care, and 23% had some other role. Participants had a range of experience in their positions: 13% had been in their role for less than 1 year, 34% between 1 and 3 years, 21% between 4 and 6 years, 6% between 7 and 9 years, and 26% had been in their role for 10 or more years.
The majority of participants (61%) agreed that there was a protected commitment at their organization for diversity, equity, and inclusion (DEI) work that occurred regardless of fluctuating financial resources, while 15% disagreed and 24% were unsure. Seventy percent of participants agreed or strongly agreed that the core work of their organization was based around social justice, respect, and solidarity, and the entire organization works to build a climate that promotes equity, while 15% disagreed, 11% were neutral or unsure, and 5% said this was true in policy and not yet in practice. The majority of participants (69%) agreed that the expectation to provide culturally competent or responsive services existed equitably for all staff and did not rest disproportionately on those who identify as LGBQ+/TGNCNB or as BIPOC, while 16% of respondents disagreed, and 17% were neutral or unsure. The majority agreed that their organization had a clear policy for and process to address staff (71%) and client (72%) complaints of discrimination, respectively (including micro-aggressions and behavioral patterns of exclusion and inclusion).
The majority of organizations reported that equity was entrenched across the organization in terms of culture, unwritten rules, norms, practices, and policies among the three main categories of sexual orientation, gender identity, and racial equity, though more SOGI equity was reported than racial equity (Table 4). Regardless of the category (LGBQ+, TGNCNB, racial) or organizational metric (policies, practices, norms), the mean response was 3.0, which translates to “We have an initial improvement effort underway and we have started seeing benefits.” Statistical differences were not found within-group (i.e., within LGBQ+, differences between policies, practices, and norms) or between-group (i.e., organizational policies across LGBQ+ vs. TGNCNB vs. racialized) comparison of means.
Responses (Categorical Percentages, Means, Standard Deviation) to Organizational Equity in Terms of Culture, Unwritten Rules, Norms, Practices, and Policies, Divided by the Main Comparison Categories of Sexual Orientation, Gender Identity, and Racial Equity, Among 88 Staff of 35 New York State-Based Health and Human Service Organizations, 2000
Of the 35 organizations who responded, 31 organizations had responses from at least two staff members, resulting in an organizational report of findings mapped to the matrix. The mean value across all organizations for Internal Equity Coordination was 2.8 (SD: 0.58), Internal Policies and Education was 2.9 (SD: 0.47), and Program Development and Support was 2.9 (SD: 0.36). All of these values mapped to the “budding flower” category on Table 3.
Bivariate analyses were conducted to determine if perceptions of organizational equity differed by organizational role, comparing internal facing roles (e.g., program coordinator, director, administrator) and service delivery roles (e.g., physical or mental health providers, case/care manager). Statistically significant results (p < 0.05) were found between these roles for defining equity within an organization, with more internal staff determining that equity is a core component of organizational structure.
Internal staff were significantly more likely to agree/strongly agree that the expectation to provide culturally competent services exists for all staff and does not disproportionately rest on LGBQ+, TGNCNB, or staff of color (78%) compared with those providing services (40%, p < 0.05). Statistically significant differences between internal/external roles were found for the reflection of LGBQ+ equity at organizational norms, unwritten rules, and cultural levels and the reflection of racial equity within organizational culture, with more internal staff reporting these concepts were entrenched across the organization (p < 0.05).
Significantly more service delivery staff felt there was a clear policy to address staff discrimination complaints, yet strongly disagreed they felt comfortable using the policy, compared with internal staff (p < 0.05). Statistically significantly more internal than external facing staff reported job descriptions reflected the need for LGBQ+, TGNCNB, and/or racial equity by including cultural competency values (46% and 26%, respectively, p < 0.05). More internal staff reported that there were transparent conversations about organizational power and privilege with different people involved in lasting change (43% vs. 35%, p < 0.05).
Concerning staff development, we compared opportunities for BIPOC staff with White staff, in which internal facing staff were statistically significantly more likely to report that staff development opportunities were offered with the same frequency between BIPOC and White staff (48%) versus external facing staff who were more likely to report staff development opportunities were rare (p < 0.05).
Organizations’ results and equity priorities were discussed during one-on-one organizational conversations, which led to the development and implementation of technical assistance and capacity-building opportunities to increase equity in terms of race, ethnicity, sexual orientation, and gender identity in organizations.
Discussion
Generally, equity around sexual orientation was the most entrenched in organizational policies, practices, norms, unwritten rules, and overall culture, followed by equity around gender identity. Similar research has shown that health care providers are significantly more comfortable and familiar with LGBQ+ needs than TGNCNB needs, pointing to a need for increased focus on TGNCNB cultural competency and equity. 15 Of the three marginalized communities, equity around race/ethnicity was the least entrenched in organizations, highlighting needed support.
Equity for SOGI and race does not occur in silos. Organization staff and clients have unique intersectional backgrounds, and are members of different communities that may affect individual needs and priorities.16–18 As there was no tool or survey that measured organizational cultural competency and equity and included SOGI along with race, we created this survey to improve our understanding of the nuances of organizational equity. We separated sexual orientation, gender identity, and race into separate categories to get differences of opinion; however, a limitation of this decision is that the survey does not capture the intersectionality and overlap of these lived experiences. Intersectionality highlights the overlapping and interdependent systems of discrimination that a person can experience due to multiple marginalized identities, including sexual orientation, gender identity, race, and ethnicity, plus education level, income level, health insurance status, (dis)ability, etc. 19 While the survey helped us understand which areas the organizations may need additional support, more work is needed to understand organizational equity at the intersections of identity.
Due to oppressive historical power structures, often the people in leadership roles are not individuals with marginalized identities, and may not see or be able to report on inequities within their organization, and/or be willing to enact changes that could undermine their own privilege. 20 Change agents, on the contrary, often have lived experience of being minoritized and must advocate for change from within structures that marginalize them. 21 However, having commitment from leadership is essential to create culturally competent and equitable organizations that dismantle structural racism.15,18,22 Therefore, we selectively sought responses from employees in both leadership and non-leadership roles in each organization in order to capture a more accurate picture of equity in the organizations. Leadership buy-in helps to ensure DEI initiatives are engrained into organizational culture by making it integral to the mission and outputs, 23 and make sure that staff at all levels are educated about and aware of supportive policies, and subsequently comfortable using the policies if needed. 15
When we introduced this survey, the research team was new to the coalition of organizations and had not yet established an ongoing relationship with organization representatives. In order to protect the privacy of the individuals who completed the survey, plus increase survey response and transparency, we did not collect demographic information. While this decision hopefully improved transparency in responses, we are also not able to analyze the results to determine if participants’ identities had an impact on their responses. Other studies that compared employee demographics and perceptions of cultural competency in their organizations, found respondents who identified as female, transgender, non-Hispanic Black or multiracial/ethnic, and LGBTQ+ report their organizations’ cultural competency to be significantly lower than White, cisgender, heterosexual men. 24 Collecting demographic data could help us stratify data in order to more effectively assess organizational culture.
Finally, as this was a pilot study, this survey requires additional psychometric testing across multiple leaders and organizations in order to establish reliability and validity. This survey may be useful to health and human service organizations undertaking strategic planning or change management processes, as it is intended to assess organizations’ capacity to provide multicultural and culturally responsive services to the LGBTQ+ population and understand organizations’ educational, training, and capacity-building needs. We suggest that organizations conduct this survey every 3–5 years, 25 based on individual needs and capacity. Not only does this timeline fit within similar governmental guidelines for community health assessments, 25 it gives organizations a chance to analyze results, implement interventions and changes, and allow for those changes to take effect, so that follow-up surveys can provide meaningful information on how organizational equity is changing.
Additionally, based on the limitations of our pilot study outlined above, we suggest that organizations planning to use this survey begin by involving existing equity committees, employee resource groups, and/or external consultants to help champion the survey and any additional work that builds from the results. These partnerships may help employees feel more comfortable completing the survey honestly than if the survey was to come directly from leadership or a human resources department. The more employees that complete the survey, the more accurate and representative the results will be for an organization. We suggest high numbers of total employees in an organization complete the survey, with a representative distribution across roles. As stated in our limitations, employees in leadership roles may not be as aware of equity imbalances, which may skew the final data toward the “full bloom” category if leadership is more represented in the results than other employees. Thus, we also suggest that organizations planning to use this survey first have a clear understanding and parameters for what roles are considered leadership for their specific organization.
This is the first survey that comprehensively assessed organizational equity in terms of race, sexual orientation, and gender identity, effectively separating out equity and discrimination within sexual orientation and gender identity, instead of combining the two groups into one LGBTQ+ collective. This separation allows for a deeper understanding of the equity needs for a collection of marginalized groups.
Conclusions
In order to offer effective and meaningful interventions that improve organizational equity and cultural competency, we need a clear understanding of how cultural competency in organizations may differ based on the identity of the population. This surSvey is the first to measure organizational cultural competency in relation to race and ethnicity as well as sexual orientation and gender identity, and provided the basis for 4 years of technical assistance and capacity-building interventions for these organizations. As organizations increase their equity, staff feel better equipped to provide culturally competent health and human services.
Footnotes
Acknowledgments
The authors wish to thank their Community Advisory Board, the NYS LGBT Network, and the following people for their contributions to this project: Katherine T. Acey, Katherine Chambers, J.D. Davids, Cecilia Gentilli, Cynthia Greenberg, Don Kao, Jarrett Lucas, Glenn Magpantay, Anthony Pena, Jessica Penaranda, Sharon Stapel, Sadé Swift, and Sean Thomas-Breitfeld.
Authors’ Contributions
B.A.L.: Conceptualization, funding acquisition, methodology, formal analysis, and writing–review and editing. S.B.R.-M.: Project administration, visualization, writing–original draft, and supervision. B.B.: Investigation, validation, and writing–review and editing. F.E.: Investigation, validation, and writing–review and editing. T.H.: Data curation and writing–review and editing. J.M.: Data curation and writing–review and editing. L.B.S.: Investigation, validation, and writing–review and editing. S.S.: Data curation and writing–review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was received from the New York State Department of Health AIDS Institute, Contract C33738GG (B.A.L., PI:URMC). The project described in this publication was supported by the University of Rochester CTSA award number UL1 TR002001 from the National Center for Advancing Translational Sciences of the National Institutes of Health. The project described herein was supported by the University of Rochester Office of Health Equity Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the New York State Department of Health AIDS Institute, or the University of Rochester.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.